Anatomy of the arm along with the nerves and their course
Reading File
Finding Sources
Finding Sources
Searching Images
arm anatomy nerves brachial plexus course diagram
Finding Sources
Finding Sources
Loading Image
Finding Sources
Loading Image
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
Loading Image
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive content from Gray's Anatomy for Students. Let me compile the full answer.
Anatomy of the Arm
Source: Gray's Anatomy for Students
Overview
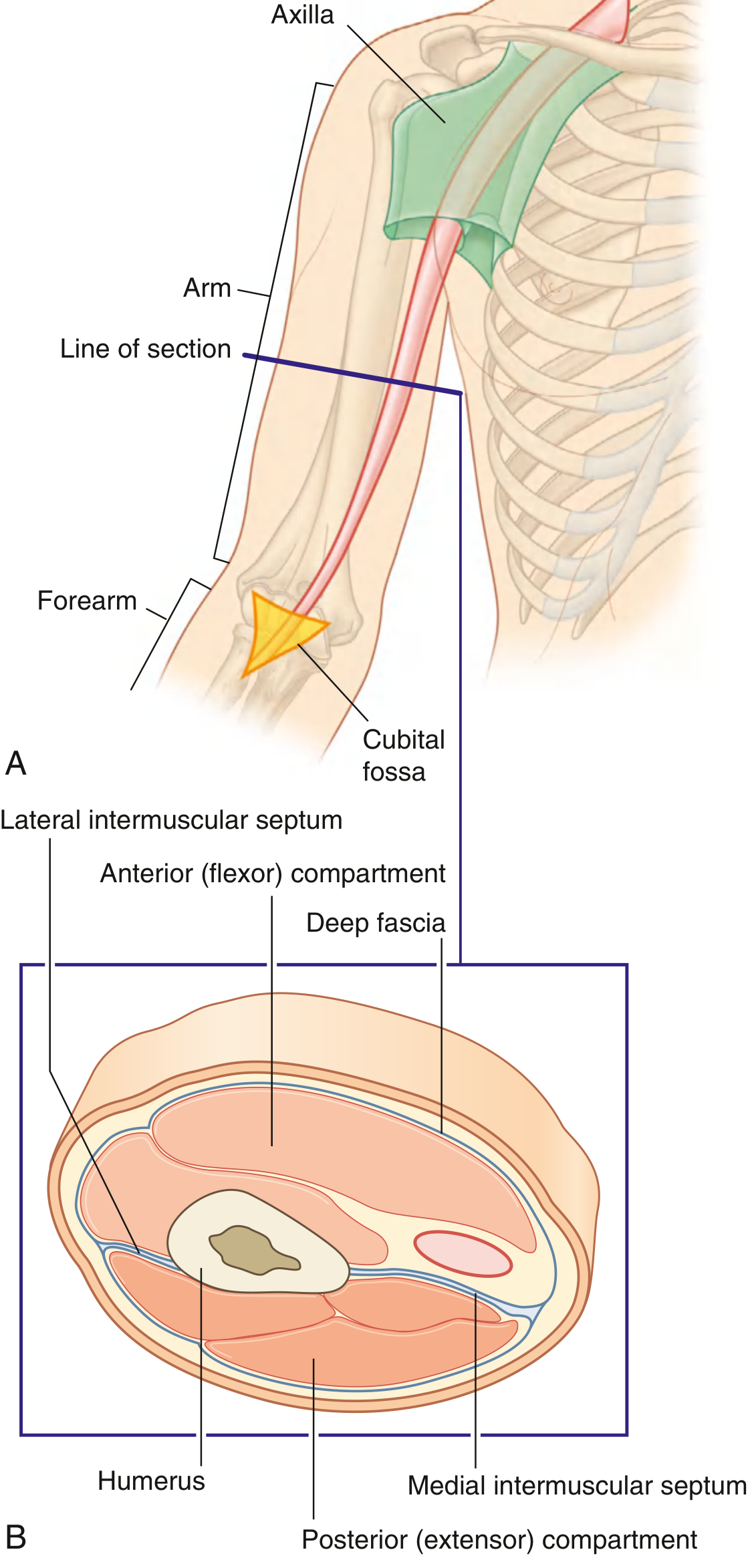
The arm is the region of the upper limb between the shoulder and the elbow. Its superior aspect communicates medially with the axilla; inferiorly, important neurovascular structures pass through the cubital fossa anterior to the elbow joint.
The arm is divided into two compartments by medial and lateral intermuscular septa, which pass from each side of the humerus to the surrounding sleeve of deep fascia:
- Anterior (flexor) compartment — muscles that flex the elbow
- Posterior (extensor) compartment — muscle that extends the elbow
Skeleton — The Humerus
The sole skeletal support of the arm is the humerus. Key surface landmarks relevant to nerves and vessels:
- Radial groove (spiral groove) — a shallow diagonal groove on the posterior surface that houses the radial nerve and profunda brachii artery
- Medial and lateral borders — attachment points for the medial and lateral intermuscular septa
- Lateral supraepicondylar ridge — attachment for brachioradialis and extensor carpi radialis longus
Muscles
Anterior Compartment
| Muscle | Origin | Insertion | Nerve | Spinal Level | Function |
|---|---|---|---|---|---|
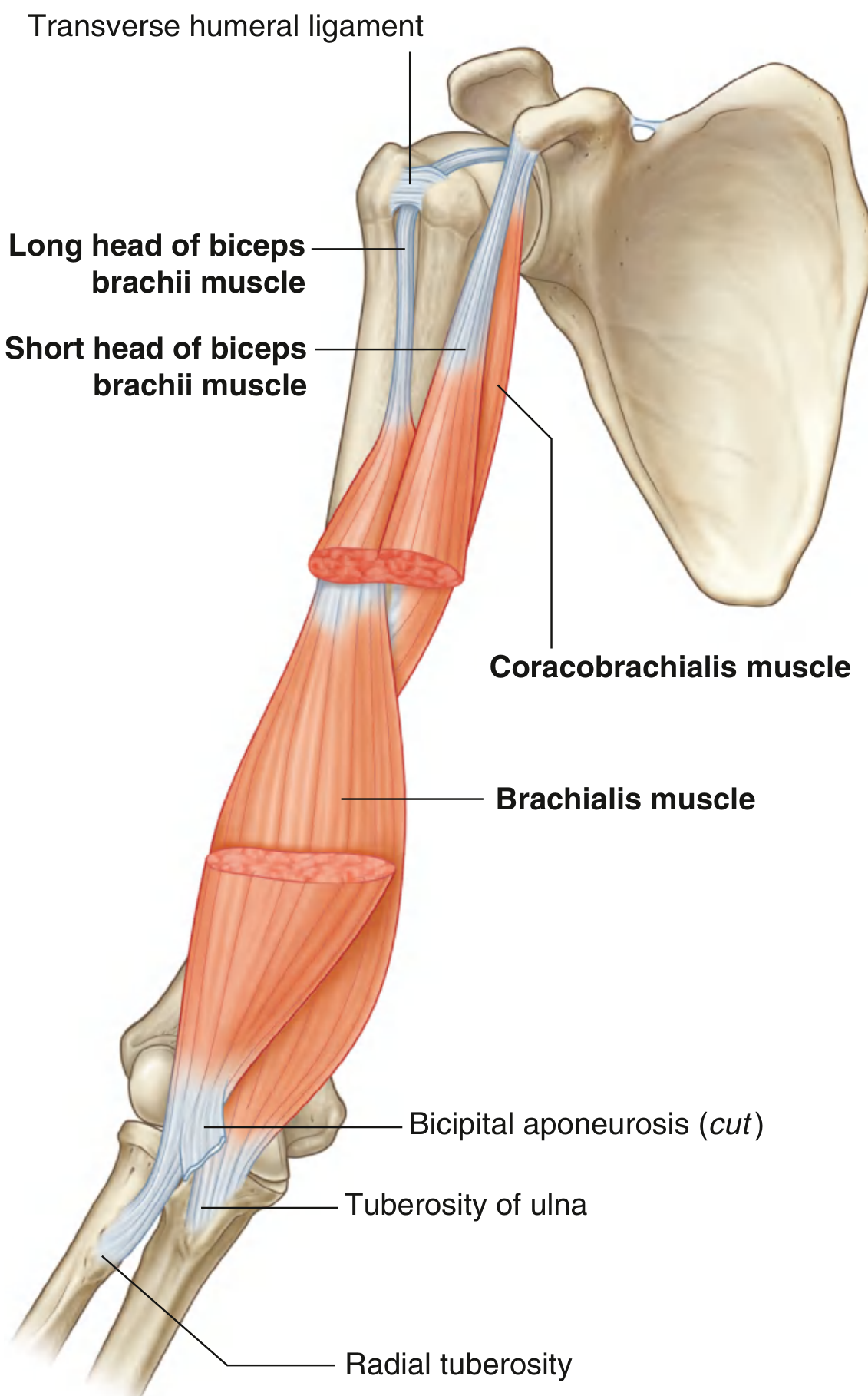
| Coracobrachialis | Apex of coracoid process | Medial midshaft of humerus | Musculocutaneous | C5, C6, C7 | Flexion of arm at glenohumeral joint |
| Biceps brachii | Long head: supraglenoid tubercle; Short head: coracoid process | Radial tuberosity + bicipital aponeurosis | Musculocutaneous | C5, C6 | Powerful elbow flexion + forearm supination |
| Brachialis | Anterior surface of humerus (medial & lateral surfaces) + adjacent septa | Tuberosity of ulna | Musculocutaneous (predominantly); radial nerve (lateral portion) | C5, C6 | Flexion of forearm at elbow |
Posterior Compartment
| Muscle | Origin | Insertion | Nerve | Spinal Level | Function |
|---|---|---|---|---|---|
| Triceps brachii | Long head: infraglenoid tubercle of scapula; Medial head: posterior humerus (below radial groove); Lateral head: posterior humerus (above radial groove) | Olecranon | Radial nerve | C6, C7, C8 | Extension of forearm at elbow; long head also extends and adducts at shoulder |
Nerves of the Arm
Five major nerves traverse the arm, all derived from the brachial plexus (C5–T1):
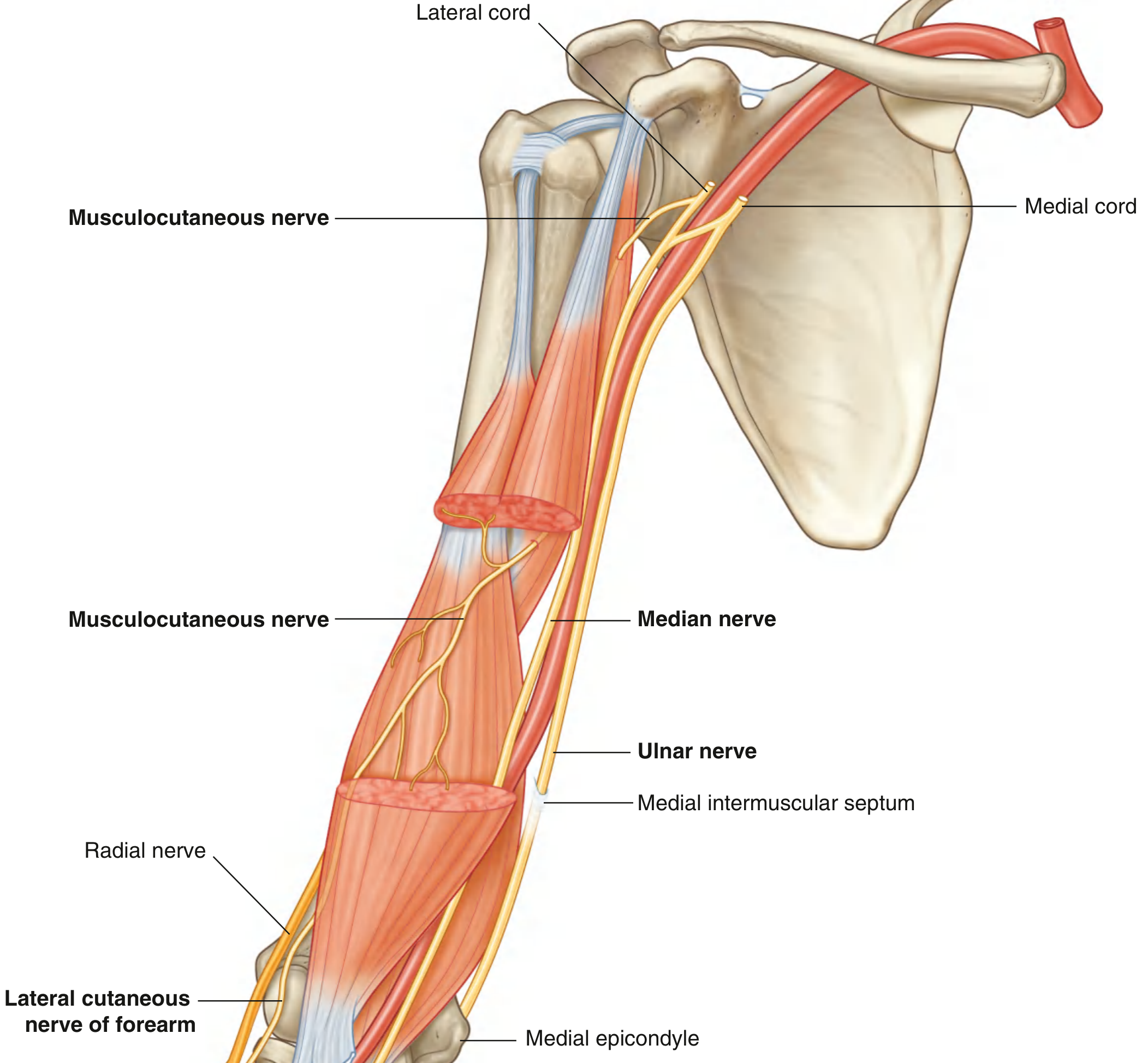
1. Musculocutaneous Nerve (C5, C6, C7)
Origin: Lateral cord of the brachial plexus
Course:
- Leaves the axilla and enters the arm by piercing the coracobrachialis muscle
- Passes diagonally down the arm in the plane between the biceps brachii and brachialis muscles
- Emerges lateral to the biceps tendon at the elbow
- Penetrates deep fascia → continues as the lateral cutaneous nerve of the forearm
Motor supply in arm:
- All three anterior compartment muscles: coracobrachialis, biceps brachii, brachialis
Sensory supply:
- Skin on the lateral surface of the forearm (as the lateral cutaneous nerve of the forearm)
2. Median Nerve (C6–T1)
Origin: Formed by union of lateral (C6, C7) and medial (C8, T1) cords
Course:
- Enters the arm at the inferior margin of the teres major muscle
- Runs vertically down the medial side of the anterior compartment
- Proximal arm: lies lateral to the brachial artery
- Distal arm: crosses to the medial side of the brachial artery
- Passes anterior to the elbow joint → enters the forearm
Branches in the arm: None of significance (a branch to pronator teres may arise just above the elbow)
Sensory: No cutaneous branches in the arm
3. Ulnar Nerve (C8, T1)
Origin: Medial cord of the brachial plexus
Course:
- Enters the arm with the median nerve and axillary artery, lying medial to the axillary artery in the proximal arm
- At mid-arm, it pierces the medial intermuscular septum → moves into the posterior compartment
- Lies anterior to the medial head of the triceps brachii
- Passes posterior to the medial epicondyle of the humerus (the "funny bone" groove)
- Enters the anterior compartment of the forearm
Branches in the arm: None
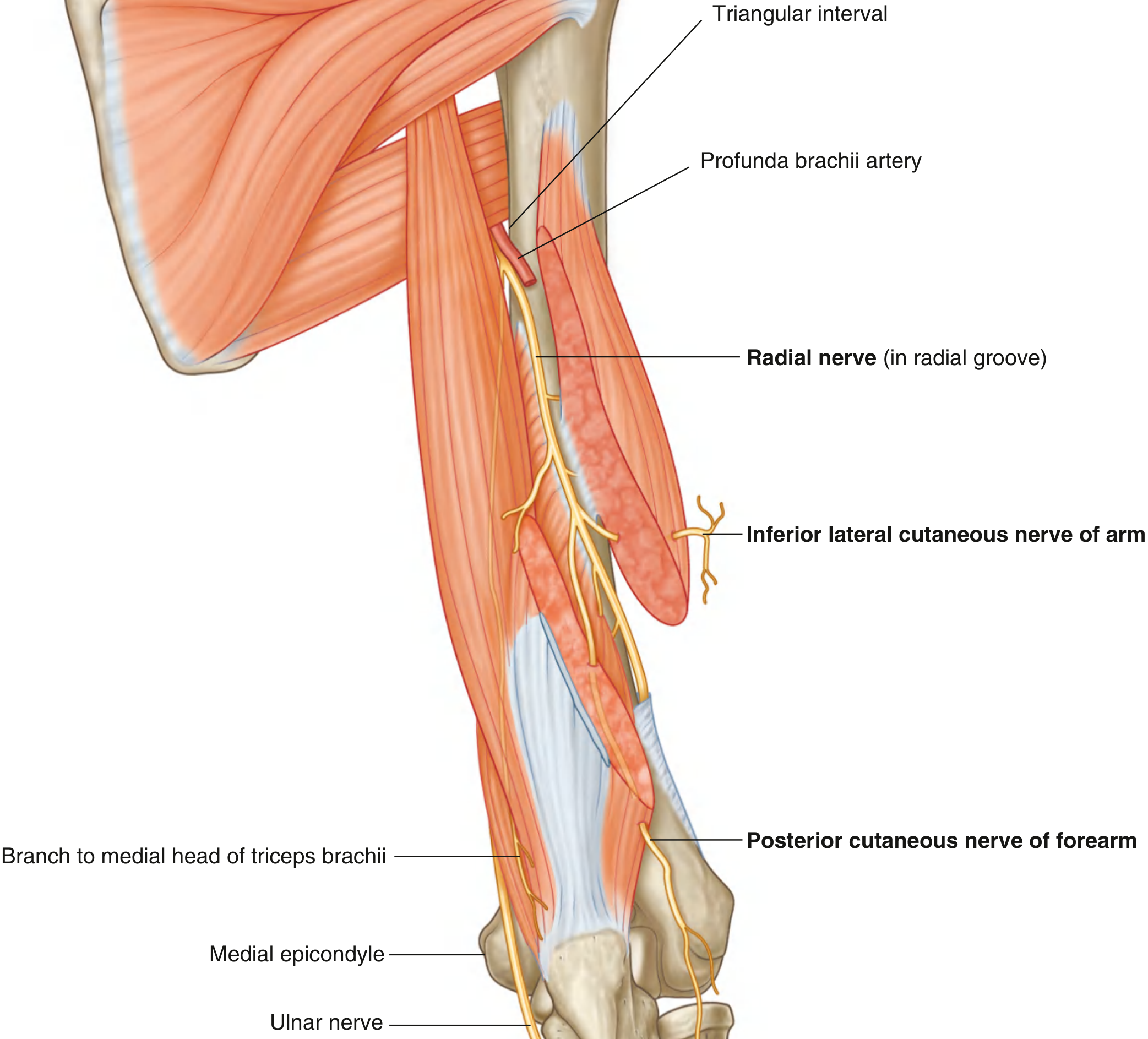
4. Radial Nerve (C5–T1)
Origin: Posterior cord of the brachial plexus
Course:
- Enters the arm by crossing the inferior margin of the teres major muscle, initially posterior to the brachial artery
- Accompanied by the profunda brachii artery, enters the posterior compartment via the triangular interval
- Passes diagonally (medial → lateral) through the posterior compartment, lying in the radial groove directly on bone
- Pierces the lateral intermuscular septum → enters the anterior compartment
- Lies between the brachialis (medially) and brachioradialis (laterally)
- Enters the forearm anterior to the lateral epicondyle, just deep to brachioradialis
Branches in the arm:
Motor:
- Triceps brachii (all three heads; the medial head branch arises before entering the posterior compartment and descends with the ulnar nerve)
- Brachioradialis
- Extensor carpi radialis longus
- Lateral portion of brachialis
Cutaneous:
- Inferior lateral cutaneous nerve of the arm — skin over the inferolateral arm
- Posterior cutaneous nerve of the forearm — skin over the posterior forearm
Both cutaneous branches penetrate the lateral head of triceps + overlying fascia to reach the skin.
5. Axillary Nerve (C5, C6)
Origin: Posterior cord of the brachial plexus
Course (passes through the arm's immediate proximal region):
- Exits the axilla posteriorly through the quadrangular space (along with the posterior circumflex humeral artery)
- Winds around the surgical neck of the humerus
- Supplies the deltoid and teres minor muscles + skin over the lateral shoulder (superior lateral cutaneous nerve of arm)
(Technically supplies structures at the shoulder but is relevant context because it branches just proximal to the arm.)
Brachial Plexus Architecture (Summary Diagram)
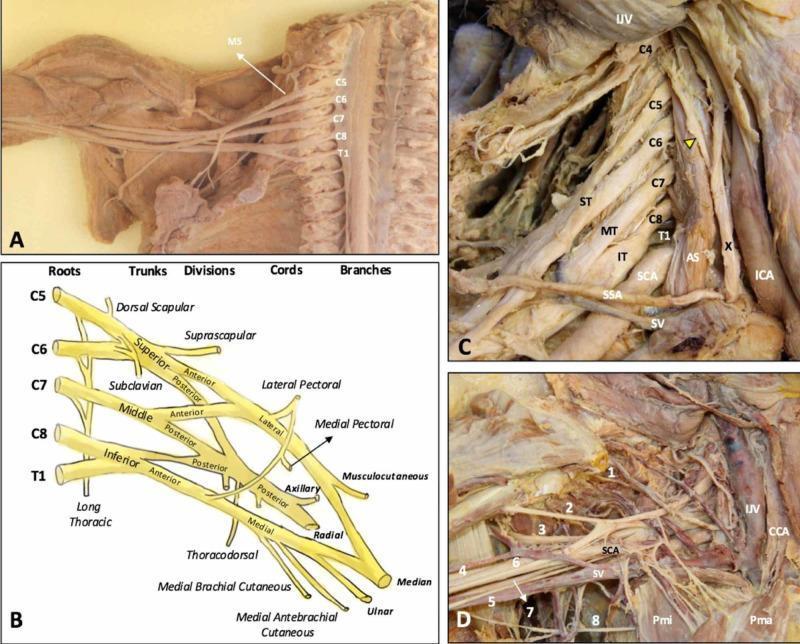
| Terminal Branch | Cord of Origin | Root Values |
|---|---|---|
| Musculocutaneous | Lateral | C5, C6, C7 |
| Median | Lateral + Medial | C6–T1 |
| Ulnar | Medial | C8, T1 |
| Radial | Posterior | C5–T1 |
| Axillary | Posterior | C5, C6 |
Arteries and Veins
Brachial Artery
- Begins as continuation of the axillary artery at the lower border of teres major
- Runs in the anterior compartment, moving from medial (proximal) to midline (distal)
- Terminates just distal to the elbow joint → divides into radial and ulnar arteries
- Key branch: profunda brachii artery — largest branch, enters the posterior compartment with the radial nerve through the triangular interval
Veins
- Brachial veins (deep, paired): flank the brachial artery
- Basilic vein (superficial): ascends medially, penetrates deep fascia mid-arm, joins the axillary vein
- Cephalic vein (superficial): ascends on the anterolateral arm → passes through the anterior axillary wall to the axillary vein
Clinical Correlates
Radial Nerve Injury (Midshaft Humerus Fracture)
The radial nerve is tightly bound with the profunda brachii artery in the radial groove. A midshaft humeral fracture can stretch or transect the nerve here, producing:
- Wrist drop — loss of wrist extension (paralysis of posterior forearm extensors)
- Sensory loss over the dorsum of the hand
Ulnar Nerve at Medial Epicondyle
As the ulnar nerve passes posterior to the medial epicondyle, it is superficial and vulnerable to trauma. Injury here causes:
- Loss of intrinsic hand muscle function (supplied in the forearm and hand)
- "Claw hand" pattern + sensory loss over the little finger and medial half of the ring finger
Musculocutaneous Nerve Injury
Rare in isolation; causes weakness of elbow flexion and loss of biceps/brachioradialis reflex + sensory loss over the lateral forearm.
Gray's Anatomy for Students, Chapter 7 (Upper Limb), pp. 870–882
Anatomy of forearm and nerves supply along with route
Finding Sources
Searching Images
forearm anatomy nerves median ulnar radial nerve course route diagram
Reading File
Finding Sources
Reading File
Loading Image
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
Reading File
Reading File
Finding Sources
Finding Sources
Loading Image
Loading Image
I now have comprehensive textbook content and diagrams. Let me compile the full detailed answer.
Anatomy of the Forearm
Source: Gray's Anatomy for Students, Chapter 7
Overview
The forearm extends between the elbow joint and the wrist joint.
- Proximally: most structures pass through the cubital fossa (anterior to the elbow). The exception is the ulnar nerve, which passes posterior to the medial epicondyle.
- Distally: structures pass through, or anterior to, the carpal tunnel. The exception is the radial artery, which passes dorsally around the wrist.
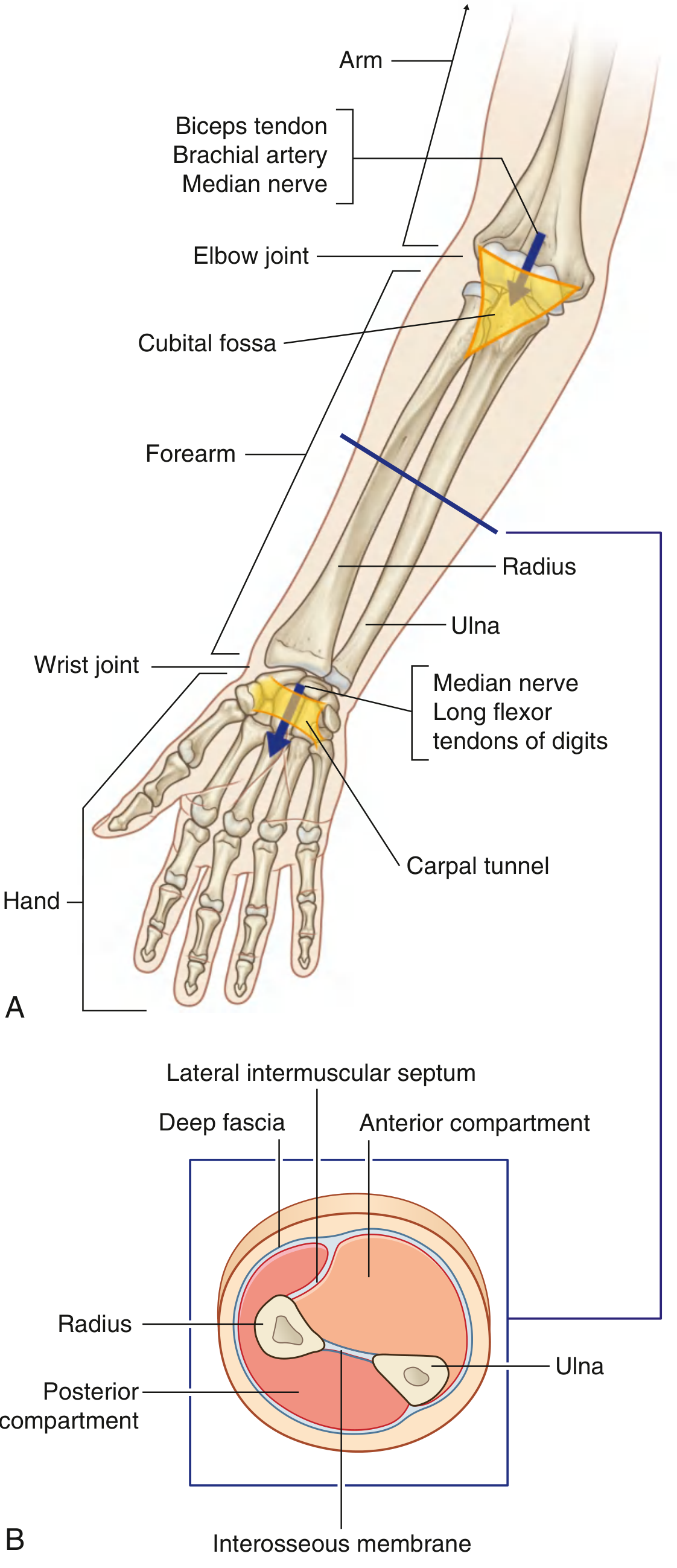
Skeleton
Two parallel bones form the framework:
| Bone | Position | Proximal Dimension | Distal Dimension |
|---|---|---|---|
| Radius | Lateral | Small (articulates with capitulum) | Large (forms wrist joint) |
| Ulna | Medial | Large (trochlear notch, olecranon) | Small (ulnar styloid) |
The interosseous membrane connects adjacent borders of radius and ulna and, together with the lateral intermuscular septum and deep fascia along the posterior ulnar border, separates the two compartments.
Compartments
| Anterior (Flexor) Compartment | Posterior (Extensor) Compartment | |
|---|---|---|
| Function | Flex wrist/digits, pronate | Extend wrist/digits, supinate |
| Nerve | Median + Ulnar (partial) | Radial nerve (all muscles) |
| Layers | Superficial, Intermediate, Deep | Superficial, Deep |
Muscles — Anterior (Flexor) Compartment
Rule: All anterior forearm muscles are innervated by the median nerve, except:
- Flexor carpi ulnaris (FCU) → ulnar nerve
- Medial half of flexor digitorum profundus (ring + little fingers) → ulnar nerve
Superficial Layer (all from medial epicondyle)
| Muscle | Insertion | Nerve | Level | Function |
|---|---|---|---|---|
| Pronator teres | Middle lateral surface of radius | Median | C6, C7 | Pronation; accessory elbow flexor |
| Flexor carpi radialis | Base of metacarpal II (± III) | Median | C6, C7 | Wrist flexion + abduction |
| Palmaris longus (absent ~15%) | Flexor retinaculum + palmar aponeurosis | Median | C7, C8 | Accessory wrist flexor |
| Flexor carpi ulnaris | Pisiform → hamate → metacarpal V | Ulnar | C7, C8 | Wrist flexion + adduction |
Intermediate Layer
| Muscle | Origin | Insertion | Nerve | Level | Function |
|---|---|---|---|---|---|
| Flexor digitorum superficialis (FDS) | Medial epicondyle (humero-ulnar head) + anterior radius (radial head) | Middle phalanges, digits 2–5 | Median | C7, C8, T1 | Flexes PIP and MCP joints of digits 2–5; accessory wrist flexor |
Deep Layer
| Muscle | Origin | Insertion | Nerve | Level | Function |
|---|---|---|---|---|---|
| Flexor digitorum profundus (FDP) — lateral half (index/middle) | Anterior + medial surface of ulna + interosseous membrane | Distal phalanges, digits 2–5 | Anterior interosseous nerve (branch of median) | C8, T1 | Flexes DIP joints |
| Flexor digitorum profundus (FDP) — medial half (ring/little) | Same | Same | Ulnar nerve | C8, T1 | Flexes DIP joints |
| Flexor pollicis longus | Anterior surface of radius + interosseous membrane | Distal phalanx of thumb | Anterior interosseous nerve | C8, T1 | Flexes thumb IP joint |
| Pronator quadratus | Anterior surface of distal ulna | Anterior surface of distal radius | Anterior interosseous nerve | C8, T1 | Pronation |
Muscles — Posterior (Extensor) Compartment
Rule: All posterior forearm muscles are innervated by the radial nerve (superficial branch/posterior interosseous nerve).
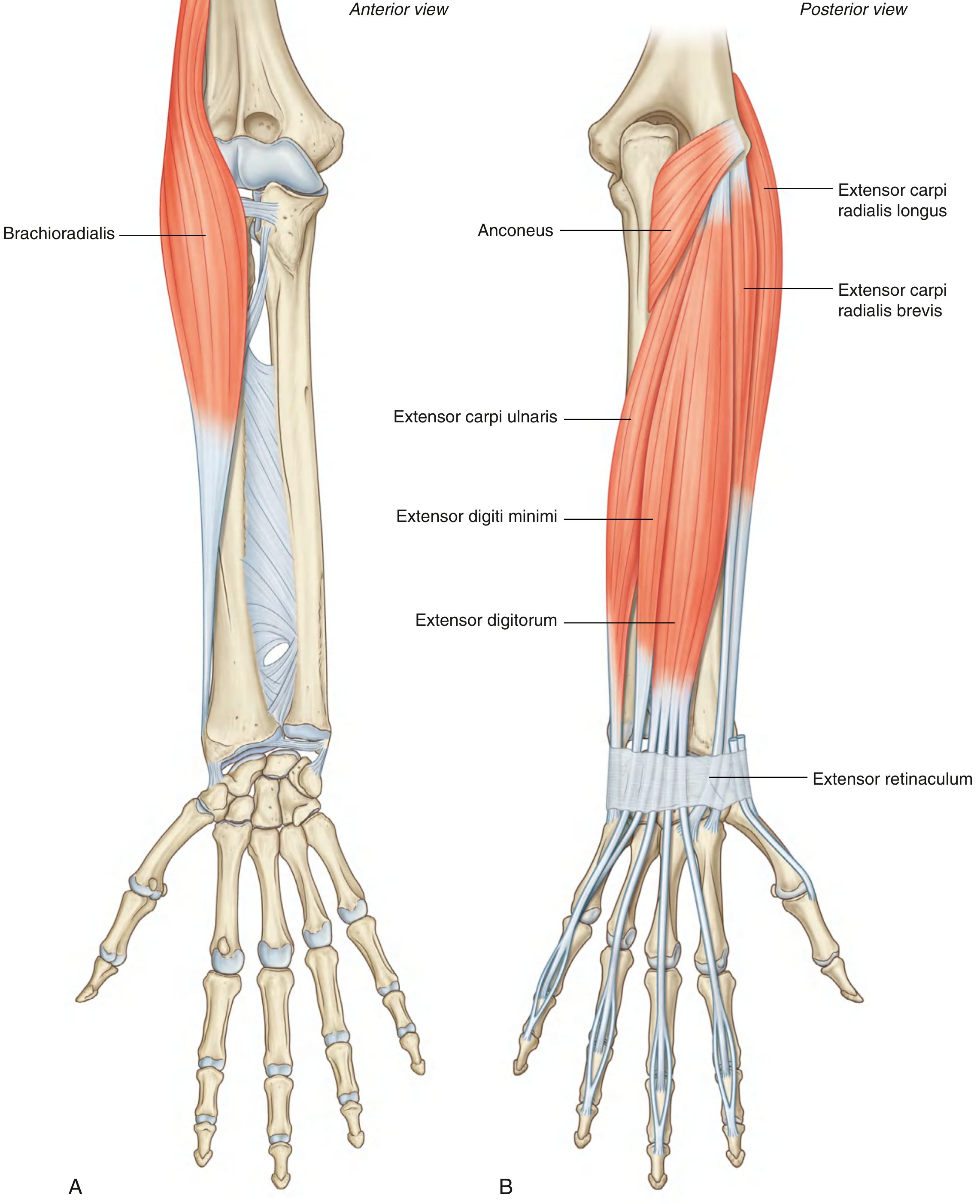
Superficial Layer (common origin: lateral epicondyle / supraepicondylar ridge)
| Muscle | Insertion | Nerve | Level | Function |
|---|---|---|---|---|
| Brachioradialis | Lateral distal radius (radial styloid) | Radial nerve (before bifurcation) | C5, C6 | Elbow flexion (accessory; strongest mid-prone) |
| Extensor carpi radialis longus (ECRL) | Base of metacarpal II | Radial nerve (before bifurcation) | C6, C7 | Wrist extension + abduction |
| Extensor carpi radialis brevis (ECRB) | Base of metacarpal III | Deep branch radial nerve | C7, C8 | Wrist extension + abduction |
| Extensor digitorum | Extensor hoods, digits 2–5 | Posterior interosseous nerve | C7, C8 | Extends digits + wrist |
| Extensor digiti minimi | Extensor hood of little finger | Posterior interosseous nerve | C7, C8 | Extends little finger |
| Extensor carpi ulnaris | Base of metacarpal V | Posterior interosseous nerve | C7, C8 | Wrist extension + adduction |
| Anconeus | Olecranon + posterior ulna | Radial nerve | C7, C8, T1 | Accessory elbow extensor |
Deep Layer
| Muscle | Origin | Insertion | Nerve | Level | Function |
|---|---|---|---|---|---|
| Supinator | Lateral epicondyle + radial collateral/anular ligaments + supinator crest of ulna | Lateral radius (superior to anterior oblique line) | Posterior interosseous nerve | C6, C7 | Supination |
| Abductor pollicis longus (APL) | Posterior ulna + radius + interosseous membrane | Lateral base of metacarpal I | Posterior interosseous nerve | C7, C8 | Thumb abduction |
| Extensor pollicis brevis (EPB) | Posterior radius + interosseous membrane | Base of proximal phalanx of thumb | Posterior interosseous nerve | C7, C8 | Extends thumb MCP joint |
| Extensor pollicis longus (EPL) | Posterior ulna + interosseous membrane | Base of distal phalanx of thumb | Posterior interosseous nerve | C7, C8 | Extends all thumb joints |
| Extensor indicis | Posterior ulna + interosseous membrane | Extensor hood of index finger | Posterior interosseous nerve | C7, C8 | Extends index finger independently |
Nerves of the Forearm
1. Median Nerve (C6–T1)
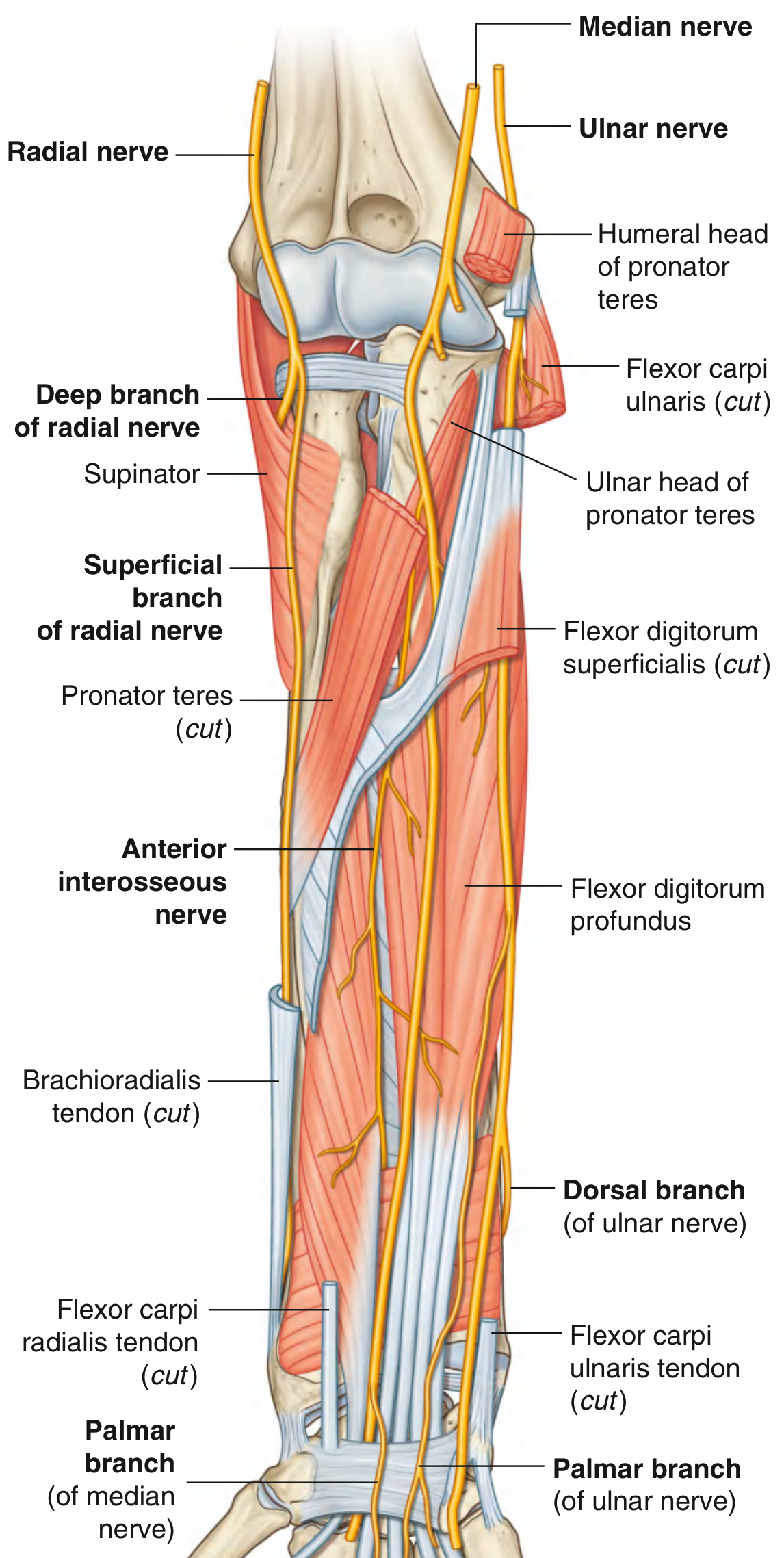
Entry: Leaves the cubital fossa by passing between the two heads of pronator teres (humeral + ulnar heads), then passes between the humero-ulnar and radial heads of flexor digitorum superficialis.
Course:
- Runs straight down the forearm in the fascial plane on the deep surface of FDS
- In the distal forearm, moves around the lateral side of FDS → becomes superficial between the tendons of palmaris longus (medially) and flexor carpi radialis (laterally)
- Exits the forearm through the carpal tunnel deep to the flexor retinaculum
Branches in the forearm:
| Branch | Course | Supply |
|---|---|---|
| Muscular branches | Arise just distal to elbow, medially from the nerve | Pronator teres, FCR, palmaris longus, FDS |
| Anterior interosseous nerve (AIN) | Arises between heads of pronator teres → descends with anterior interosseous artery along the interosseous membrane | FPL, lateral half of FDP (index + middle), pronator quadratus; terminates as articular branches to distal radioulnar joint and wrist |
| Palmar branch | Arises just proximal to flexor retinaculum → passes superficial to the retinaculum | Skin over base and central palm (spared in carpal tunnel syndrome) |
2. Ulnar Nerve (C8, T1)
Entry: Passes posterior to the medial epicondyle → enters the anterior forearm by passing through the triangular gap between the humeral and ulnar heads of flexor carpi ulnaris (FCU)
Course:
- Descends along the medial side of the forearm between FCU and FDP
- In the distal two-thirds, the ulnar artery lies lateral to the nerve
- Distally lies tucked under the anterolateral lip of the FCU tendon
- Exits by passing superficial to the flexor retinaculum, lateral to the pisiform bone
Branches in the forearm:
| Branch | Course | Supply |
|---|---|---|
| Muscular branches | Arise soon after entering the forearm | FCU + medial half of FDP (ring + little fingers) |
| Palmar branch | Arises in the middle of the forearm → passes superficially into the hand | Skin over the medial palm |
| Dorsal branch | Arises in the distal forearm → passes posteriorly deep to the FCU tendon | Skin over the posteromedial dorsum of hand + posterior surfaces of medial 1½ digits |
3. Radial Nerve — in the Forearm (C5–T1)
The radial nerve bifurcates into deep and superficial branches under the margin of brachioradialis in the lateral wall of the cubital fossa.
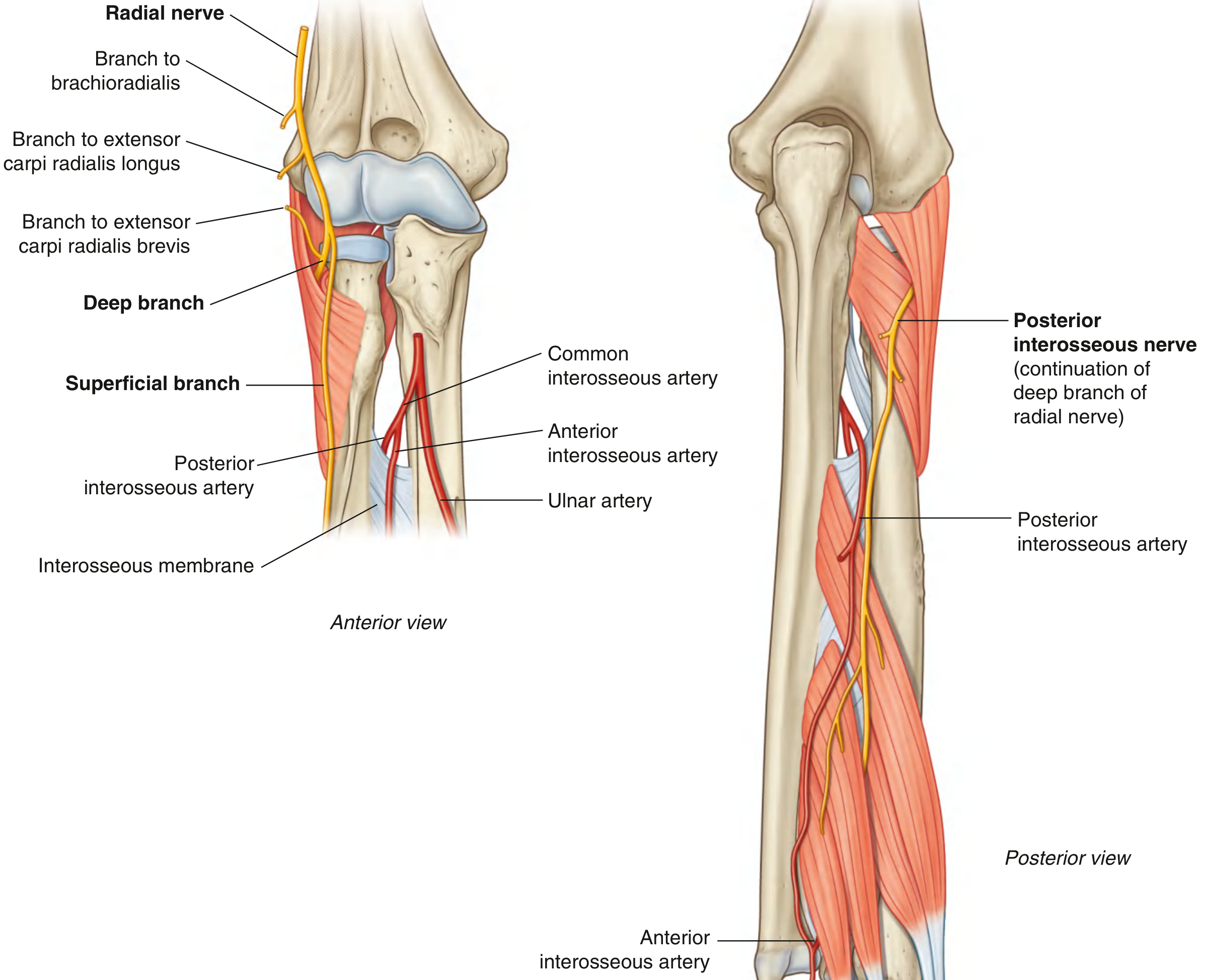
Before bifurcation (at cubital fossa):
- Branches to brachioradialis and extensor carpi radialis longus
A. Deep Branch (→ Posterior Interosseous Nerve)
Course:
- Originates in the lateral cubital fossa, deep to brachioradialis
- Innervates extensor carpi radialis brevis
- Passes between the superficial and deep layers of the supinator muscle, winding around the lateral aspect of the proximal radius
- Supplies supinator muscle during its passage through it
- Emerges from the distal edge of supinator as the posterior interosseous nerve (PIN)
- Lies between the superficial and deep layers of posterior forearm muscles
- Terminates as articular branches to the wrist, passing deep to extensor pollicis longus
Muscles supplied by PIN: extensor carpi radialis brevis, supinator, extensor digitorum, extensor digiti minimi, extensor carpi ulnaris, APL, EPB, EPL, extensor indicis
B. Superficial Branch
Course:
- Purely sensory
- Descends down the anterolateral forearm deep to brachioradialis, in close association with the radial artery
- Approximately two-thirds of the way down the forearm → passes laterally and posteriorly around the radial side of the forearm, deep to the brachioradialis tendon
- Enters the hand to supply skin over the posterolateral surface (dorsum of lateral 3½ digits to PIP level)
4. Lateral Cutaneous Nerve of the Forearm (C5, C6)
Origin: Continuation of the musculocutaneous nerve after it emerges lateral to the biceps tendon at the elbow.
Course: Pierces deep fascia lateral to the biceps tendon → descends superficially along the lateral forearm to the wrist.
Supply: Skin over the lateral surface of the forearm (both anterior and posterior aspects laterally).
Summary: Nerve Supply of the Forearm
| Nerve | Anterior Compartment Muscles | Posterior Compartment Muscles | Cutaneous |
|---|---|---|---|
| Median | Pronator teres, FCR, palmaris longus, FDS, FPL, lateral FDP, pronator quadratus | None | Skin of central/lateral palm (palmar branch) |
| Ulnar | FCU, medial FDP | None | Medial palm; posteromedial dorsum of hand (palmar + dorsal branches) |
| Radial | Brachioradialis, ECRL (before bifurcation) | All posterior muscles via PIN | Posterolateral dorsum of hand + lateral 3½ fingers (superficial branch) |
| Lateral cutaneous n. of forearm | None | None | Lateral forearm skin |
Arteries
| Artery | Course | Territory |
|---|---|---|
| Radial artery | Anterolateral forearm, medial to brachioradialis → passes dorsally around wrist | Radial side muscles; radial pulse lateral to FCR tendon |
| Ulnar artery | Medial forearm between FCU + FDP → enters hand lateral to pisiform, superficial to flexor retinaculum | Ulnar side muscles; dominant supply to palm via superficial palmar arch |
| Anterior interosseous artery | Anterior surface of interosseous membrane → perforates membrane distally | Deep anterior muscles; perforating branches to posterior compartment |
| Posterior interosseous artery | Passes over proximal interosseous membrane into posterior compartment | Superficial extensors; joins dorsal carpal arch |
Clinical Correlates
Anterior Interosseous Nerve (AIN) Palsy
Caused by fractures, penetrating wounds, forearm surgery, or tight cast. Loss of FPL + lateral FDP + pronator quadratus → inability to flex the IP joint of the thumb and DIP joint of the index finger → loss of the "OK sign" (pinch posture). No sensory deficit (AIN is purely motor).
Posterior Interosseous Nerve (PIN) Compression
The PIN can be compressed as it passes through the supinator muscle (arcade of Frohse). Results in weakness of finger/thumb extension with no wrist drop (ECRL is spared, as it is innervated before bifurcation) and no sensory loss (the superficial branch carries sensation).
Carpal Tunnel Syndrome
The median nerve is compressed under the flexor retinaculum. The palmar branch (arising proximal to the retinaculum, passing superficial to it) is spared, so thenar skin sensation is preserved while lateral 3½ fingers are affected.
Cubital Tunnel Syndrome
Ulnar nerve compression at the medial epicondyle/between the FCU heads. Results in weakness of intrinsic hand muscles (in addition to FCU + medial FDP), sensory loss over the medial 1½ fingers, and "claw hand" of the ring and little fingers.
Gray's Anatomy for Students, Chapter 7 (Upper Limb) — Forearm section, pp. 892–910
Flexor retinaculum
Finding Sources
Searching Images
flexor retinaculum carpal tunnel anatomy structures passing through diagram
Reading File
Reading File
Loading Image
Finding Sources
Loading Image
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Loading Image
Finding Sources
I now have all the content needed — two outstanding anatomical diagrams plus the full textbook text. Let me compile the complete answer.
Flexor Retinaculum
Source: Gray's Anatomy for Students, Chapter 7
Definition
The flexor retinaculum (also called the transverse carpal ligament) is a thick, strong band of connective tissue that bridges across the anterior aspect of the wrist, converting the concave arch of the carpal bones into the carpal tunnel — a fibro-osseous channel through which the long flexor tendons and median nerve pass from the forearm into the hand.
Attachments (4 bony points)
The retinaculum spans between the medial and lateral sides of the base of the carpal arch:
| Side | Bony Attachment |
|---|---|
| Lateral (radial) | Tubercle of the scaphoid + tubercle of the trapezium |
| Medial (ulnar) | Pisiform + hook of the hamate |
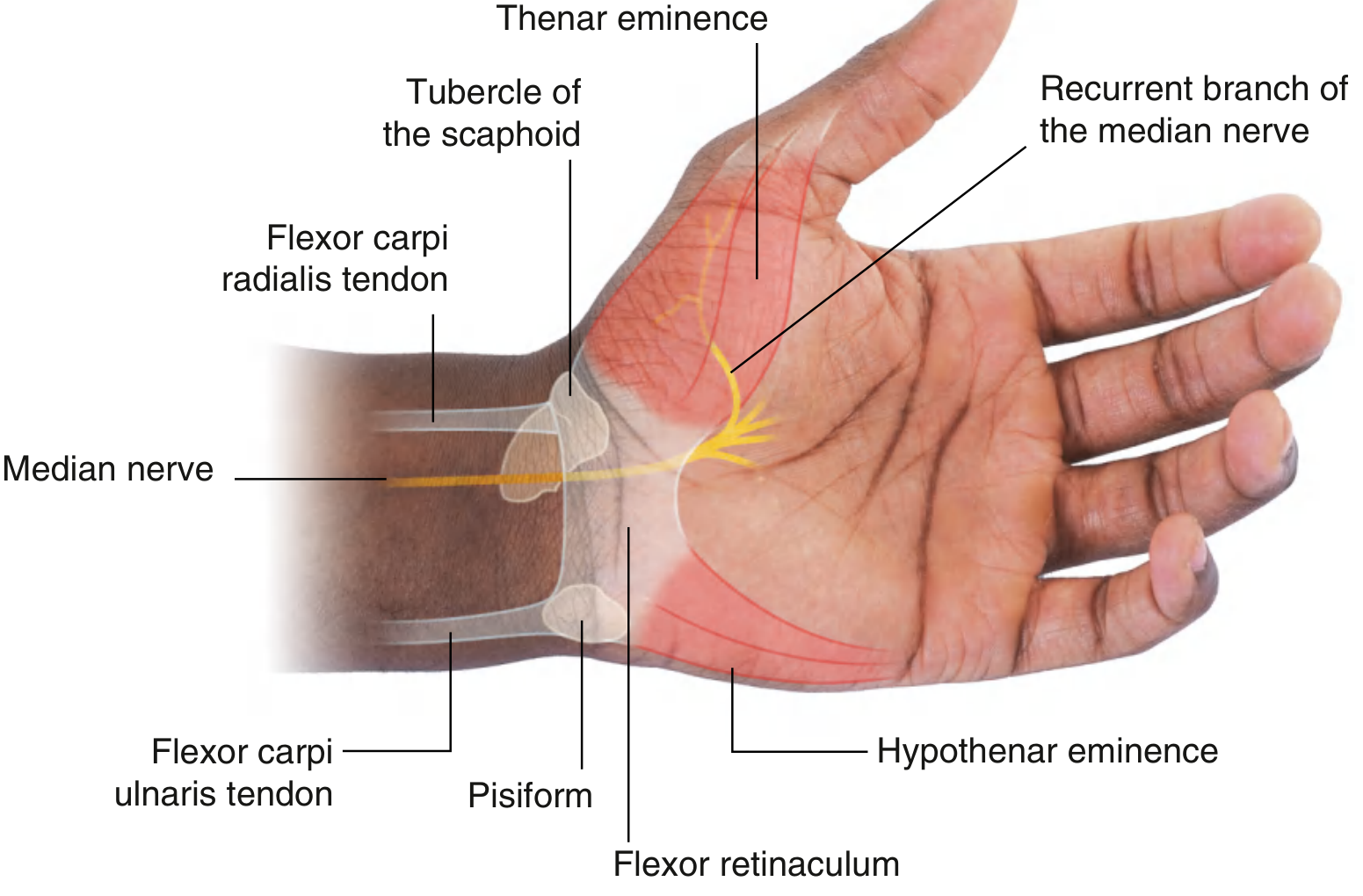
Surface Landmarks
- Proximal margin — an imaginary line between the pisiform (palpable at the distal end of the FCU tendon) and the tubercle of the scaphoid (palpable at the distal end of the FCR tendon)
- Distal margin — deep to the junction of the anterior margin of the thenar eminence and the hypothenar eminence, near the base of the palm
The Carpal Tunnel
The carpal arch (concavity formed by the carpal bones) + the flexor retinaculum anteriorly = the carpal tunnel.
- Roof (anterior wall): Flexor retinaculum
- Floor and sides: Carpal bones (scaphoid, lunate, triquetrum, pisiform, trapezium, trapezoid, capitate, hamate)
The retinaculum holds the tendons against the bony plane and prevents bowstringing during wrist flexion.
Contents of the Carpal Tunnel (9 tendons + 1 nerve)
Everything passing deep to (through) the flexor retinaculum:
| Structure | Notes |
|---|---|
| Flexor digitorum superficialis (FDS) tendons ×4 | Enclosed in a common synovial sheath with FDP |
| Flexor digitorum profundus (FDP) tendons ×4 | Enclosed in the same common synovial sheath as FDS |
| Flexor pollicis longus (FPL) tendon ×1 | Enclosed in its own separate synovial sheath |
| Median nerve | Positioned anterior to the tendons (most superficial structure in the tunnel) |
Total: 9 tendons + 1 nerve
Synovial sheaths around the tendons facilitate free gliding movement within the tunnel.
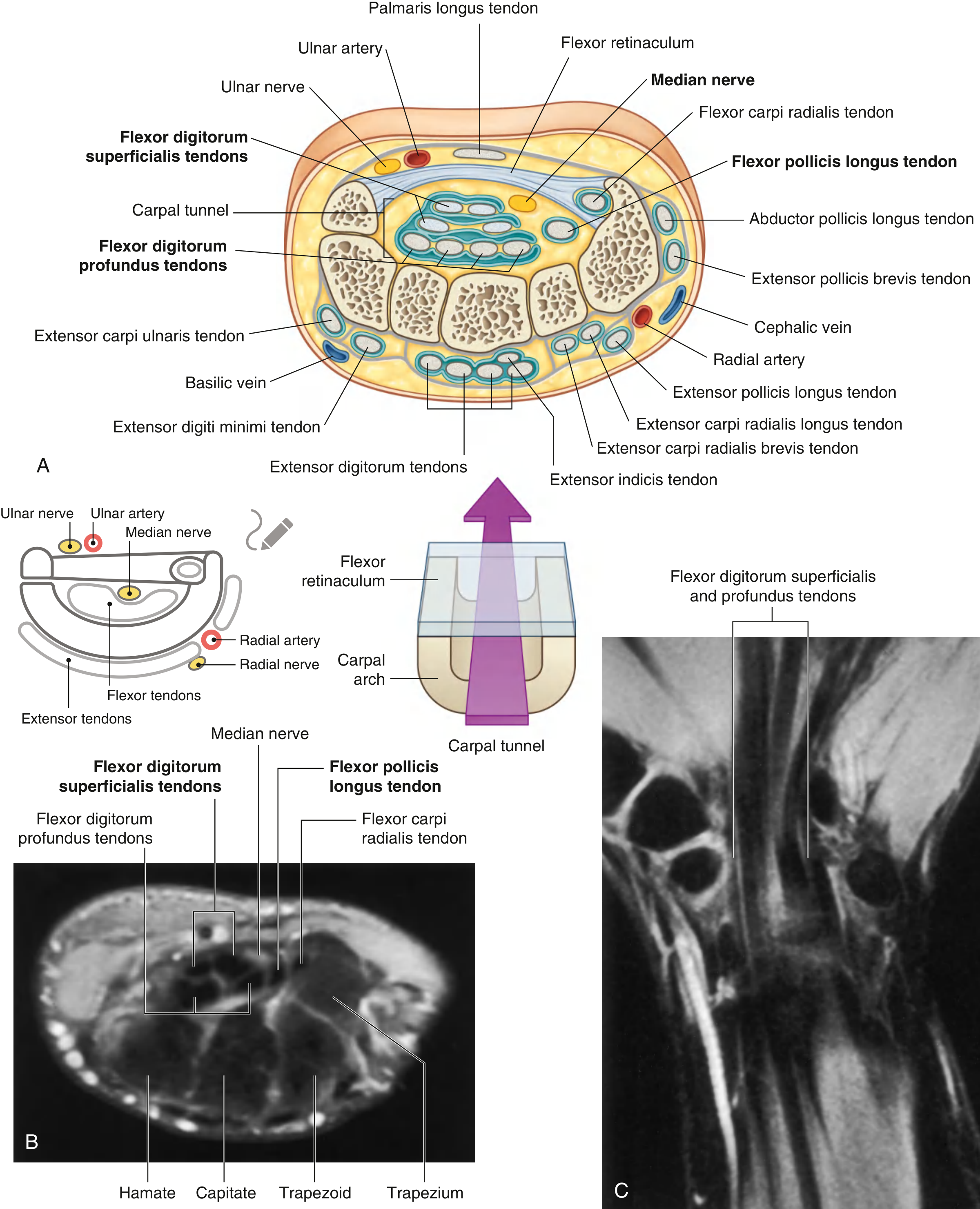
Structures Passing OUTSIDE (Superficial/Anterior to) the Retinaculum
These structures do not pass through the carpal tunnel:
| Structure | Position | Notes |
|---|---|---|
| Ulnar nerve | Anterior to retinaculum (Guyon's canal) | Passes lateral to the pisiform |
| Ulnar artery | Anterior to retinaculum | Lies lateral to the ulnar nerve |
| Palmaris longus tendon | Anterior to retinaculum | Not enclosed in a synovial sheath |
| Palmar branch of median nerve | Anterior to retinaculum | Branches from median nerve proximal to retinaculum; supplies skin over central/lateral palm — spared in CTS |
| Radial artery | Passes posterolaterally, dorsally around the wrist | Does not pass through carpal tunnel |
Special case — Flexor carpi radialis (FCR) tendon:
The FCR tendon does pass through a separate compartment formed by the lateral aspect of the flexor retinaculum folding around a groove on the medial side of the tubercle of the trapezium. It is enclosed in its own synovial sheath and is technically within the retinaculum, but outside the main carpal tunnel.
Muscular Attachments from the Retinaculum
The flexor retinaculum serves as the origin for the thenar and hypothenar muscles:
| Muscle Group | Muscles Originating from Retinaculum |
|---|---|
| Thenar muscles | Abductor pollicis brevis, flexor pollicis brevis (superficial head), opponens pollicis |
| Hypothenar muscles | Abductor digiti minimi, flexor digiti minimi brevis, opponens digiti minimi |
The palmar aponeurosis also has its apex continuous with the flexor retinaculum (when palmaris longus is absent, the aponeurosis anchors directly to it).
Recurrent (Motor) Branch of the Median Nerve
Immediately after emerging from the distal edge of the flexor retinaculum, the median nerve gives off its recurrent branch, which:
- Curves back (recurs) over the distal margin of the retinaculum
- Lies deep to skin and deep fascia over the anterior margin of the thenar eminence
- Supplies all three thenar muscles: abductor pollicis brevis, flexor pollicis brevis, opponens pollicis
- This branch is vulnerable during carpal tunnel release surgery — division causes permanent loss of thumb opposition
Clinical: Carpal Tunnel Syndrome (CTS)
Mechanism: Increased pressure within the carpal tunnel compresses the median nerve, causing venous congestion → nerve edema → ischemic axonal injury.
Common causes: Repetitive wrist use, rheumatoid arthritis (tendon sheath swelling), pregnancy (fluid retention), cysts from carpal joints, hypothyroidism, diabetes. In rare cases, a median artery variant may persist and run through the tunnel alongside the nerve.
Symptoms:
- Pain, paraesthesia ("pins and needles"), and numbness in the distribution of the median nerve — lateral 3½ fingers (thumb, index, middle, radial half of ring)
- Thenar wasting and weakness of pinch grip in advanced cases
- Tinel's sign: tapping over the flexor retinaculum reproduces symptoms
- Thenar skin is SPARED because the palmar branch of the median nerve branches proximal to the retinaculum and passes superficial to it
Treatment:
- Conservative: splinting, anti-inflammatory measures, corticosteroid injection
- Surgical: division of the flexor retinaculum (carpal tunnel decompression) — releases the roof, relieves pressure on the nerve
Summary Table
| Feature | Detail |
|---|---|
| Structure | Thick connective tissue band (transverse carpal ligament) |
| Lateral attachments | Tubercle of scaphoid + tubercle of trapezium |
| Medial attachments | Pisiform + hook of hamate |
| Forms | Roof (anterior wall) of the carpal tunnel |
| Contents of tunnel | FDS ×4, FDP ×4, FPL ×1 tendons + median nerve |
| Passes anterior to it | Ulnar nerve, ulnar artery, palmaris longus, palmar branch of median n. |
| Muscle origins | Thenar muscles + hypothenar muscles |
| Key nerve through it | Median nerve (compressed in carpal tunnel syndrome) |
| Key nerve from it | Recurrent branch of median nerve → thenar muscles |
Gray's Anatomy for Students, Chapter 7 (Upper Limb) — pp. 919–920
This is a shared conversation. Sign in to Orris to start your own chat.