Detail about pneumonia
"pneumonia" AND "management"
pneumonia overview etiology pathophysiology treatment 2025
Pneumonia - A Comprehensive Overview
Definition
- Textbook of Family Medicine 9e, p. 321
- Medical Microbiology 9e, p. 235
Classification
By Clinical Setting
| Type | Definition |
|---|---|
| Community-Acquired Pneumonia (CAP) | Develops in the outpatient setting or within 48 hours of hospital admission |
| Hospital-Acquired (Nosocomial) Pneumonia (HAP) | Develops >48 hours after hospital admission |
| Ventilator-Associated Pneumonia (VAP) | Occurs in mechanically ventilated patients |
| Aspiration Pneumonia | From aspiration of oropharyngeal or gastric contents |
| Pneumonia in Immunocompromised Host | Opportunistic organisms; distinct management |
By Pathogen Type
- Typical bacterial (e.g., Streptococcus pneumoniae, Haemophilus influenzae, Staphylococcus aureus)
- Atypical (e.g., Mycoplasma pneumoniae, Chlamydia pneumoniae, Legionella pneumophila)
- Viral (influenza A/B, RSV, SARS-CoV-2, CMV)
- Fungal (Pneumocystis jirovecii, Cryptococcus, Coccidioides)
By Anatomic Pattern
- Lobar pneumonia - consolidation of an entire lobe (classic in pneumococcal)
- Bronchopneumonia - patchy infiltrates around bronchi (common in children, elderly)
- Interstitial pneumonia - involvement of alveolar walls/interstitium (typical of viral and atypical organisms)
Epidemiology
-
Pneumonia/influenza is the primary diagnosis in over 1 million hospital admissions per year in the United States
-
In-hospital death rate: ~3.3%
-
Aggregate national hospital charges exceed $35 billion per year
-
Globally, it remains a leading cause of death, especially in low- and middle-income countries and in children
-
Children, elderly, and immunocompromised individuals are especially vulnerable
-
Textbook of Family Medicine 9e, p. 321
Etiology & Common Pathogens
Community-Acquired Pneumonia (CAP)
- Streptococcus pneumoniae - the most common cause of bacterial CAP and lobar pneumonia; declining in children due to vaccination
- Haemophilus influenzae - common in COPD, elderly
- Mycoplasma pneumoniae - classic "atypical" or "walking pneumonia"
- Chlamydia pneumoniae, Legionella pneumophila - atypical pathogens
- Respiratory viruses - influenza, RSV, SARS-CoV-2
Hospital/Nursing Home Patients
- Gram-negative rods: Serratia, Pseudomonas, Klebsiella, E. coli
- Anaerobes (aspiration)
- Multidrug-resistant (MDR) bacteria
Immunocompromised Patients
- Pneumocystis jirovecii (PCP) - especially in HIV/AIDS
- Cryptococcus, Coccidioides immitis
- Atypical mycobacteria, CMV, fungi
Special Populations
- Alcoholics: H. influenzae, aspirated anaerobes (Peptostreptococcus, Bacteroides)
- Neonates: Group B Streptococcus, gram-negatives, Chlamydia trachomatis (6-8 weeks)
- Children: Viral pathogens predominate; S. pneumoniae most common bacterial cause; S. aureus causes aggressive pneumonia post-varicella/measles
Pathophysiology
Entry & Early Infection
- Microaspiration of oropharyngeal secretions (most common)
- Inhalation of aerosolized particles
- Hematogenous seeding (rare)
Pneumococcal Pneumonia - Prototype
Hypoxemia Mechanism
- Shunt units (consolidated alveoli with no ventilation)
- Low V/Q regions
- Murray & Nadel's Textbook of Respiratory Medicine, p. 960
Clinical Presentation
Two Classic Patterns
- Abrupt onset, high fever (39-41°C) with shaking chills
- Productive cough - may have blood-tinged or rust-colored sputum
- Pleuritic chest pain
- Physical exam: decreased breath sounds, dullness to percussion, egophony on affected side
- WBC typically elevated (>15,000 x 10³/mm³) with neutrophil predominance
- Smoldering onset, low-grade fever
- Fewer constitutional symptoms
- Caused by Mycoplasma, Chlamydia, Legionella, or respiratory viruses
- Often called "walking pneumonia"
In Children
- Malaise, cough, chest pain, tachypnea (earliest clue - disproportionate to fever), intercostal retractions
- Viral: less toxic appearance, low-grade fever, wheezing
- Bacterial: appear acutely ill, high fever, chills, dyspnea
General Symptoms
Diagnosis
Chest X-Ray (CXR)

- Bacterial pneumonia: Lobar consolidation and alveolar infiltrates (radiographic changes lag 1-2 days behind clinical course; can be completely normal on day 1)
- Viral/atypical pneumonia: Patchy or streaky bilateral interstitial patterns + hyperinflation
- Parapneumonic pleural effusions may occur
Laboratory Tests
| Test | Use |
|---|---|
| CBC | Leukocytosis with neutrophilia (bacterial); normal/low WBC (viral) |
| Sputum Gram stain & culture | Low yield but may guide therapy |
| Blood cultures | Especially if bacteremia suspected |
| Legionella urinary antigen | High sensitivity for Legionella |
| Cold agglutinin test | Positive in Mycoplasma pneumoniae |
| AFB smear/culture | When TB is suspected |
| Procalcitonin & CRP | Biomarkers to distinguish bacterial vs. viral |
| Bronchoscopy/BAL | Reserved for immunocompromised, VAP, or non-resolving cases |
Severity Assessment Tools
- C - Confusion
- U - Urea >7 mmol/L
- R - Respiratory rate ≥30/min
- B - Blood pressure <90 systolic or ≤60 diastolic mmHg
- 65 - Age ≥65 years
Treatment
General Principles
- Treatment duration: minimum 5 days, and at least 48-72 hours beyond last fever/clinical instability
- Severity tools (PSI, CURB-65) should guide site-of-care decisions (outpatient vs. inpatient vs. ICU)
CAP - Outpatient (Mild, Healthy Adults)
- Amoxicillin OR
- Doxycycline OR
- Azithromycin/Clarithromycin (in areas with low macrolide resistance)
CAP - Inpatient (Non-ICU)
- Beta-lactam + macrolide (e.g., amoxicillin-clavulanate + azithromycin), OR
- Respiratory fluoroquinolone alone (levofloxacin, moxifloxacin)
CAP - ICU / Severe
- Beta-lactam + azithromycin or beta-lactam + respiratory fluoroquinolone
- Add MRSA coverage (vancomycin or linezolid) if MRSA risk factors present
HAP / VAP
- Broad-spectrum coverage targeting Gram-negatives and MRSA
- Agents: piperacillin-tazobactam, cefepime, or carbapenems ± vancomycin/linezolid
Atypical Organisms
- Mycoplasma/Chlamydia: macrolides or doxycycline
- Legionella: fluoroquinolones or azithromycin
Key Note
- Textbook of Family Medicine 9e, p. 322
Complications
| Complication | Notes |
|---|---|
| Parapneumonic effusion | ~25% of pneumococcal pneumonia; generally mild hypoxemia |
| Empyema | Purulent pleural effusion; rare but serious |
| Lung abscess | Uncommon in pneumococcal except serotype 3 |
| Bacteremia | Increases mortality, especially in elderly/asplenic |
| Respiratory failure / ARDS | Severe pneumonia with extensive consolidation |
| Pneumatoceles | Especially with S. aureus in children |
| Septic shock | Multi-organ dysfunction |
Splenic Dysfunction
Prevention
Vaccines
- Influenza vaccine: Annually for patients >50 years, those with chronic lung disease, diabetes, immune dysfunction, or other chronic organ failure
- Pneumococcal vaccine (PCV/PPSV23):
- Revaccinate after 10 years if the first vaccine was given before age 65
- Universal pneumococcal vaccination in children has significantly reduced S. pneumoniae CAP
Infection Control
- Hand hygiene, isolation precautions
- Head-of-bed elevation at 30-45° for ventilated patients (shown to reduce VAP risk)
- Oral care bundles in ICU patients
Summary Table
| Feature | Typical Bacterial | Atypical | Viral |
|---|---|---|---|
| Onset | Abrupt | Gradual | Gradual |
| Fever | High, with chills | Low-grade | Low-grade |
| Cough | Productive, purulent | Dry or mild | Dry |
| CXR | Lobar consolidation | Interstitial/patchy | Bilateral interstitial |
| WBC | Elevated, neutrophilia | Normal or mildly elevated | Normal or low |
| Common organisms | S. pneumoniae, H. influenzae | Mycoplasma, Legionella | Influenza, RSV |
- Textbook of Family Medicine 9e (Elsevier), pp. 321-323
- Medical Microbiology 9e, pp. 235-236
- Murray & Nadel's Textbook of Respiratory Medicine, p. 960
- IDSA/ATS Clinical Practice Guidelines for CAP (2019)
Tell me detail about LRTI . I am a respiratory medicine 1st year PGT
"lower respiratory tract infection" AND "guidelines"
LRTI lower respiratory tract infection classification etiology pathophysiology management guidelines 2024 2025
What This Covers (PGT Summary Map)
- Acute Bronchitis/Tracheitis - definition, viral etiology, why antibiotics are NOT indicated, stewardship
- CAP - full pathogens by setting, CURB-65, ATS/IDSA severe CAP criteria (with flowchart), antibiotic algorithm (outpatient → non-ICU → ICU → MRSA/Pseudomonas), 2026 ATS update
- HAP/VAP - CDC/NHSN VAE surveillance algorithm (VAC → IVAC → possible/probable VAP), organism resistance profile, 7-day antibiotic target, PK/PD dosing principles
- Aspiration Pneumonia and Lung Abscess - anaerobic microbiology, virulence factors, management
- Empyema - pathophysiology and management
- Diagnostics/Biomarkers - sputum quality, CRP-guided prescribing (NICE), procalcitonin, NGS
Key points to remember for exams:
- Acute bronchitis = no antibiotics (but 71% still get them - classic MCQ trap)
- CURB-65 score ≥3 = hospitalize; ATS major criteria (1 of 2) or minor criteria (3 of 9) = ICU
- HAP/VAP treatment = 7 days (not longer - more MDR with prolonged courses)
- Daptomycin is inactivated by pulmonary surfactant - cannot be used for lung infections
- Low procalcitonin does NOT rule out bacterial pneumonia - never withhold treatment on PCT alone
Tell me about Asthma in detail
"asthma" AND "management guidelines"
GINA 2025 2026 asthma guidelines update management
https://www.pulmonologyadvisor.com/features/asthma-gina-2026…
Asthma - Comprehensive PGT Guide (Respiratory Medicine)
1. Definition
Asthma is a disease characterized by episodic airway obstruction and airway hyperresponsiveness, usually accompanied by airway inflammation. In most cases, the obstruction is reversible, but in a subset of patients a component may become irreversible. In a large proportion, airway inflammation is eosinophilic, but some patients present with differing types (neutrophilic, mixed, or paucigranulocytic).
- Harrison's Principles of Internal Medicine 22E, Chapter 298
2. Epidemiology
- Affects ~300 million people worldwide; one of the most common chronic lung diseases
- Prevalence in adults: ~7-10% in high-income countries
- Increased prevalence with urbanization, Western lifestyle, obesity
- Can occur at any age; in children, more common in boys; in adults, more common in women
- Asthma deaths remain significant - GINA 2026 emphasizes fatality risk indicators as a new focus
3. Pathophysiology
3.1 Structural Changes in the Asthmatic Airway
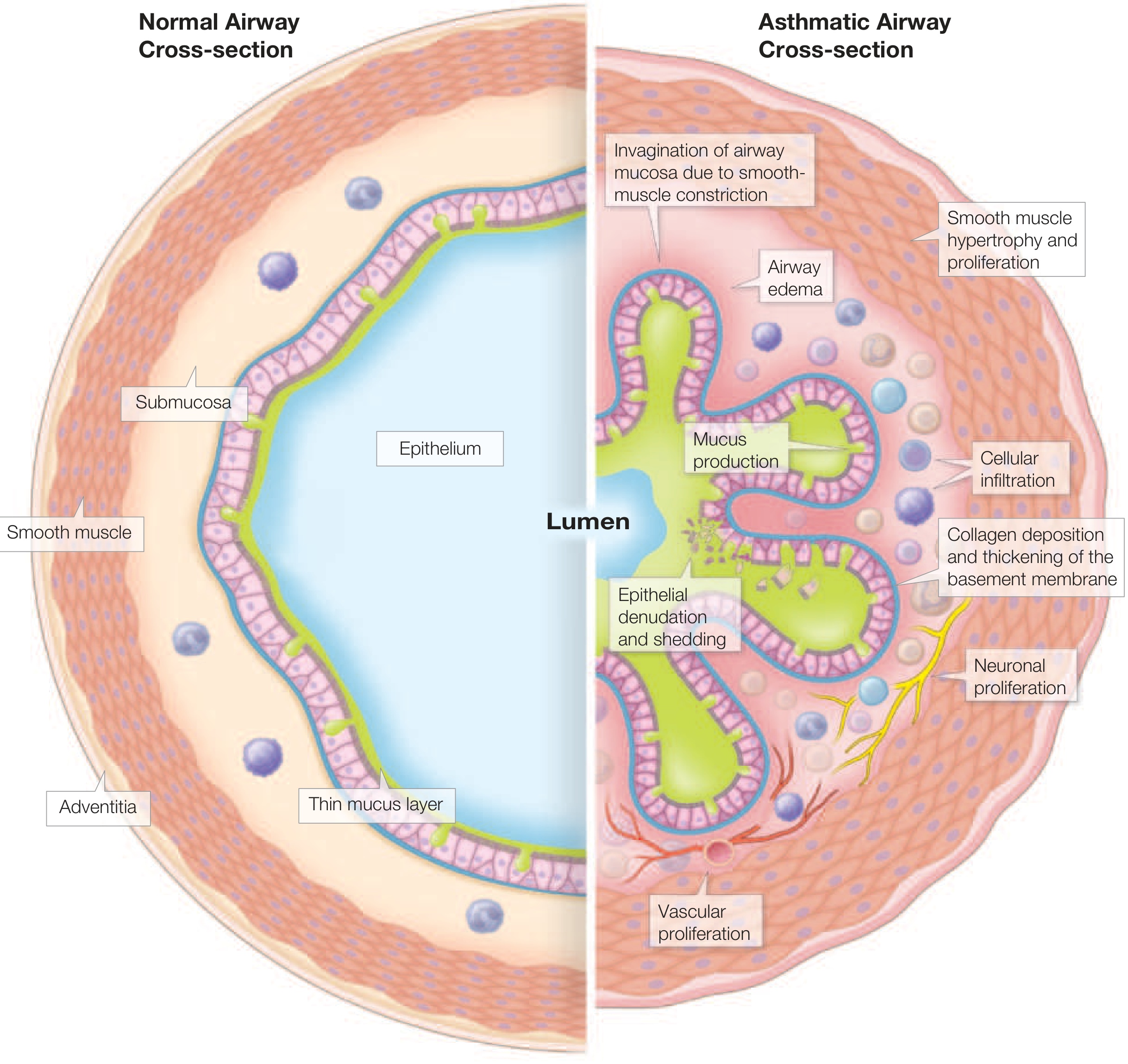
| Feature | Normal Airway | Asthmatic Airway |
|---|---|---|
| Smooth muscle | Normal | Hypertrophy and hyperplasia |
| Epithelium | Intact | Denudation and shedding |
| Basement membrane | Thin | Collagen deposition and thickening |
| Lumen | Open | Invagination of mucosa due to smooth-muscle constriction |
| Mucus | Thin layer | Mucus hypersecretion |
| Vasculature | Normal | Vascular proliferation (angiogenesis) |
| Innervation | Normal | Neuronal proliferation |
| Submucosa | Normal | Cellular infiltration + airway edema |
3.2 Airway Inflammation - Type 2 vs Non-Type 2
Type 2 (T2) Inflammation (most common, ~50-70%)
- Driven by: ILC2s (innate lymphoid cells type 2), Th2 lymphocytes
- Key cytokines: IL-4, IL-5, IL-13 (+ alarmins TSLP, IL-25, IL-33 from epithelium)
- Hallmark: Eosinophilic inflammation
- Elevated FeNO (fractional exhaled nitric oxide), blood and sputum eosinophilia
- Responds to: ICS, anti-IL-5 (mepolizumab, reslizumab, benralizumab), anti-IL-4Rα (dupilumab), anti-IgE (omalizumab), anti-TSLP (tezepelumab)
- Eosinophil products (ECP, major basic protein) cause airway hyperresponsiveness, mucus hypersecretion, and peribronchiolar collagen deposition
Non-Type 2 (T2-Low) Inflammation
- Neutrophilic: Associated with more severe asthma, smoking, obesity, occupational exposures; often steroid-resistant
- Paucigranulocytic: No obvious airway inflammation - often smooth muscle predominant
- Mixed granulocytic: Both eosinophils and neutrophils - often the most severe phenotype
3.3 Mechanisms of Airway Hyperresponsiveness (AHR)
- Structural: Airway wall thickening (smooth muscle hypertrophy + hyperplasia + subepithelial fibrosis) → disproportionate airway narrowing
- Inflammatory: Activated mast cells, eosinophils, T-cells release bronchoconstrictors (histamine, leukotrienes, prostaglandins)
- Neurogenic: Stimulation of sensory nerves → reflex bronchoconstriction
- Epithelial disruption: Epithelium-mesenchyme trophic unit → releases growth factors contributing to remodeling
- Lymphatics: Decreased lymphatic vessel density in fatal asthma → airway edema, fibrotic changes, despite elevated VEGF-C/D
3.4 Airway Smooth Muscle (Three Roles)
- Hyperresponsive to stimuli
- Hypertrophy + hyperplasia → airway wall thickening
- Produces chemokines/cytokines → promotes airway inflammation and mast cell survival
3.5 Subepithelial Changes (Remodeling)
- Thickening of the subepithelial basement membrane from deposition of:
- Repair-type collagens, tenascin, periostin, fibronectin, osteopontin
- Primarily from myofibroblasts under the epithelium
- Stiffens the airway, narrows the lumen, impairs relaxation → chronic airway obstruction
3.6 ICS Pharmacology - Key PGT Points
- ICS are the mainstay of maintenance therapy
- Corticosteroids reduce type 2 inflammation and airway hyperresponsiveness
- Oral bioavailability comparison (critical to reduce systemic side effects):
- Beclomethasone: ~20%
- Fluticasone: ~1%
- Mometasone: <1%
- Ciclesonide: Not activated until it deposits in lung tissue (pro-drug)
- Up to 80% of pMDI/DPI dose deposits in oropharynx - hence importance of low oral bioavailability
- Systemic effects of ICS: short-term growth suppression in children, decreased bone mineral density, possible increased cataracts
- Asthmatic airways have more proximal deposition of ICS (due to reduced airway caliber) → less systemic absorption than normal subjects
4. Classification / Phenotypes
GINA Severity Classification (Based on treatment step)
- Mild: Controlled on Step 1-2 (low-dose ICS or ICS/formoterol as-needed)
- Moderate: Controlled on Step 3 (low-dose ICS/LABA)
- Severe: Requires Step 4-5 or remains uncontrolled despite Step 4-5
Phenotypes (Clinical)
| Phenotype | Features |
|---|---|
| Allergic/Atopic | Early onset, family history of atopy, elevated IgE, responds well to ICS + anti-IgE |
| Eosinophilic (non-allergic) | Adult-onset, high blood/sputum eosinophils, often severe, responds to anti-IL-5 |
| Exercise-induced | Bronchoconstriction triggered by exercise; hyperventilation dries airway lining |
| Aspirin-exacerbated respiratory disease (AERD) | Triad: asthma + nasal polyps + aspirin/NSAID sensitivity; involves dysregulated arachidonic acid metabolism |
| Obesity-associated | Non-eosinophilic, difficult to control; associated with GERD, OSA |
| Occupational | Workplace sensitizers or irritants; improvement on vacations/weekends |
| Late-onset (adult) | Often severe, frequently non-atopic |
| Neutrophilic | Associated with smoking, infection, severe disease; steroid-resistant |
5. Triggers
| Category | Examples |
|---|---|
| Allergens | House dust mites, cockroach, mold, pet dander, seasonal pollens |
| Viral infections | Rhinovirus most common; increased AHR for 4-6 weeks post-infection; COVID-19 pandemic saw ~50% reduction in exacerbations (attributed to reduced viral infections) |
| Exercise + cold/dry air | Hyperventilation dries airway lining → osmolarity change → mediator release; cold air compounds this effect |
| Air pollution | Ozone, sulfur dioxide, nitrogen dioxide, particulate matter |
| Drugs | Beta-blockers (even ophthalmic drops); aspirin/NSAIDs (in AERD); ACE inhibitors (cause cough that can mimic poor asthma control) |
| Occupational | High MW (isocyanates, anhydrides) and low MW agents; reactive airway dysfunction syndrome (RADS) from single high-level irritant exposure |
| Hormonal | Perimenstrual symptoms (rapid estrogen fluctuations); pregnancy |
| Stress | Poorly understood mechanism |
| Irritants | Tobacco smoke, strong odors, cleaning products |
6. Clinical Features
Symptoms (Classic Triad)
- Episodic wheezing (expiratory > inspiratory)
- Shortness of breath (worse on exertion, at night, or after exposure to triggers)
- Chest tightness
- Cough (may be the only symptom - "cough-variant asthma")
- Symptoms often worse on arising in the morning or at night
- History of atopy (eczema, rhinitis, food allergies) is common
Physical Examination
- May be completely normal between attacks
- During attacks: expiratory wheeze, prolonged expiration, use of accessory muscles, hyperinflated chest
- Severe attack: silent chest (no wheeze due to minimal air entry - DANGER sign), cyanosis, pulsus paradoxus, inability to complete sentences
Asthma Control Assessment (GINA)
| Domain | Controlled | Partly Controlled | Uncontrolled |
|---|---|---|---|
| Daytime symptoms | None (≤2/week) | >2/week | ≥3 features of partly controlled |
| Night waking due to asthma | None | Any | |
| SABA reliever use | None (≤2/week) | >2/week | |
| Activity limitation | None | Any |
7. Diagnosis
Step 1: Compatible History
⚠️ Important: More than one-third of patients with a physician diagnosis of asthma do NOT meet diagnostic criteria. Always confirm with objective testing.
Step 2: Pulmonary Function Tests
- FEV₁/FVC ratio <0.70 (or below LLN) confirms obstruction
- Post-bronchodilator FEV₁ improvement ≥12% AND ≥200 mL = significant reversibility (confirms asthma)
- Post-BD FEV₁ improvement ≥10-15% from baseline = positive
- Variability >10% (am vs pm, or day-to-day) is suggestive
- Portable, inexpensive, useful for monitoring in moderate-severe asthma and pregnant women
- Methacholine or histamine challenge
- PC20 (provocative concentration causing 20% fall in FEV₁): <8 mg/mL = positive AHR
- ATS impairment rating uses PC20 alongside FEV₁ and medication need
| Score | PC20 (mg/mL) | Interpretation |
|---|---|---|
| 0 | >8 | Normal |
| 1 | 8 to >0.5 | Mild AHR |
| 2 | 0.5 to >0.125 | Moderate AHR |
| 3 | ≤0.125 | Severe AHR |
- Marker of eosinophilic (T2) airway inflammation
- ≥40 ppb = elevated, suggests eosinophilic asthma, predicts ICS response
- <25 ppb = ICS-responsive eosinophilic inflammation less likely
Step 3: Adjunctive Evaluation
| Test | Purpose |
|---|---|
| Skin prick testing / specific IgE | Identify allergen sensitization |
| Blood eosinophil count | T2 phenotyping; biologic eligibility |
| Serum total + specific IgE | Omalizumab eligibility |
| FeNO | T2 inflammation marker |
| Sputum eosinophils | Research/difficult-to-treat asthma |
| CT chest | Exclude bronchiectasis, ABPA, structural causes |
| Chest X-ray | Baseline; exclude other diagnoses |
| Allergen challenge | Occupational asthma assessment |
8. Comorbidities
| Comorbidity | Key Points |
|---|---|
| Rhinosinusitis / Nasal polyps | Nasal polyps in adults + asthma → think AERD; intranasal steroids reduce AHR and ED visits; biologics increasingly used |
| GERD | Independent predictor of exacerbations; treatment of symptomatic GERD improves airway function; asymptomatic GERD treatment not beneficial |
| Obesity | 2-4x more hospitalization risk; non-eosinophilic, steroid-resistant pattern; bariatric surgery improves control |
| OSA | Increased prevalence in asthma; apnea-hypopnea index correlates with severe exacerbations; CPAP improves QoL and reduces exacerbations; systemic corticosteroids for asthma worsen OSA by causing weight gain and pharyngeal muscle myopathy |
| Anxiety/Depression | Increased exacerbation rates; patients may not distinguish anxiety attacks from asthma |
| Vocal cord dysfunction (ILO) | Can mimic or coexist with asthma; more common in women; definitive diagnosis by laryngoscopy during symptomatic episode |
9. Medications
9.1 Beta-2 Agonists
- Albuterol (salbutamol): onset 3-5 min, duration 4-6 h; MDI or nebulizer
- Indicated for reliever (rescue) therapy
- Regular use → tachyphylaxis of bronchoprotective effect; associated with increased mortality when used without ICS
- β₂-receptor polymorphism at amino acid 16 → increased airway reactivity with regular SABA use
- Salmeterol (slow onset), Formoterol (rapid onset, comparable to SABA)
- NEVER use as monotherapy in asthma (increased mortality risk)
- Always combine with ICS
- Indacaterol, olodaterol, vilanterol
- Only used in combination with ICS in asthma
9.2 Inhaled Corticosteroids (ICS)
- Beclomethasone (dipropionate) - older, 20% oral bioavailability
- Budesonide - moderate bioavailability, safe in pregnancy
- Fluticasone propionate - ~1% oral bioavailability
- Mometasone - <1% oral bioavailability
- Fluticasone furoate - ultra-LABA combination (vilanterol)
- Ciclesonide - pro-drug, activated only in lung tissue, minimal systemic effects
9.3 Anticholinergics (Muscarinic Antagonists)
- SAMA (ipratropium): Used for acute severe asthma (combined with SABA in emergency)
- LAMA (tiotropium): Add-on therapy at Step 4-5; can be used instead of LABA in some patients
- ICS/LAMA approved for asthma in adults; some concern of numerical (not significant) increased mortality in African Americans vs ICS/LABA
9.4 Leukotriene Receptor Antagonists (LTRAs)
- Montelukast, zafirlukast, pranlukast
- Alternative controller at Step 2; useful for aspirin-exacerbated disease and exercise-induced asthma
- ⚠️ FDA black box warning: Montelukast associated with serious neuropsychiatric effects including suicidal ideation - this limits use as first-line alternative
9.5 Theophylline
- Now rarely used due to narrow therapeutic window, drug-drug interactions, and reduced bronchodilation vs other agents
- Occasionally used as add-on in Step 4-5 in resource-limited settings
9.6 Anti-IgE Therapy
- Omalizumab (anti-IgE monoclonal antibody): for moderate-severe allergic asthma; eligibility - perennial allergen sensitization, elevated total IgE
- Reduces exacerbations, emergency visits, steroid use
- GINA 2026: also approved for CRSwNP (along with omalizumab-igec biosimilar)
9.7 Anti-IL-5 / Anti-IL-5Rα
- Mepolizumab (anti-IL-5): SC, every 4 weeks; blood eosinophils ≥150-300/µL
- Reslizumab (anti-IL-5): IV, weight-based; blood eosinophils ≥400/µL
- Benralizumab (anti-IL-5Rα): SC, every 4 weeks (then every 8 weeks); produces near-complete eosinophil depletion; blood eosinophils ≥300/µL
- Depemokimab (NEW - GINA 2026): approved for severe eosinophilic asthma ≥12 years; also approved for CRSwNP ≥18 years; long-acting biologic
9.8 Anti-IL-4Rα
- Dupilumab: Blocks both IL-4 and IL-13 signaling; for moderate-severe eosinophilic/type 2 asthma; also effective for CRSwNP and atopic dermatitis (addresses "one airway, one disease")
9.9 Anti-TSLP
- Tezepelumab: Anti-TSLP (targets most upstream alarmin); effective even in patients without classic T2 biomarkers; broad efficacy across phenotypes including non-eosinophilic asthma; GINA 2026 includes it in CRSwNP indication
10. Stepwise Management (GINA 2026 / NAEPP Framework)
Key Paradigm Shift - Anti-Inflammatory Reliever (AIR)
A landmark change: ICS/formoterol (single inhaler) used as-needed for relief - instead of SABA alone - is now the preferred approach at all steps. This reduces severe exacerbations and OCS use by ensuring anti-inflammatory therapy accompanies every bronchodilator dose.
| Step | Preferred Therapy | Alternative |
|---|---|---|
| Step 1 (Intermittent) | As-needed low-dose ICS/formoterol (AIR) | As-needed ICS + SABA (NAEPP); As-needed SABA alone (if AIR unavailable) |
| Step 2 (Mild persistent) | Low-dose ICS daily + as-needed ICS/formoterol (AIR) | Low-dose ICS daily + SABA; LTRA (but monitor for neuropsychiatric effects) |
| Step 3 (Moderate persistent) | Low-dose ICS/LABA daily + as-needed ICS/formoterol | Medium-dose ICS; LTRA add-on |
| Step 4 (Severe) | Medium-dose ICS/LABA daily + as-needed ICS/formoterol | Add LAMA; add LTRA or theophylline |
| Step 5 (Very severe/uncontrolled) | High-dose ICS/LABA + LAMA + biologic therapy (anti-IgE, anti-IL-5, anti-IL-4Rα, anti-TSLP) | Minimal oral corticosteroids (minimize OCS due to side effects) |
- Based on: Type 2 biomarkers (FeNO, blood eosinophils, IgE), comorbidities (AERD, CRSwNP, atopic dermatitis), cost, dosing frequency, route of administration, patient preference
- All biologics in GINA 2026 decision tree are for T2 inflammation
- Step UP after 2-3 months of poor control (rule out: poor adherence, poor technique, ongoing exposure, comorbidities first)
- Step DOWN when well-controlled for ≥3 months (avoid discontinuing ICS entirely)
- All patients must receive ICS-containing therapy
- ICS/formoterol or ICS/SABA as AIR reduces the risk of severe exacerbations requiring OCS
- Treat modifiable risk factors; improve inhaler technique; patient education
11. Acute Severe Asthma (Asthma Attack)
Assessment of Severity
| Feature | Moderate Attack | Severe Attack | Life-Threatening |
|---|---|---|---|
| Speech | Full sentences | Phrases | Words/unable |
| RR | 20-25 | 25-30 | >30 |
| HR | <110 | 110-120 | >120 |
| PEFR | >50-75% best | 33-50% best | <33% best ("brittle") |
| SpO₂ | >95% | 92-95% | <92% |
| Wheeze | Moderate | Loud | Silent chest (DANGER) |
| Mental status | Normal | Agitated | Drowsy/confused |
| PaCO₂ | <45 | <45 | ≥45 (impending respiratory failure) |
⚠️ A normal or rising PaCO₂ in a severe asthma attack indicates fatigue and impending respiratory failure - prepare for intubation.
GINA 2026 - Acute Management
- SABA (salbutamol 4-8 puffs via MDI with spacer OR nebulizer) up to every 1h
- ICS/formoterol as AIR for mild exacerbations (alternative to SABA)
- Increase maintenance ICS dose 4-5 fold
- Oral corticosteroids if not responding
- Salbutamol up to 3 times, 20-30 min apart (GINA 2026 specifies dosing)
- Ipratropium 4 puffs with salbutamol for up to 3 times
- Oral/IV corticosteroids initiated
- Supplemental oxygen (GINA 2026 updated SpO₂ targets)
- IV magnesium sulfate 2g over 20 min for life-threatening/refractory cases
- Heliox (helium-oxygen mixture) - reduces work of breathing in very severe cases
- NIV may be considered in selected patients
- ICU + intubation for respiratory failure (mechanical ventilation is challenging - increased risk of barotrauma, air-trapping, permissive hypercapnia strategy)
After Acute Attack:
- Oral corticosteroids typically for 5-7 days
- Increase controller therapy
- Arrange early follow-up (within 1 week)
- GINA 2026: updated discharge planning and follow-up protocols
12. Special Considerations
Asthma in Pregnancy
- ~4% of pregnant women have asthma; ~1/3 worsen during pregnancy
- FEV₁ and PEFR unchanged in pregnancy (useful for monitoring)
- Progesterone → increased tidal volume + minute ventilation (normal in pregnancy)
- ABG in pregnancy: pH 7.45, PaCO₂ 27-32 mmHg (respiratory alkalosis = normal)
- A normal PaCO₂ (40 mmHg) in a pregnant asthmatic = hypercapnia relative to normal pregnancy values
- Moderate-severe asthma in pregnancy increases risk of preterm labor, low birth weight, perinatal death, preeclampsia
- ICS are safe in pregnancy - undertreated asthma is far more dangerous to the fetus than ICS
Aspirin-Exacerbated Respiratory Disease (AERD)
- Triad: asthma + nasal polyposis + hypersensitivity to aspirin/NSAIDs
- Mechanism: Cyclooxygenase-1 inhibition → shunting of arachidonic acid toward leukotriene pathway
- Nasal polyps in adults should raise suspicion
- Management: Avoid NSAIDs; LTRAs (zafirlukast/montelukast) helpful; aspirin desensitization
Asthma-COPD Overlap (ACO)
- Features of both asthma (reversibility, AHR, eosinophilia) and COPD (incomplete reversibility, smoking history, emphysema on CT)
- Treatment is complex; ICS important; long-acting bronchodilators
- SABA monotherapy alone is contraindicated
Occupational Asthma
- Sensitizer-induced: develops after a latency period; caused by high MW (proteins) or low MW (chemicals like isocyanates) agents
- Irritant-induced (RADS): after single, high-level irritant exposure; no latency period
- Diagnosis: serial PEF measurements at work and away; specific bronchial challenge; reduction on vacation = diagnostic clue
13. Monitoring Parameters
| Parameter | Use |
|---|---|
| Asthma Control Test (ACT) | Score ≤19 = uncontrolled; validated questionnaire |
| PEFR diary | Daily monitoring; diurnal variation >10% = poor control |
| FeNO | Follow T2 inflammation; guide ICS titration |
| Blood eosinophils | Monitor T2; guide biologic eligibility |
| Spirometry | Baseline, annual, or when control changes |
| CAAT (new in GINA 2026) | Chronic Airways Assessment Test |
| Peds-AIRQ / PRAM (new in GINA 2026) | Pediatric assessment tools |
14. Fatality Risk Indicators (GINA 2026 - New Focus)
- Previous near-fatal attack (intubation, ICU)
- Hospitalization for asthma in past year
- Currently not using ICS or poor adherence
- Currently using or recently stopped OCS
- Overuse of SABA (>1 canister/month)
- No written asthma action plan
- History of psychiatric illness or psychosocial problems
- Food allergy with confirmed sensitization
- Comorbid cardiovascular disease
15. Quick Reference Summary
ASTHMA = Episodic obstruction + AHR + Inflammation (usually eosinophilic)
Diagnosis: Symptoms + reversible obstruction on spirometry
OR positive bronchial provocation (PC20 <8 mg/mL)
T2 biomarkers: FeNO ≥40, eosinophils ≥300/µL, elevated IgE
Reliever (ALL steps): ICS/formoterol (AIR) - NOT SABA alone [GINA 2026]
Controller hierarchy:
Step 1-2: Low ICS ± LTRA
Step 3: ICS/LABA
Step 4: Medium ICS/LABA ± LAMA
Step 5: Biologic (anti-IgE, anti-IL-5, anti-IL-4Rα, anti-TSLP)
Acute severe: SABA + ipratropium + OCS; Mg²⁺ for life-threatening
Silent chest + normal PaCO₂ = DANGER signs
Biologics (T2): Omalizumab, mepolizumab, reslizumab, benralizumab,
dupilumab, tezepelumab, depemokimab (NEW 2026)
- ICS/formoterol as AIR at ALL steps (including Step 1) - reducing OCS need
- New biologic: Depemokimab for severe eosinophilic asthma (≥12y) and CRSwNP (≥18y)
- Updated fatality risk indicators - greater emphasis on prevention of asthma death
- New assessment tools: CAAT, Peds-AIRQ, PRAM
- Updated SpO₂ targets and SABA dosing in acute management
- Biologic decision tree updated for T2 inflammation with comorbidity consideration
Tell me detail about asthma
- Definition & Epidemiology
- Pathophysiology - Type 2 vs Non-Type 2 inflammation, airway remodeling, AHR mechanisms, with the airway cross-section diagram
- ICS Pharmacology - oral bioavailability comparison, systemic effects
- Classification - phenotypes (allergic, eosinophilic, AERD, obesity-associated, neutrophilic, occupational)
- Triggers - allergens, viral infections, drugs (beta-blockers, aspirin, ACE inhibitors), exercise, pollution
- Clinical Features - symptoms, physical exam, control assessment table
- Diagnosis - spirometry, PEFR, bronchial provocation (PC20), FeNO, blood eosinophils, skin testing
- Comorbidities - rhinosinusitis, GERD, obesity, OSA, vocal cord dysfunction, anxiety
- Medications - SABAs, LABAs, ICS (agents + bioavailability), LAMAs, LTRAs (montelukast warning), theophylline, all biologics
- Stepwise Management (GINA 2026) - including the AIR (Anti-Inflammatory Reliever) paradigm shift
- Acute Severe Asthma - severity grading table, management protocol, danger signs
- Special Situations - pregnancy, AERD, ACO, occupational asthma
- GINA 2026 Key Updates - depemokimab, new assessment tools, fatality risk indicators
More detail
"severe asthma" AND "biologic therapy"
asthma pathophysiology immunology type 2 inflammation T2 non-T2 endotypes 2025 2026
ASTHMA - Deep Dive (Extended PGT Reference)
PART 1: EPIDEMIOLOGY (in depth)
- ~262 million people affected globally (Harrison's 2025)
- US prevalence: 7.9% (vs ~4.3% worldwide); has been rising since 2001 (was 7.3%)
- More common in children (8.4%) than adults (7.7%)
- Children: 2:1 male > female ratio
- Adults: female > male (hormonal influence)
- Highest US prevalence: Puerto Rican population; highest morbidity in Black race
- 1.8 million US ED visits/year; 189,000 hospitalizations (2016 data)
- Total US economic cost: $82 billion (2013)
- Asthma mortality: rose in 1960s (due to overuse of high-potency inhaled β₂-agonists); declined after 1990s with widespread ICS use; mortality rate declined from 0.44 per 100,000 (1993) to 0.19 (2006) - but no further reduction since then
- COVID-19 pandemic → nearly 50% reduction in exacerbations (attributed to decreased viral infections from social distancing)
PART 2: PATHOGENESIS - FROM ALLERGEN TO AIRWAY (Molecular Detail)
2.1 The Asthma Development Pathway
GENETIC SUSCEPTIBILITY
+
ENVIRONMENTAL EXPOSURES (allergens, pollution, infections, tobacco)
+
DEVELOPMENTAL FACTORS (aging, hormonal changes, obesity)
↓
Airway Hyperresponsiveness
+
Airway Inflammation (Type 2 or non-Type 2)
+
Structural Changes (Remodeling)
↓
ASTHMA (symptoms ← triggers → exacerbations)
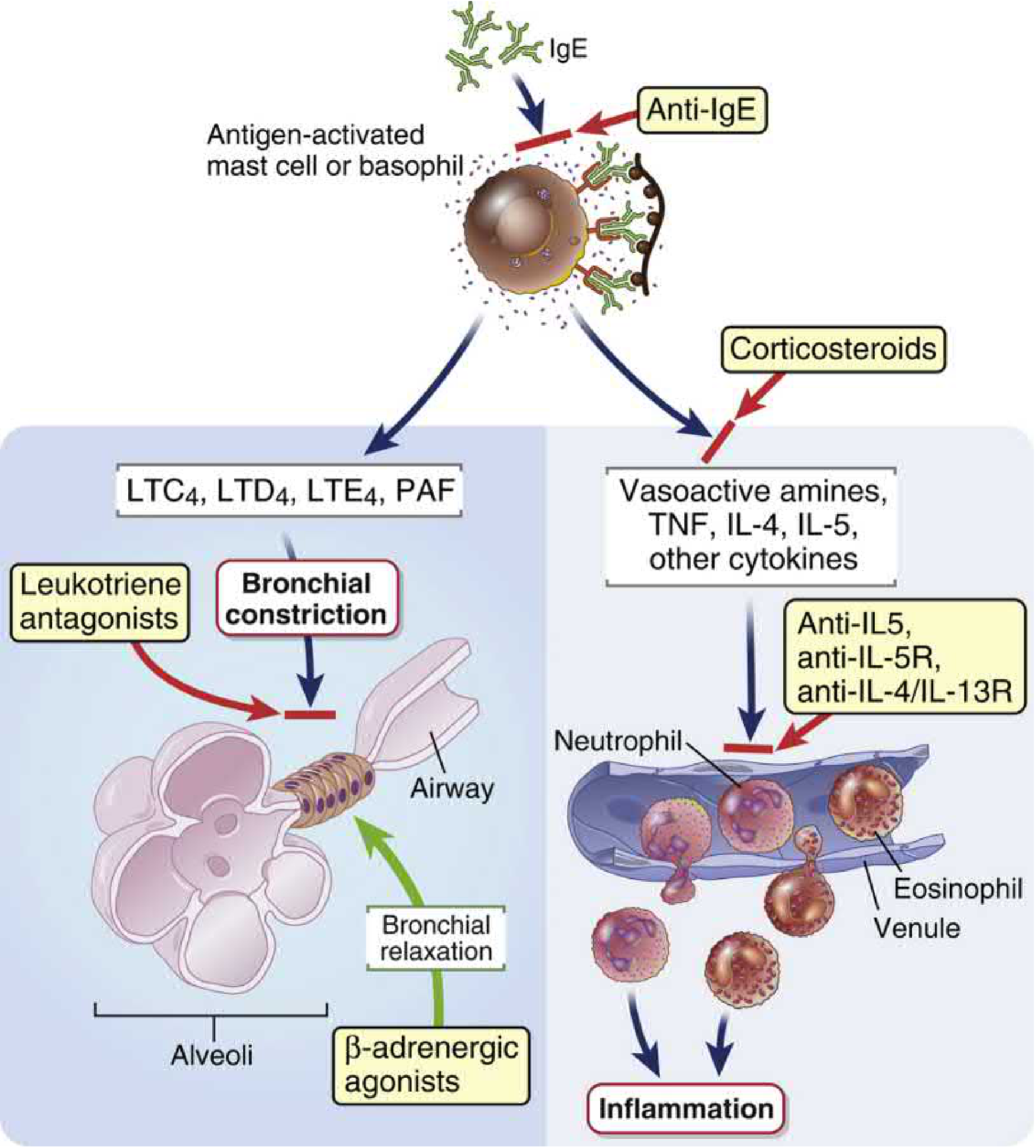
2.2 The Allergic (IgE-mediated) Cascade
- Allergen enters airway mucosa
- Captured by dendritic cells → processed → presented via MHCII to naive T-cells
- In atopic individuals → Th2 polarization (master transcription factor: GATA-3)
- Th2 cells produce: IL-4 (drives B-cell class switching to IgE), IL-5 (eosinophil survival/activation), IL-13 (mucus production, AHR, IgE)
- B-cells produce IgE antibodies → bind to FcεRI receptors on mast cells and basophils
- Allergen cross-links surface-bound IgE on mast cells
- Mast cell degranulation → rapid release of preformed mediators (within minutes)
- New mediator synthesis occurs over hours
2.3 Mast Cell - The Central Effector Cell
| Mediator | Effect |
|---|---|
| Histamine | Smooth muscle contraction, vasodilation, increased vascular permeability, mucus secretion |
| Tryptase | Protease; activates complement, kinin, coagulation pathways; marker of mast cell activation |
| Heparin | Anti-coagulant; potentiates tryptase |
| Mediator | Pathway | Effect |
|---|---|---|
| LTC₄ → LTD₄ → LTE₄ (cysteinyl leukotrienes) | 5-lipoxygenase (5-LO) | Major mediators of bronchoconstriction (1000x more potent than histamine); vascular permeability, mucus secretion |
| LTB₄ | 5-LO | Neutrophil chemotaxis |
| PGD₂ (Prostaglandin D₂) | COX pathway | Bronchoconstriction, vasodilation, eosinophil/basophil recruitment via CRTH2 receptor |
| PAF (Platelet-Activating Factor) | Phospholipase A₂ | Bronchoconstriction, platelet aggregation, eosinophil recruitment |
| Thromboxane A₂ | COX pathway | Bronchoconstriction, vasoconstriction |
| Cytokine | Source | Effect |
|---|---|---|
| IL-4 | Mast cells, Th2 | IgE class switching; upregulates VCAM-1 (eosinophil trafficking) |
| IL-5 | Mast cells, Th2, ILC2 | Eosinophil maturation (bone marrow), survival, activation |
| IL-13 | Mast cells, Th2, ILC2 | Mucus hypersecretion (goblet cell metaplasia), AHR, IgE production, airway remodeling |
| TNF-α | Mast cells, macrophages | Pro-inflammatory, NF-κB activation, adhesion molecule upregulation |
Biphasic Response: The initial bronchoconstriction (early asthmatic response, EAR) reflects histamine, PG, and leukotriene effects. The late-phase reaction (LAR, 4-6h later) is cytokine/eosinophil-mediated sustained inflammation. Corticosteroids suppress the late phase but NOT the early phase. LTRAs suppress BOTH phases.
2.4 The Alarmin Cascade (Innate Immunity - Critical for PGT)
| Alarmin | Source | Downstream Effect |
|---|---|---|
| TSLP (Thymic Stromal Lymphopoietin) | Epithelium | Activates dendritic cells → Th2 polarization; activates ILC2s; stimulates mast cells; promotes neutrophilic inflammation (T2-low path) |
| IL-25 (IL-17E) | Epithelium, eosinophils | Activates ILC2s → IL-4, IL-5, IL-13 production |
| IL-33 | Epithelium, smooth muscle | Activates ILC2s and mast cells → IL-5, IL-13; amplifies T2 inflammation |
ILC2s (Innate Lymphoid Cells type 2) can drive T2 inflammation without allergen sensitization - this explains non-allergic eosinophilic asthma. TSLP is the most upstream alarmin and the broadest therapeutic target (tezepelumab).
2.5 Eosinophil in Asthma
- IL-5 (differentiation from bone marrow progenitors)
- Eotaxins (CCL11, CCL24, CCL26) via CCR3 receptor on eosinophils
- VCAM-1 on endothelium (upregulated by IL-4)
| Product | Effect |
|---|---|
| MBP (Major Basic Protein) | Toxic to epithelium; causes epithelial shedding; directly induces AHR |
| ECP (Eosinophil Cationic Protein) | Toxic to epithelium and parasites; induces mast cell histamine release |
| EPO (Eosinophil Peroxidase) | Oxidative damage via H₂O₂ + halide |
| EDN (Eosinophil-Derived Neurotoxin) | Ribonuclease; neurotoxic; AHR |
| Cysteinyl leukotrienes (LTC₄) | Bronchoconstriction, mucus secretion |
| IL-5, IL-13 | Perpetuates T2 inflammation |
2.6 Type 2 vs Non-Type 2 Detailed Comparison
| Feature | T2-High | T2-Low (Neutrophilic) | T2-Low (Paucigranulocytic) |
|---|---|---|---|
| Frequency | ~50-70% | ~20-30% | ~10-20% |
| Inflammatory cells | Eosinophils + mast cells | Neutrophils | None predominant |
| Key cytokines | IL-4, IL-5, IL-13, TSLP, IL-33, IL-25 | IL-17A, IL-17F, IL-8 (CXCL8) | Unclear |
| Driving cells | Th2 + ILC2 | Th17 + ILC3 | Smooth muscle intrinsic |
| Blood eosinophils | ≥150-300/µL | Normal/low | Normal |
| FeNO | ≥25-40 ppb | Low (<25 ppb) | Low |
| Serum IgE | Often elevated | Normal | Normal |
| ICS response | Excellent | Poor (steroid-resistant) | Variable |
| Associated with | Atopy, allergic rhinitis, early-onset | Smoking, obesity, infection, neutrophil-driven | Smooth muscle-predominant |
| Periostin | Elevated (esp. AERD) | Low | Low |
| Treatment | ICS, biologics (anti-IgE, anti-IL-5, anti-IL-4Rα, anti-TSLP) | LAMA, bronchial thermoplasty, treat triggers | ICS + LABA; bronchial thermoplasty |
2.7 Airway Remodeling (Structural Changes)
| Change | Mechanism | Clinical Consequence |
|---|---|---|
| Goblet cell hyperplasia | IL-13, IL-5 | Mucus hypersecretion → mucus plugging |
| Submucosal gland hypertrophy | Cholinergic stimulation, IL-13 | Increased mucus volume |
| Subepithelial fibrosis | Myofibroblast activation → collagen (types I, III, V), tenascin, periostin, fibronectin, osteopontin | Airway wall stiffening → irreversible obstruction component |
| Smooth muscle hypertrophy + hyperplasia | Growth factors (EGF, PDGF, bFGF) | Increased contractile mass → AHR |
| Angiogenesis | VEGF (from eosinophils, mast cells, epithelium) | Airway edema; supports inflammatory cell trafficking |
| Epithelial shedding | MBP, EPO damage | Exposes sub-epithelial sensory nerves → AHR; forms epithelial-mesenchymal trophic unit |
| Neuronal remodeling | Nerve growth factor, substance P | Enhanced sensory nerve activity → cough, bronchoconstriction |
| Lymphatic remodeling | Decreased lymphatic density in fatal asthma despite elevated VEGF-C/D | Airway edema → worsened obstruction |
Remodeling begins early - subepithelial fibrosis is found even at disease onset. Corticosteroids suppress inflammation but do NOT consistently reverse remodeling. This is why prevention of progression is critical.
PART 3: GENETICS & RISK FACTORS
Genetic Factors
- Asthma has strong genetic heritability (~60-80% in twins)
- Candidate genes cluster around:
- Chromosome 5q31-33: IL-4, IL-5, IL-13, IL-9, GM-CSF gene cluster; β₂-adrenergic receptor
- Chromosome 11q13: FcεRI β-chain (high-affinity IgE receptor)
- Chromosome 12q: IFN-γ, stem cell factor, IGF
- Chromosome 13q: BRCA2, IgE regulation
- ORMDL3/GSDMB (chromosome 17q21): one of the strongest GWAS associations for childhood asthma
- β₂-receptor polymorphism at amino acid 16 (Arg→Gly): Gly/Gly homozygotes show greater tachyphylaxis with regular SABA use and increased AHR
Risk Factors for Development
| Factor | Mechanism |
|---|---|
| Allergen exposure in atopic individuals | IgE sensitization |
| Viral infections (RSV, rhinovirus in infancy) | Persistent AHR; may initiate asthma trajectory |
| Tobacco exposure (active + passive) | Airway inflammation, impaired mucociliary clearance |
| Air pollution | Oxidative stress, airway inflammation; ozone, NO₂, PM₂.₅ |
| Obesity | Altered lung mechanics; non-T2 inflammation; leptin effects; adipokines |
| Diet (Western diet, reduced antioxidants) | Increased oxidative stress; altered microbiome |
| Low vitamin D | Reduced regulatory T-cell function |
| Antibiotics in infancy | Altered gut microbiome (hygiene hypothesis) |
| Hygiene hypothesis | Reduced microbial exposure → failure to develop Th1 immunity → unopposed Th2 → atopy |
| Elite athletes (high-intensity exercise) | Repeated airway desiccation/osmotic stress |
PART 4: DIAGNOSIS IN DETAIL
4.1 Pulmonary Function Testing
| Finding | Significance |
|---|---|
| FEV₁/FVC <0.70 (or <LLN) | Obstructive pattern |
| Post-BD FEV₁ increase ≥12% AND ≥200 mL | Significant reversibility = confirms asthma |
| Near-normal FEV₁ between attacks | Mild asthma - spirometry alone may miss diagnosis |
| Low FEV₁ | Strong predictor of future exacerbations and decline in control |
| PEF variability >10% (am vs pm) | Suggests poor asthma control |
| PEF variability | Better predictor of future exacerbations than single PEF measurement |
- FEV₁ may be normal or near-normal in mild asthma - does NOT exclude the diagnosis
- Diagnosis may be difficult to confirm after starting ICS (obstruction and AHR mitigate with therapy) - if diagnosis uncertain, trial of medication taper may be needed
- Low FEV₁ = strongest objective predictor of poor asthma control and need for acute care
4.2 Bronchial Provocation Testing
- Direct smooth muscle stimulation via M₃ muscarinic receptors
- PC₂₀ <8 mg/mL = significant AHR (positive test)
- False positives: COPD, allergic rhinitis, heart failure, recent viral URTI (persists 4-6 weeks)
- If FEV₁ normal → use PC₂₅ for impairment rating
- Hyperventilation → airway desiccation → osmolarity change in lining fluid → mediator release
- >10-15% fall in FEV₁ post-exercise = positive
- More specific for exercise-induced bronchoconstriction
- Osmotic challenge - desiccates airway surface → mediator release
- Positive: ≥15% fall in FEV₁ at cumulative dose ≤635 mg
- Better specificity than methacholine for confirming active asthma
4.3 FeNO Interpretation
| FeNO Level | Interpretation | Action |
|---|---|---|
| <25 ppb | Low - eosinophilic inflammation unlikely | ICS response less likely; consider non-T2 |
| 25-50 ppb | Borderline | Consider clinical context |
| ≥40-50 ppb | High - eosinophilic T2 inflammation | Strong ICS response expected; biologic eligibility |
- FeNO is driven primarily by IL-13 → inducible NO synthase in airway epithelium
- Elevated in eosinophilic asthma, AERD, allergic rhinitis
- Falls with ICS - useful for monitoring adherence and adjusting dose
- NOT affected by acute bronchodilators
- Smoking falsely LOWERS FeNO
- Tall height and atopy increase FeNO
4.4 Sputum Eosinophil Count
- Eosinophils >2-3% = eosinophilic asthma; predicts ICS response and exacerbation risk
- Gold standard for T2 phenotyping but invasive; mainly used in research/specialist centres
- Useful to guide ICS dose titration in severe asthma (reduces exacerbations better than symptom-guided titration)
4.5 Blood Eosinophil Count (BEC)
| BEC | Interpretation |
|---|---|
| ≥150/µL | Suggests T2 inflammation; threshold for some biologic eligibility criteria |
| ≥300/µL | Strong T2 signal; preferred threshold for mepolizumab, benralizumab eligibility |
| ≥400/µL | Reslizumab eligibility threshold |
| >1500/µL | Hypereosinophilic syndrome territory - check for other causes |
4.6 Differential Diagnosis
| Condition | Key Distinguishing Feature |
|---|---|
| COPD | Smoking history; incomplete reversibility; FEV₁/FVC <0.70 post-BD; no significant atopy |
| Heart failure | Orthopnoea, PND, elevated BNP, basal crackles, dilated heart on CXR |
| Vocal cord dysfunction (ILO) | Inspiratory stridor; laryngoscopy-confirmed; resolves with speech therapy |
| Bronchiectasis | Chronic productive cough; finger clubbing; CT bronchial dilation + wall thickening |
| α₁-antitrypsin deficiency | Panlobular emphysema; liver disease; family history; measured levels |
| Bronchiolitis obliterans | Fixed obstruction; mosaic attenuation on HRCT; history of infection/transplant |
| Hyperventilation syndrome | Paraesthesias, tetany; normal spirometry; ETCO₂ low |
| Foreign body | Unilateral wheeze; history |
| Carcinoid / endobronchial mass | Fixed wheeze; stridor; CT/bronchoscopy |
PART 5: PHARMACOLOGY - MOLECULAR MECHANISMS
5.1 β₂-Agonist Mechanism (Molecular Detail)
β₂ receptor → Gs protein → Adenylyl cyclase
→ ↑cAMP → Protein Kinase A (PKA) activation
→ Phosphorylation of:
• Myosin light chain kinase (MLCK) → inhibited → smooth muscle RELAXATION
• K+ channels (Ca²⁺-activated K+) → opens → hyperpolarization → relaxation
• Decreased PI hydrolysis (↓IP₃ → ↓intracellular Ca²⁺)
• Increased Na⁺/K⁺-ATPase activity
• Increased myosin light chain phosphatase activity
- Inhibit mast cell mediator release (via β₂ on mast cells)
- Prevent microvascular leakage (reduce edema from histamine/LTD₄/PGD₂)
- Increase mucociliary clearance (enhance ion transport + mucus secretion from submucosal glands)
- Inhibit ACh release from presynaptic β₂ receptors on cholinergic nerves
- β₂-agonists are functional antagonists (relieve symptoms) but have NO anti-inflammatory effect
- Regular SABA use → tachyphylaxis of bronchoprotective effect
- Arg16 polymorphism patients: regular SABA → increased airway reactivity
- Increased SABA use = marker of poor control = associated with increased asthma mortality
- Hence GINA 2026 mandates ICS/formoterol as AIR (not SABA alone)
- Formoterol: moderate lipophilicity → stays near membrane receptor → slow-release property → but in plasma, loses this → can act rapidly; onset comparable to SABA (3-5 min)
- Salmeterol: long aliphatic chain anchored in receptor "exosite" → cannot dissociate rapidly → slow onset → NOT suitable as reliever
5.2 ICS Mechanism (Molecular Detail)
ICS molecule → enters cell → binds cytoplasmic glucocorticoid receptor (GR)
→ GR-ICS complex translocates to nucleus
→ Two mechanisms:
1. Trans-repression (anti-inflammatory - main effect):
Binds to NF-κB and AP-1 transcription factors
→ Inhibits expression of inflammatory genes:
(IL-4, IL-5, IL-13, TNF-α, ICAM-1, Cox-2, iNOS)
→ Reduces FeNO, eosinophil counts, AHR
2. Trans-activation (side effects - via GRE binding):
Upregulates anti-inflammatory proteins (annexin-1, SLPI)
→ Also responsible for: growth suppression, bone loss, cataracts, skin thinning
| Drug | Oral Bioavailability | Half-life | Special Feature |
|---|---|---|---|
| Beclomethasone (BDP) | ~20% | ~0.5h (activated to 17-BMP in lung) | Oldest; oropharyngeal deposition issue |
| Budesonide | ~10-15% | 2-3h | Safe in pregnancy; both pMDI and DPI |
| Fluticasone propionate | ~1% | 14h | High topical potency; low oral BA |
| Fluticasone furoate | Negligible | 24h | Once-daily; used with vilanterol |
| Mometasone | <1% | 5h | Very low oral BA |
| Ciclesonide | <1% | 0.7h (parent); 45h (active metabolite) | Pro-drug activated in lung by esterases; no oropharyngeal deposition; minimal systemic effects |
5.3 ICS Resistance
- Reduced GR expression in inflammatory cells
- GR-β isoform (acts as dominant negative inhibitor of GR-α)
- NF-κB/AP-1 overactivation (overcomes steroid suppression)
- HDAC2 (histone deacetylase 2) reduction - required for ICS to work; reduced by oxidative stress (smoking, severe asthma)
- Macrophage-predominant neutrophilic inflammation - inherently ICS-resistant
5.4 Anticholinergic Mechanism
Cholinergic nerve stimulation → ACh release → M₃ receptor on smooth muscle
→ ↑IP₃ → ↑Ca²⁺ → smooth muscle CONTRACTION
Anticholinergics (SAMA/LAMA) → M₃ receptor blockade → smooth muscle RELAXATION
- Less effective than β₂-agonists as bronchodilators (ACh is only one bronchoconstrictor pathway)
- Also block M₃ receptors on submucosal glands → reduce mucus secretion
- M₂ receptors (presynaptic, autoinhibitory) - if blocked → increased ACh release (pro-constrictive)
- Tiotropium (LAMA): preferential M₃/M₁ kinetics → functional selectivity despite non-selective binding
5.5 Leukotriene Pathway and LTRAs
Arachidonic acid → 5-lipoxygenase (5-LO) + 5-LO activating protein (FLAP)
→ LTA₄ → LTC₄ (via glutathione-S-transferase)
→ secreted → cleaved to LTD₄ → LTE₄
All bind CysLT₁ receptor on smooth muscle, mucus glands, inflammatory cells
→ Bronchoconstriction + mucus hypersecretion + eosinophil recruitment + vascular permeability
LTRA (montelukast, zafirlukast) → CysLT₁ receptor antagonism
→ Reduces: early AND late phase response, exercise-induced bronchoconstriction,
aspirin-triggered bronchoconstriction (AERD), nasal polyp growth
Leukotrienes are 1000x more potent than histamine as bronchoconstrictors. LTD₄ = most potent. FDA black box warning on montelukast (2020): serious neuropsychiatric events including suicidal ideation, depression, nightmares, aggression - must inform patients before prescribing.
PART 6: BIOLOGICS - FULL MECHANISTIC GUIDE
6.1 Overview - How Biologics Target T2 Inflammation
Allergen/Damage
↓
EPITHELIUM → TSLP → [Tezepelumab]
IL-33 → [Itepekimab (in trials)]
IL-25
↓
ILC2 / Th2
↓
IL-4 → IgE class switch → IgE → [Omalizumab / Omalizumab-igec]
IL-5 → Eosinophil maturation/survival → [Mepolizumab, Reslizumab]
↓ IL-5Rα → [Benralizumab, Depemokimab]
IL-13 → Mucus, AHR, fibrosis
↕
IL-4Rα (shared receptor subunit for IL-4 and IL-13) → [Dupilumab]
6.2 Individual Biologics
| Biologic | Target | Route/Frequency | Blood Eos Threshold | Key Features |
|---|---|---|---|---|
| Omalizumab | IgE | SC q2-4 weeks | Not required (IgE-based) | Serum IgE 30-700 IU/mL + perennial allergen sensitization; reduces exacerbations ~25-50%; also for CRSwNP, urticaria |
| Omalizumab-igec | IgE (biosimilar) | SC q2-4 weeks | Not required | New in GINA 2026; biosimilar of omalizumab; now approved for CRSwNP |
| Mepolizumab | IL-5 | SC 100 mg q4 weeks | ≥150/µL (screen); ≥300/µL preferred | Reduces exacerbations ~50%; reduces OCS use; also for EGPA, HES, CRSwNP |
| Reslizumab | IL-5 | IV weight-based q4 weeks | ≥400/µL | Only IV biologic; reduces exacerbations ~50% |
| Benralizumab | IL-5Rα | SC 30mg q4 weeks ×3, then q8 weeks | ≥300/µL | Near-complete blood eosinophil depletion (depletes via ADCC); also for CRSwNP |
| Dupilumab | IL-4Rα (blocks IL-4 + IL-13) | SC q2 weeks | ≥150/µL or FeNO ≥25 ppb | Broadest T2 coverage; also atopic dermatitis, CRSwNP, eosinophilic esophagitis, COPD with eos; arthralgia side effect |
| Tezepelumab | TSLP | SC q4 weeks | None required | Broadest efficacy including T2-low/paucigranulocytic; upstream target; reduces exacerbations even with low eos/FeNO; also for CRSwNP |
| Depemokimab | IL-5 (long-acting) | SC q6 months | ≥300/µL | NEW (GINA 2026); longest dosing interval of any biologic; ≥12y for eos asthma; ≥18y for CRSwNP |
Step 5 Severe Asthma - Need Biologic?
↓
Check T2 biomarkers (blood eos, FeNO, IgE, allergen sensitization)
↓
If ALLERGIC + elevated IgE → Omalizumab (or omalizumab-igec)
If EOSINOPHILIC (eos ≥300) → Anti-IL-5: Mepolizumab / Benralizumab / Reslizumab / Depemokimab
If EOSINOPHILIC + ATOPIC DERMATITIS/CRSwNP → Dupilumab (addresses "one airway" disease)
If BROAD T2 or UNCERTAIN or T2-LOW with eos → Tezepelumab (upstream, broadest)
If ALL T2 POSITIVE → Choose based on comorbidities, cost, route, frequency, patient preference
PART 7: GINA 2026 STEPWISE MANAGEMENT - FULL TABLE
| Step | Preferred Controller | Preferred Reliever | Notes |
|---|---|---|---|
| Step 1 (Symptoms <2/month) | As-needed low-dose ICS-formoterol | ICS-formoterol (AIR) | Alternative: Low-dose ICS taken whenever SABA taken (NAEPP); SABA alone only if no ICS access |
| Step 2 (Symptoms ≥2/month, not daily) | Low-dose ICS daily OR as-needed low-dose ICS-formoterol | ICS-formoterol (AIR) | Alternative: LTRA or low-dose ICS taken with SABA |
| Step 3 (Daily symptoms) | Low-dose ICS/LABA | ICS-formoterol (AIR) | Alternative: medium-dose ICS; low-dose ICS + LTRA |
| Step 4 (Daily symptoms, uncontrolled on Step 3) | Medium-dose ICS/LABA | ICS-formoterol (AIR) | Add-on: LAMA (tiotropium); add-on LTRA |
| Step 5 (Uncontrolled on Step 4) | High-dose ICS/LABA + phenotypic assessment → biologic | ICS-formoterol (AIR) | Options: anti-IgE, anti-IL-5/5Rα, anti-IL-4Rα, anti-TSLP; Add low-dose OCS as last resort (side effects) |
- Step UP: If poorly controlled for ≥2-3 months; FIRST check: adherence, inhaler technique, trigger avoidance, comorbidities
- Step DOWN: When well-controlled for ≥3 months; do NOT fully stop ICS (risk of rebound)
- Never stop ICS suddenly in any patient at any step
PART 8: STATUS ASTHMATICUS - DEEP ICU MANAGEMENT
8.1 Definition
8.2 Pathophysiology of Acute Attack
Bronchoconstriction + airway edema + mucus plugging
↓
Air trapping → dynamic hyperinflation
↓
↑ Intrinsic PEEP (auto-PEEP) → increased work of breathing
↓
Respiratory muscle fatigue → Hypercapnia (DANGER)
↓
Respiratory failure → Cardiorespiratory arrest
| Stage | PaO₂ | PaCO₂ | pH | Interpretation |
|---|---|---|---|---|
| Early/mild | Normal or ↓ | ↓ (hypocapnia) | ↑ (alkalosis) | Tachypnea compensates; hyperventilation |
| Moderate | ↓ | Normal (~40) | Normal | DANGER: Normal PaCO₂ in distress = fatigue |
| Severe | ↓↓ | ↑ | ↓ (acidosis) | Respiratory failure - intubate |
Key exam point: A "normal" PaCO₂ in an acutely distressed asthmatic indicates impending respiratory failure. Most asthmatics should be hypocapnic during an attack.
8.3 Emergency Management Protocol
- Supplemental O₂ to maintain SpO₂ 93-95% (GINA 2026 specifies updated SpO₂ targets; avoid hyperoxia)
- Salbutamol (albuterol) via MDI+spacer (4-8 puffs) OR nebuliser - repeat every 20 min up to 3 times
- Ipratropium bromide 4-8 puffs via MDI OR 0.5 mg nebulised - with each salbutamol dose (up to 3 times)
- Systemic corticosteroids: Oral prednisolone 40-50 mg OR IV hydrocortisone 100-200 mg if cannot swallow; onset of effect 4-6h
- Indications: Impending/actual respiratory failure, deteriorating mental status, PaCO₂ rising + acidosis, silent chest, exhaustion
- Challenges: High airway resistance → high peak pressures → risk of barotrauma, pneumothorax
- Mechanical ventilation strategy:
- Low respiratory rate (RR 8-12/min) + low tidal volume (6-8 mL/kg IBW)
- Long expiratory time (I:E ratio 1:3 or 1:4) to minimize auto-PEEP and air trapping
- Permissive hypercapnia: Allow PaCO₂ to rise (accept pH ≥7.2); correct severe acidosis with sodium bicarbonate if pH <7.2
- Neuromuscular paralysis (short-term) to reduce peak airway pressures
- Ketamine as induction agent: bronchodilator properties via catecholamine release; drug of choice for intubation in severe asthma
- Volatile anaesthetic agents (isoflurane, sevoflurane): potent bronchodilators; use in refractory cases at specialist centres; associated with increased ventilator length in some studies
- Bronchoscopy to clear mucus plugs: described but potentially dangerous during difficult MV; reserved for selected cases
8.4 Asthma Mortality Risk Factors (Harrison's 2025)
- History of ICU admission for asthma
- History of intubation for asthma
- Illicit drug use
- Depression
- New diagnosis within past year
- ≥2 ED visits in past 6 months
- Severe psychosocial problems
- Lower socioeconomic status
- ≥2 courses of systemic corticosteroids in past year
- Overuse of SABAs (>1 canister/month)
- Currently not on ICS or non-adherent
PART 9: SPECIAL SCENARIOS (Detailed)
9.1 Exercise-Induced Bronchoconstriction (EIB)
- Exercise → hyperventilation → desiccation of airway lining fluid → osmolarity change in airway surface liquid → mast cell degranulation → mediator release (LTs, PGs, histamine) → bronchoconstriction
- Cold air compounds this (lower absolute moisture; rewarming also causes edema)
- EIB usually peaks 5-15 minutes after exercise and resolves 30-60 min spontaneously
-
10-15% fall in FEV₁ within 15-30 min of standardized exercise challenge
- Distinguish from refractory period (2h window after exercise where subsequent exercise causes less bronchoconstriction - related to mast cell mediator depletion)
- ICS (long-term anti-inflammatory - reduces mast cell activity)
- Pre-treatment: SABA 15-20 min before exercise; or ICS/formoterol (single dose)
- LABAs for occasional exercise: can extend bronchoprotection but NOT recommended for monotherapy
- Warm-up exercises before vigorous activity (exploits refractory period)
- Breathing through nose/warm scarf in cold weather
9.2 Aspirin-Exacerbated Respiratory Disease (AERD)
Aspirin/NSAID → COX-1 inhibition
↓
Arachidonic acid NOT converted to PGs (especially PGE₂ - bronchodilatory)
↓
Shunting → 5-LO pathway → overproduction of CysLTs
↓
Massive bronchoconstriction + rhinorrhoea + urticaria
- Avoid COX-1 inhibitors (aspirin, ibuprofen, naproxen, diclofenac, indomethacin)
- Safe alternatives: Paracetamol (acetaminophen) at low doses; COX-2 selective inhibitors (celecoxib - use cautiously)
- LTRAs (montelukast, zafirlukast) - reduce severity
- Aspirin desensitization: Gradual incremental aspirin doses in supervised setting → tolerance; allows aspirin for cardiovascular disease; reduces polyp recurrence and systemic steroid need
- Dupilumab and tezepelumab show efficacy for AERD-associated nasal polyps
9.3 Asthma-COPD Overlap (ACO)
| Asthma features | COPD features |
|---|---|
| Variable symptoms | ≥10 pack-year smoking history |
| Significant reversibility (≥15% post-BD) | FEV₁/FVC <0.70 post-BD |
| Blood eosinophilia / elevated FeNO | CT emphysema or air trapping |
| History of childhood asthma or atopy | Age >40 |
- ICS are mandatory (reduces mortality in ACO vs ICS withdrawal)
- LABA/LAMA as add-on
- SABA as reliever
- SABA monotherapy is contraindicated in ACO
- Pulmonary rehabilitation for functional limitation
- Manage comorbidities (cardiovascular disease, osteoporosis from long-term OCS)
PART 10: MONITORING FRAMEWORK (GINA 2026)
10.1 Asthma Control Questionnaires
- 5 questions covering past 4 weeks; scored 5-25
- ≤19 = poorly controlled; ≥20 = well controlled; 25 = fully controlled
- 6-7 items; score 0-6; higher = worse control
- Score >1.5 = uncontrolled; <0.75 = controlled
- CAAT (Chronic Airways Assessment Test) - for patients with both asthma and COPD features
- Peds-AIRQ (Pediatric Asthma Impairment and Risk Questionnaire)
- PRAM (Pediatric Respiratory Assessment Measure) - for acute exacerbation severity in children
10.2 Written Asthma Action Plan
- Every patient should have a written action plan
- Based on symptoms or PEFR (green/yellow/red zones)
- Specifies: when to increase reliever, when to start OCS, when to go to ED
- Absence of written plan = fatality risk factor
PART 11: ASTHMA vs COPD at a Glance
| Feature | Asthma | COPD |
|---|---|---|
| Age of onset | Often childhood | Usually >40y |
| Smoking | Usually not | Major cause |
| Atopy | Common | Uncommon |
| Inflammation | Eosinophilic (T2) mainly | Neutrophilic/macrophage |
| Key cytokines | IL-4, IL-5, IL-13 | IL-8, TNF-α, IL-17 |
| Reversibility | Yes (≥12% + 200mL) | Incomplete (<12%) |
| DLCO | Normal | Reduced |
| CT findings | Normal or hyperinflation | Emphysema, air trapping |
| Steroid response | Excellent (T2) | Poor (largely resistant) |
| Mucus plugs | Yes (Curschmann spirals, Charcot-Leyden crystals) | Chronic sputum |
| Progression | Usually stable | Progressive irreversible |
| Biologics | Yes (5 targets approved) | Dupilumab for eos COPD only |
- Harrison's Principles of Internal Medicine 22E (2025), Chapter 298 (Asthma)
- Goodman & Gilman's Pharmacological Basis of Therapeutics, Chapter 44 (Pulmonary Pharmacology)
- Cellular and Molecular Immunology (Abbas), Chapter 20 (Immediate Hypersensitivity)
- Murray & Nadel's Textbook of Respiratory Medicine, Chapters 62, 27 (Asthma Assessment, Sleep)
- Fishman's Pulmonary Diseases and Disorders, Chapter on Asthma
- GINA 2026 Global Strategy Report (released May 5, 2026)
- Systematic Review, PMID 40520782: Umbrella review of biologics for severe asthma (2025)
Create a reference PDF summarizing asthma management algorithms and biologic selection criteria
ls /home/daytona/workspace/ 2>/dev/null || echo "workspace empty"
mkdir -p /home/daytona/workspace/asthma-pdf && python3 -c "from reportlab.lib import colors; print('reportlab ok')" && python3 -c "from reportlab.platypus import SimpleDocTemplate; print('platypus ok')"
~/asthma-pdf/generate_asthma_pdf.py
#!/usr/bin/env python3
"""
Asthma Management Reference PDF
Comprehensive clinical reference for respiratory medicine PGT
Covers: GINA 2026 stepwise management, biologic selection, acute severe asthma, severity assessment
"""
from reportlab.lib.pagesizes import A4
from reportlab.lib import colors
from reportlab.lib.styles import getSampleStyleSheet, ParagraphStyle
from reportlab.lib.units import cm, mm
from reportlab.lib.enums import TA_CENTER, TA_LEFT, TA_JUSTIFY
from reportlab.platypus import (
SimpleDocTemplate, Paragraph, Spacer, Table, TableStyle,
HRFlowable, PageBreak, KeepTogether
)
from reportlab.platypus.flowables import BalancedColumns
from reportlab.graphics.shapes import Drawing, Rect, String, Line, Arrow, Polygon
from reportlab.graphics import renderPDF
from reportlab.graphics.charts.barcharts import VerticalBarChart
from reportlab.pdfgen import canvas
import datetime
# ─────────────────────────── COLOUR PALETTE ───────────────────────────
DARK_BLUE = colors.HexColor('#1A3A5C')
MED_BLUE = colors.HexColor('#2E6DA4')
LIGHT_BLUE = colors.HexColor('#D6E8F7')
TEAL = colors.HexColor('#007B8A')
LIGHT_TEAL = colors.HexColor('#D0F0F3')
GREEN = colors.HexColor('#1E7A45')
LIGHT_GREEN = colors.HexColor('#D4EDDA')
ORANGE = colors.HexColor('#D4600A')
LIGHT_ORANGE = colors.HexColor('#FDEBD0')
RED = colors.HexColor('#B22222')
LIGHT_RED = colors.HexColor('#FADBD8')
YELLOW = colors.HexColor('#856404')
LIGHT_YELLOW = colors.HexColor('#FFF3CD')
PURPLE = colors.HexColor('#5B2C8D')
LIGHT_PURPLE = colors.HexColor('#E8D5F5')
GREY_LIGHT = colors.HexColor('#F5F7FA')
GREY_MED = colors.HexColor('#DEE2E6')
GREY_DARK = colors.HexColor('#6C757D')
WHITE = colors.white
BLACK = colors.black
# ─────────────────────────── PAGE SETUP ───────────────────────────────
OUTPUT = '/home/daytona/workspace/asthma-pdf/Asthma_Management_Reference.pdf'
PAGE_W, PAGE_H = A4
MARGIN = 1.6 * cm
def make_doc():
doc = SimpleDocTemplate(
OUTPUT,
pagesize=A4,
leftMargin=MARGIN, rightMargin=MARGIN,
topMargin=2.2*cm, bottomMargin=2.0*cm,
title='Asthma Management Reference – GINA 2026',
author='Orris Medical AI',
subject='Respiratory Medicine – PGT Reference',
)
return doc
# ─────────────────────────── STYLES ───────────────────────────────────
ss = getSampleStyleSheet()
def S(name, parent='Normal', **kw):
return ParagraphStyle(name, parent=ss[parent], **kw)
COVER_TITLE = S('CoverTitle', 'Normal',
fontSize=28, leading=34, textColor=WHITE,
fontName='Helvetica-Bold', alignment=TA_CENTER)
COVER_SUB = S('CoverSub', 'Normal',
fontSize=14, leading=18, textColor=LIGHT_BLUE,
fontName='Helvetica', alignment=TA_CENTER)
COVER_NOTE = S('CoverNote', 'Normal',
fontSize=9, leading=12, textColor=GREY_MED,
fontName='Helvetica-Oblique', alignment=TA_CENTER)
H1 = S('H1', 'Normal',
fontSize=13, leading=16, textColor=WHITE,
fontName='Helvetica-Bold', alignment=TA_LEFT,
spaceBefore=4, spaceAfter=2,
backColor=DARK_BLUE, borderPadding=(5,8,5,8))
H2 = S('H2', 'Normal',
fontSize=11, leading=14, textColor=DARK_BLUE,
fontName='Helvetica-Bold',
spaceBefore=8, spaceAfter=3,
borderPadding=(0,0,2,0))
H3 = S('H3', 'Normal',
fontSize=9.5, leading=12, textColor=MED_BLUE,
fontName='Helvetica-Bold',
spaceBefore=6, spaceAfter=2)
BODY = S('Body', 'Normal',
fontSize=8.5, leading=12, textColor=BLACK,
fontName='Helvetica',
spaceAfter=3, alignment=TA_JUSTIFY)
BODY_BOLD = S('BodyBold', 'Normal',
fontSize=8.5, leading=12, textColor=DARK_BLUE,
fontName='Helvetica-Bold', spaceAfter=2)
BULLET = S('Bullet', 'Normal',
fontSize=8.5, leading=12, textColor=BLACK,
fontName='Helvetica',
leftIndent=14, firstLineIndent=-10,
spaceAfter=2)
NOTE = S('Note', 'Normal',
fontSize=7.5, leading=10.5, textColor=GREY_DARK,
fontName='Helvetica-Oblique',
leftIndent=4, spaceAfter=2)
WARN = S('Warn', 'Normal',
fontSize=8, leading=11, textColor=RED,
fontName='Helvetica-Bold',
leftIndent=8, spaceAfter=3)
TH = S('TH', 'Normal',
fontSize=8, leading=10, textColor=WHITE,
fontName='Helvetica-Bold', alignment=TA_CENTER)
TC = S('TC', 'Normal',
fontSize=7.8, leading=10.5, textColor=BLACK,
fontName='Helvetica', alignment=TA_LEFT)
TC_C = S('TC_C', 'Normal',
fontSize=7.8, leading=10.5, textColor=BLACK,
fontName='Helvetica', alignment=TA_CENTER)
TC_B = S('TC_B', 'Normal',
fontSize=7.8, leading=10.5, textColor=DARK_BLUE,
fontName='Helvetica-Bold', alignment=TA_LEFT)
FOOTER_STYLE = S('Footer', 'Normal',
fontSize=7, leading=9, textColor=GREY_DARK,
fontName='Helvetica', alignment=TA_CENTER)
# ─────────────────────────── HELPERS ──────────────────────────────────
def HR(color=GREY_MED, width=1, spaceB=4, spaceA=4):
return HRFlowable(width='100%', thickness=width, color=color,
spaceAfter=spaceA, spaceBefore=spaceB)
def SP(h=0.3):
return Spacer(1, h*cm)
def p(text, style=BODY):
return Paragraph(text, style)
def bullet(text, symbol='•'):
return Paragraph(f'{symbol} {text}', BULLET)
def section_header(title, color=DARK_BLUE, text_color=WHITE):
data = [[Paragraph(title, ParagraphStyle('sh', parent=H1,
backColor=color,
textColor=text_color))]]
t = Table(data, colWidths=[PAGE_W - 2*MARGIN])
t.setStyle(TableStyle([
('BACKGROUND', (0,0), (-1,-1), color),
('ROUNDEDCORNERS', [4]),
('TOPPADDING', (0,0), (-1,-1), 5),
('BOTTOMPADDING', (0,0), (-1,-1), 5),
('LEFTPADDING', (0,0), (-1,-1), 10),
]))
return t
def info_box(title, content_paras, bg=LIGHT_BLUE, border=MED_BLUE):
"""A titled info box."""
inner = [[p(title, S('ib_title','Normal',
fontSize=8.5, fontName='Helvetica-Bold',
textColor=border))]]
for c in content_paras:
inner.append([c])
t = Table(inner, colWidths=[PAGE_W - 2*MARGIN - 0.4*cm])
t.setStyle(TableStyle([
('BACKGROUND', (0,0), (-1,-1), bg),
('BOX', (0,0), (-1,-1), 1, border),
('LEFTPADDING', (0,0), (-1,-1), 8),
('RIGHTPADDING', (0,0), (-1,-1), 8),
('TOPPADDING', (0,0), (-1,-1), 4),
('BOTTOMPADDING', (0,0), (-1,-1), 4),
('ROUNDEDCORNERS', [4]),
]))
return t
def make_table(headers, rows, col_widths, header_bg=DARK_BLUE,
row_alt=GREY_LIGHT, zebra=True):
header_row = [Paragraph(h, TH) for h in headers]
data = [header_row]
for i, row in enumerate(rows):
data.append([Paragraph(str(c), TC) if not isinstance(c, Paragraph) else c
for c in row])
t = Table(data, colWidths=col_widths, repeatRows=1)
style = [
('BACKGROUND', (0,0), (-1,0), header_bg),
('GRID', (0,0), (-1,-1), 0.4, GREY_MED),
('ROWBACKGROUNDS', (0,1), (-1,-1), [WHITE, row_alt] if zebra else [WHITE]),
('VALIGN', (0,0), (-1,-1), 'MIDDLE'),
('TOPPADDING', (0,0), (-1,-1), 4),
('BOTTOMPADDING', (0,0), (-1,-1), 4),
('LEFTPADDING', (0,0), (-1,-1), 5),
('RIGHTPADDING', (0,0), (-1,-1), 5),
('FONTNAME', (0,0), (-1,0), 'Helvetica-Bold'),
]
t.setStyle(TableStyle(style))
return t
def colored_cell(text, bg, text_color=BLACK, bold=False):
style = S('cc','Normal', fontSize=7.8, leading=10.5,
textColor=text_color,
fontName='Helvetica-Bold' if bold else 'Helvetica',
alignment=TA_CENTER)
return Paragraph(text, style)
# ─────────────────────── COVER PAGE ──────────────────────────────────
def build_cover(canvas_obj, doc):
canvas_obj.saveState()
# Background gradient-like blocks
canvas_obj.setFillColor(DARK_BLUE)
canvas_obj.rect(0, PAGE_H*0.38, PAGE_W, PAGE_H*0.62, fill=1, stroke=0)
canvas_obj.setFillColor(MED_BLUE)
canvas_obj.rect(0, PAGE_H*0.35, PAGE_W, PAGE_H*0.05, fill=1, stroke=0)
canvas_obj.setFillColor(TEAL)
canvas_obj.rect(0, 0, PAGE_W, PAGE_H*0.35, fill=1, stroke=0)
# Accent line
canvas_obj.setStrokeColor(LIGHT_BLUE)
canvas_obj.setLineWidth(3)
canvas_obj.line(MARGIN, PAGE_H*0.38, PAGE_W - MARGIN, PAGE_H*0.38)
# Title
canvas_obj.setFillColor(WHITE)
canvas_obj.setFont('Helvetica-Bold', 30)
canvas_obj.drawCentredString(PAGE_W/2, PAGE_H*0.72, 'ASTHMA MANAGEMENT')
canvas_obj.setFont('Helvetica-Bold', 24)
canvas_obj.drawCentredString(PAGE_W/2, PAGE_H*0.65, 'CLINICAL REFERENCE')
# Subtitle box
canvas_obj.setFillColor(LIGHT_BLUE)
canvas_obj.roundRect(MARGIN, PAGE_H*0.58, PAGE_W-2*MARGIN, 1.2*cm, 5, fill=1, stroke=0)
canvas_obj.setFillColor(DARK_BLUE)
canvas_obj.setFont('Helvetica-Bold', 12)
canvas_obj.drawCentredString(PAGE_W/2, PAGE_H*0.587, 'Algorithms, Biologic Selection & Acute Management')
# Info boxes in lower section
boxes = [
('GINA 2026', 'Stepwise Management\n5-Step Algorithm'),
('BIOLOGICS', 'Selection Criteria\n8 Approved Agents'),
('ACUTE ASTHMA', 'Severity Grading\nStatus Asthmaticus'),
('BIOMARKERS', 'FeNO · Eosinophils\nIgE · Periostin'),
]
bw = (PAGE_W - 2*MARGIN - 0.3*cm*3) / 4
bx = MARGIN
by = PAGE_H*0.17
for i, (title, desc) in enumerate(boxes):
canvas_obj.setFillColor(colors.HexColor('#1A6B7C'))
canvas_obj.roundRect(bx, by, bw, 2.8*cm, 5, fill=1, stroke=0)
canvas_obj.setStrokeColor(LIGHT_TEAL)
canvas_obj.setLineWidth(1)
canvas_obj.roundRect(bx, by, bw, 2.8*cm, 5, fill=0, stroke=1)
canvas_obj.setFillColor(LIGHT_TEAL)
canvas_obj.setFont('Helvetica-Bold', 9)
canvas_obj.drawCentredString(bx + bw/2, by + 2.0*cm, title)
canvas_obj.setFillColor(WHITE)
canvas_obj.setFont('Helvetica', 7.5)
lines = desc.split('\n')
for j, line in enumerate(lines):
canvas_obj.drawCentredString(bx + bw/2, by + 1.2*cm - j*0.45*cm, line)
bx += bw + 0.3*cm
# Footer
canvas_obj.setFillColor(GREY_LIGHT)
canvas_obj.setFont('Helvetica-Oblique', 7.5)
canvas_obj.drawCentredString(PAGE_W/2, 0.9*cm,
f'Prepared for Respiratory Medicine PGT | Based on GINA 2026, Harrison\'s 22E, Fishman\'s Pulmonary | {datetime.date.today().strftime("%B %Y")}')
canvas_obj.restoreState()
# ─────────────────────── PAGE TEMPLATE ───────────────────────────────
def build_page_header_footer(canvas_obj, doc):
canvas_obj.saveState()
# Header bar
canvas_obj.setFillColor(DARK_BLUE)
canvas_obj.rect(0, PAGE_H - 1.4*cm, PAGE_W, 1.4*cm, fill=1, stroke=0)
canvas_obj.setFillColor(WHITE)
canvas_obj.setFont('Helvetica-Bold', 9)
canvas_obj.drawString(MARGIN, PAGE_H - 0.9*cm, 'ASTHMA MANAGEMENT REFERENCE')
canvas_obj.setFont('Helvetica', 8)
canvas_obj.drawRightString(PAGE_W - MARGIN, PAGE_H - 0.9*cm,
f'GINA 2026 | Harrison\'s 22E | Fishman\'s Pulmonary')
# Footer
canvas_obj.setFillColor(GREY_LIGHT)
canvas_obj.rect(0, 0, PAGE_W, 1.2*cm, fill=1, stroke=0)
canvas_obj.setStrokeColor(GREY_MED)
canvas_obj.setLineWidth(0.5)
canvas_obj.line(0, 1.2*cm, PAGE_W, 1.2*cm)
canvas_obj.setFillColor(GREY_DARK)
canvas_obj.setFont('Helvetica', 7)
canvas_obj.drawCentredString(PAGE_W/2, 0.45*cm,
f'For educational use only – Not for clinical decision-making without specialist review | Page {doc.page}')
canvas_obj.restoreState()
# ─────────────────────────── CONTENT ──────────────────────────────────
def build_story():
story = []
W = PAGE_W - 2*MARGIN # usable width
# ══════════════════════════════════════════════════════════════════
# PAGE 1 – DEFINITION, EPIDEMIOLOGY, DIAGNOSIS OVERVIEW
# ══════════════════════════════════════════════════════════════════
story.append(SP(0.3))
story.append(section_header('1. DEFINITION & KEY CONCEPTS'))
story.append(SP(0.3))
defn_data = [
[Paragraph('<b>ASTHMA</b> is a heterogeneous disease characterised by <b>chronic airway inflammation</b>, '
'<b>airway hyperresponsiveness (AHR)</b>, and <b>variable airflow obstruction</b> that is '
'usually reversible. In a large proportion, inflammation is <i>eosinophilic (T2-high)</i>; '
'some patients present with neutrophilic or paucigranulocytic inflammation (T2-low).', BODY)]
]
t = Table(defn_data, colWidths=[W])
t.setStyle(TableStyle([
('BACKGROUND', (0,0), (-1,-1), LIGHT_BLUE),
('BOX', (0,0), (-1,-1), 1.5, MED_BLUE),
('LEFTPADDING', (0,0), (-1,-1), 10),
('RIGHTPADDING', (0,0), (-1,-1), 10),
('TOPPADDING', (0,0), (-1,-1), 8),
('BOTTOMPADDING', (0,0), (-1,-1), 8),
]))
story.append(t)
story.append(SP(0.4))
# Three-column key facts
facts = [
[Paragraph('<b>GLOBAL BURDEN</b>\n262 million people\nworldwide affected', TC_C),
Paragraph('<b>US PREVALENCE</b>\n7.9% adults\n8.4% children', TC_C),
Paragraph('<b>ECONOMICS</b>\nUS $82 billion/year\ntotal burden (2013)', TC_C),
Paragraph('<b>MORTALITY</b>\n~3–4,000 deaths/year\nin USA; preventable', TC_C)],
]
fact_t = Table(facts, colWidths=[W/4]*4)
fact_t.setStyle(TableStyle([
('BACKGROUND', (0,0), (0,0), LIGHT_BLUE),
('BACKGROUND', (1,0), (1,0), LIGHT_GREEN),
('BACKGROUND', (2,0), (2,0), LIGHT_ORANGE),
('BACKGROUND', (3,0), (3,0), LIGHT_RED),
('BOX', (0,0), (-1,-1), 0.5, GREY_MED),
('INNERGRID', (0,0), (-1,-1), 0.5, GREY_MED),
('ALIGN', (0,0), (-1,-1), 'CENTER'),
('VALIGN', (0,0), (-1,-1), 'MIDDLE'),
('TOPPADDING', (0,0), (-1,-1), 6),
('BOTTOMPADDING', (0,0), (-1,-1), 6),
]))
story.append(fact_t)
story.append(SP(0.5))
# ── DIAGNOSIS CRITERIA ──
story.append(p('DIAGNOSTIC CRITERIA', H2))
story.append(HR(MED_BLUE, 1.5, 2, 5))
diag_headers = ['Criterion', 'Threshold / Finding', 'Notes']
diag_rows = [
[p('<b>Spirometry reversibility</b>', TC_B),
'FEV₁ ↑ ≥12% AND ≥200 mL post-bronchodilator',
'Most specific objective test; confirm before starting ICS if possible'],
[p('<b>PEFR variability</b>', TC_B),
'>10% diurnal variability (am vs pm)',
'Higher variability = worse control; better predictor of exacerbations than single PEFR'],
[p('<b>Methacholine PC₂₀</b>', TC_B),
'<8 mg/mL = significant AHR',
'High sensitivity; false positives in COPD, rhinitis, post-viral; use when spirometry normal'],
[p('<b>Mannitol challenge</b>', TC_B),
'≥15% fall in FEV₁ at ≤635 mg cumulative',
'Higher specificity than methacholine for active asthma'],
[p('<b>FeNO</b>', TC_B),
'≥40 ppb = high T2 inflammation',
'<25 ppb = eosinophilic inflammation less likely; falls with ICS (adherence marker)'],
[p('<b>Trial of ICS therapy</b>', TC_B),
'Significant symptomatic improvement',
'In mild cases where spirometry is normal; confirms diagnosis retrospectively'],
]
story.append(make_table(diag_headers, diag_rows,
[3.5*cm, 6.5*cm, W-10*cm]))
story.append(SP(0.3))
story.append(p('⚠ <b>IMPORTANT:</b> >1/3 of physician-diagnosed asthma does NOT meet objective criteria. '
'Always confirm with spirometry or provocation testing before starting long-term therapy.', WARN))
story.append(SP(0.5))
# ── BIOMARKERS TABLE ──
story.append(p('KEY BIOMARKERS & INTERPRETATION', H2))
story.append(HR(MED_BLUE, 1.5, 2, 5))
bio_headers = ['Biomarker', 'Low', 'Borderline', 'High', 'Clinical Use']
bio_rows = [
['FeNO (ppb)',
colored_cell('<25\nT2-low', LIGHT_GREEN, GREEN, True),
colored_cell('25–39\nBorderline', LIGHT_YELLOW, YELLOW, True),
colored_cell('≥40\nEosinophilic', LIGHT_RED, RED, True),
'T2 phenotyping; ICS response prediction; adherence monitoring; biologic eligibility'],
['Blood Eos (/µL)',
colored_cell('<150\nT2-low', LIGHT_GREEN, GREEN, True),
colored_cell('150–299\nMild T2', LIGHT_YELLOW, YELLOW, True),
colored_cell('≥300\nHigh T2', LIGHT_RED, RED, True),
'Biologic eligibility (mepolizumab ≥150/300, benralizumab ≥300, reslizumab ≥400)'],
['Total IgE (IU/mL)',
colored_cell('<30\nUnlikely allergic', LIGHT_GREEN, GREEN, True),
colored_cell('30–700\nAllergic range', LIGHT_YELLOW, YELLOW, True),
colored_cell('>700\nHigh IgE', LIGHT_RED, RED, True),
'Omalizumab eligibility (IgE 30–700 + perennial allergen sensitisation)'],
['Sputum Eos (%)',
colored_cell('<2%\nNormal', LIGHT_GREEN, GREEN, True),
colored_cell('2–3%\nMild eos', LIGHT_YELLOW, YELLOW, True),
colored_cell('≥3%\nEosinophilic', LIGHT_RED, RED, True),
'Gold standard for T2 phenotyping; ICS dose titration in severe asthma'],
['Periostin (ng/mL)',
colored_cell('<25\nLow', LIGHT_GREEN, GREEN, True),
colored_cell('25–50\nModerate', LIGHT_YELLOW, YELLOW, True),
colored_cell('>50\nHigh (esp. AERD)', LIGHT_RED, RED, True),
'T2 inflammation marker; highest in AERD (mean 64.7); predicts dupilumab response'],
]
t = make_table(bio_headers, bio_rows,
[2.8*cm, 2.2*cm, 2.2*cm, 2.2*cm, W-9.4*cm])
story.append(t)
story.append(PageBreak())
# ══════════════════════════════════════════════════════════════════
# PAGE 2 – GINA 2026 STEPWISE MANAGEMENT
# ══════════════════════════════════════════════════════════════════
story.append(SP(0.2))
story.append(section_header('2. GINA 2026 STEPWISE MANAGEMENT ALGORITHM', TEAL))
story.append(SP(0.3))
# Key paradigm box
story.append(info_box(
'🔑 KEY PARADIGM CHANGE – GINA 2026 (Anti-Inflammatory Reliever, AIR)',
[
p('<b>ICS/formoterol as reliever at ALL steps</b> – replacing SABA-only approach. '
'Using ICS/formoterol as-needed ensures anti-inflammatory therapy accompanies '
'every bronchodilator dose, reducing severe exacerbations and OCS use.', BODY),
p('<b>ICS-formoterol (MART strategy)</b> = Maintenance And Reliever Therapy: '
'same inhaler used for both daily controller AND as-needed relief at steps 3–4.', BODY),
p('<b>Never use LABA as monotherapy</b> in asthma. LABAs must always be combined with ICS.', WARN),
], LIGHT_TEAL, TEAL))
story.append(SP(0.4))
# 5-Step Table
step_colors = [LIGHT_GREEN, LIGHT_BLUE, LIGHT_YELLOW, LIGHT_ORANGE, LIGHT_RED]
step_borders = [GREEN, MED_BLUE, YELLOW, ORANGE, RED]
step_labels = ['STEP 1', 'STEP 2', 'STEP 3', 'STEP 4', 'STEP 5']
step_severity = ['Intermittent\n(<2×/month)', 'Mild persistent\n(≥2×/month,\nnot daily)',
'Moderate\n(daily symptoms)', 'Severe\n(uncontrolled\non step 3)',
'Very severe\n(uncontrolled\non step 4)']
step_controller = [
'As-needed\nlow-dose\nICS-formoterol*',
'Low-dose ICS daily\n+ as-needed\nICS-formoterol*',
'Low-dose\nICS/LABA\n(daily)',
'Medium-dose\nICS/LABA\n(daily)',
'High-dose ICS/LABA\n+ phenotypic\nassessment\n± biologic therapy',
]
step_reliever = ['ICS/formoterol\n(AIR)'] * 5
step_alt = [
'Low-dose ICS\nwith each SABA†',
'LTRA (note:\nmontelukast\nwarning!)',
'Medium-dose ICS\nor low-dose\nICS + LTRA',
'Add LAMA\n(tiotropium)\nor add LTRA',
'Low-dose OCS\n(last resort;\nconsider side-effects)',
]
step_data = [
[Paragraph('<b>STEP</b>', TH),
Paragraph('<b>SEVERITY</b>', TH),
Paragraph('<b>PREFERRED\nCONTROLLER</b>', TH),
Paragraph('<b>PREFERRED\nRELIEVER</b>', TH),
Paragraph('<b>ALTERNATIVE /\nADD-ON OPTIONS</b>', TH)],
]
for i in range(5):
step_data.append([
colored_cell(step_labels[i], step_colors[i],
step_borders[i], True),
Paragraph(step_severity[i], TC_C),
Paragraph(step_controller[i], TC_C),
Paragraph(step_reliever[i], TC_C),
Paragraph(step_alt[i], TC),
])
step_t = Table(step_data, colWidths=[1.6*cm, 2.8*cm, 3.6*cm, 2.6*cm, W-10.6*cm],
repeatRows=1)
step_t.setStyle(TableStyle([
('BACKGROUND', (0,0), (-1,0), DARK_BLUE),
('TEXTCOLOR', (0,0), (-1,0), WHITE),
('GRID', (0,0), (-1,-1), 0.5, GREY_MED),
('VALIGN', (0,0), (-1,-1), 'MIDDLE'),
('ALIGN', (0,0), (-1,-1), 'CENTER'),
('TOPPADDING', (0,0), (-1,-1), 5),
('BOTTOMPADDING', (0,0), (-1,-1), 5),
('ROWBACKGROUNDS', (0,1), (-1,-1),
[LIGHT_GREEN, LIGHT_BLUE, LIGHT_YELLOW, LIGHT_ORANGE, LIGHT_RED]),
]))
story.append(step_t)
story.append(SP(0.25))
# Footnotes
story.append(p('* As-needed ICS-formoterol = Anti-Inflammatory Reliever (AIR); preferred at all steps per GINA 2026. '
'† NAEPP alternative: ICS taken whenever SABA taken (step 1). '
'‡ ICS/formoterol MART = same inhaler for controller + reliever (steps 3–4).', NOTE))
story.append(SP(0.4))
# Stepping up/down rules
story.append(p('STEPPING UP / DOWN RULES', H2))
story.append(HR(TEAL, 1.5, 2, 5))
updown_data = [
[Paragraph('<b>Before Stepping UP – Check First:</b>', TC_B),
Paragraph('<b>Stepping DOWN – When to:</b>', TC_B)],
[Paragraph('✓ Inhaler technique correct?\n'
'✓ Adherence adequate (>80%)?\n'
'✓ Trigger avoidance addressed?\n'
'✓ Comorbidities treated (GERD, rhinitis, OSA, VCD)?\n'
'✓ Diagnosis confirmed (not VCD/HF mimicking asthma)?\n\n'
'Step up only if poor control persists ≥2–3 months\n'
'after all of the above are optimised.', BODY),
Paragraph('✓ Asthma well-controlled for ≥3 months\n'
'✓ No exacerbations, normal FEV₁\n'
'✓ Not high-risk season (e.g., viral season)\n\n'
'⚠ NEVER fully stop ICS (even in step 1)\n'
'⚠ ICS dose reductions: decrease by 25–50% every 3 months\n'
'⚠ ICS discontinuation risks exacerbation and rebound eosinophilia', BODY)],
]
updown_t = Table(updown_data, colWidths=[W/2, W/2])
updown_t.setStyle(TableStyle([
('BACKGROUND', (0,0), (-1,0), LIGHT_TEAL),
('BACKGROUND', (0,1), (0,1), LIGHT_GREEN),
('BACKGROUND', (1,1), (1,1), LIGHT_YELLOW),
('GRID', (0,0), (-1,-1), 0.5, GREY_MED),
('VALIGN', (0,0), (-1,-1), 'TOP'),
('TOPPADDING', (0,0), (-1,-1), 6),
('BOTTOMPADDING', (0,0), (-1,-1), 6),
('LEFTPADDING', (0,0), (-1,-1), 8),
('RIGHTPADDING', (0,0), (-1,-1), 8),
]))
story.append(updown_t)
story.append(SP(0.4))
# OCS minimisation (GINA 2026 new)
story.append(info_box(
'OCS MINIMISATION – GINA 2026 New Recommendation',
[
bullet('All patients must receive <b>ICS-containing therapy</b> – this is non-negotiable.'),
bullet('ICS-formoterol AIR or ICS-SABA reduces risk of severe exacerbations requiring OCS.'),
bullet('Optimise modifiable risk factors before adding OCS (see comorbidities).'),
bullet('If OCS required long-term → refer for phenotyping + biologic therapy assessment.'),
p('OCS side effects: Diabetes, osteoporosis, HPA axis suppression, cataracts, '
'weight gain, immunosuppression, hypertension, avascular necrosis.', NOTE),
], LIGHT_YELLOW, ORANGE))
story.append(PageBreak())
# ══════════════════════════════════════════════════════════════════
# PAGE 3 – BIOLOGIC SELECTION
# ══════════════════════════════════════════════════════════════════
story.append(SP(0.2))
story.append(section_header('3. BIOLOGIC THERAPY – TARGETS, ELIGIBILITY & SELECTION', PURPLE))
story.append(SP(0.3))
story.append(p('Biologics are used at <b>Step 5</b> (or after Step 4 failure). All current approved biologics '
'target the <b>T2 inflammatory cascade</b>. Selection is based on biomarker profile, '
'comorbidities, route/frequency preference, and cost.', BODY))
story.append(SP(0.3))
# T2 cascade summary
cascade_data = [
[Paragraph('<b>Epithelial Alarmins</b>\n(upstream)', TC_C),
Paragraph('→', TC_C),
Paragraph('<b>ILC2 / Th2</b>\nActivation', TC_C),
Paragraph('→', TC_C),
Paragraph('<b>IL-4, IL-5, IL-13</b>\n(effector cytokines)', TC_C),
Paragraph('→', TC_C),
Paragraph('<b>IgE · Eosinophils\nMucus · AHR · Fibrosis</b>', TC_C)],
[Paragraph('TSLP, IL-33, IL-25', NOTE),
Paragraph('', TC_C),
Paragraph('', TC_C),
Paragraph('', TC_C),
Paragraph('IL-4 → IgE switching\nIL-5 → Eosinophil Δ\nIL-13 → Mucus, AHR', NOTE),
Paragraph('', TC_C),
Paragraph('', TC_C)],
]
cascade_t = Table(cascade_data, colWidths=[2.8*cm,0.6*cm,2.4*cm,0.6*cm,3.2*cm,0.6*cm,W-10.2*cm])
cascade_t.setStyle(TableStyle([
('BACKGROUND', (0,0), (0,-1), LIGHT_PURPLE),
('BACKGROUND', (2,0), (2,-1), LIGHT_TEAL),
('BACKGROUND', (4,0), (4,-1), LIGHT_BLUE),
('BACKGROUND', (6,0), (6,-1), LIGHT_RED),
('BOX', (0,0), (0,-1), 0.5, PURPLE),
('BOX', (2,0), (2,-1), 0.5, TEAL),
('BOX', (4,0), (4,-1), 0.5, MED_BLUE),
('BOX', (6,0), (6,-1), 0.5, RED),
('ALIGN', (0,0), (-1,-1), 'CENTER'),
('VALIGN', (0,0), (-1,-1), 'MIDDLE'),
('TOPPADDING', (0,0), (-1,-1), 4),
('BOTTOMPADDING', (0,0), (-1,-1), 4),
]))
story.append(cascade_t)
story.append(SP(0.4))
# Biologic table
story.append(p('APPROVED BIOLOGICS – COMPREHENSIVE COMPARISON', H2))
story.append(HR(PURPLE, 1.5, 2, 5))
bio_t_headers = ['Agent', 'Target', 'Route /\nFreq.', 'Eos\nThreshold', 'IgE\nRange',
'Key Indications / Notes']
bio_t_rows = [
[p('<b>Omalizumab</b>\n(Xolair)', TC_B),
'Anti-IgE', 'SC\nq2–4w',
p('Not required\n(IgE-based)', TC_C),
p('30–700\nIU/mL', TC_C),
'Perennial allergen sensitisation + IgE 30–700; also: CRSwNP, chronic urticaria; reduces exacerb. 25–50%'],
[p('<b>Omalizumab-igec</b>\n(biosimilar) ★NEW 2026', TC_B),
'Anti-IgE', 'SC\nq2–4w',
p('Not required', TC_C),
p('30–700\nIU/mL', TC_C),
'Biosimilar of omalizumab; GINA 2026: now approved for CRSwNP'],
[p('<b>Mepolizumab</b>\n(Nucala)', TC_B),
'Anti-IL-5', 'SC 100mg\nq4w',
p('≥150 screen\n≥300 preferred', TC_C),
p('N/A', TC_C),
'Also: EGPA, HES, CRSwNP; reduces exacerb. ~50%; reduces OCS use; weight-independent dose'],
[p('<b>Reslizumab</b>\n(Cinqair)', TC_B),
'Anti-IL-5', 'IV 3mg/kg\nq4w',
p('≥400/µL', TC_C),
p('N/A', TC_C),
'Only IV biologic for asthma; weight-based dosing; reduces exacerb. ~50%; anaphylaxis risk (0.3%)'],
[p('<b>Benralizumab</b>\n(Fasenra)', TC_B),
'Anti-IL-5Rα', 'SC 30mg\nq4w ×3\nthen q8w',
p('≥300/µL', TC_C),
p('N/A', TC_C),
'Near-complete eosinophil depletion via ADCC; also CRSwNP; convenient q8w maintenance'],
[p('<b>Depemokimab</b>\n(Slynd) ★GINA 2026', TC_B),
'Anti-IL-5\n(long-acting)', 'SC\nq6 months',
p('≥300/µL', TC_C),
p('N/A', TC_C),
'★ NEWEST biologic (GINA 2026); longest dosing interval; ≥12y severe eos asthma; ≥18y CRSwNP'],
[p('<b>Dupilumab</b>\n(Dupixent)', TC_B),
'Anti-IL-4Rα\n(blocks IL-4\n+ IL-13)', 'SC\nq2w',
p('≥150/µL or\nFeNO ≥25ppb', TC_C),
p('N/A', TC_C),
'Broadest T2 coverage; also: atopic dermatitis, CRSwNP, eosinophilic oesophagitis, COPD with eos; arthralgia SE'],
[p('<b>Tezepelumab</b>\n(Tezspire)', TC_B),
'Anti-TSLP\n(upstream\nalarmin)', 'SC 210mg\nq4w',
p('NONE\nrequired', TC_C),
p('N/A', TC_C),
'Broadest efficacy including T2-low/paucigranulocytic; works even with low eos/FeNO; also CRSwNP'],
]
story.append(make_table(bio_t_headers, bio_t_rows,
[2.5*cm, 2.0*cm, 1.8*cm, 1.8*cm, 1.5*cm, W-9.6*cm],
header_bg=PURPLE))
story.append(SP(0.3))
story.append(p('ADCC = Antibody-Dependent Cell-mediated Cytotoxicity. EGPA = Eosinophilic Granulomatosis with Polyangiitis. '
'HES = Hypereosinophilic Syndrome. CRSwNP = Chronic Rhinosinusitis with Nasal Polyps. '
'★ = new/updated in GINA 2026.', NOTE))
story.append(SP(0.4))
# Biologic selection algorithm
story.append(p('BIOLOGIC SELECTION ALGORITHM (GINA 2026)', H2))
story.append(HR(PURPLE, 1.5, 2, 5))
algo_data = [
[Paragraph('<b>Step 5 Severe Asthma – Assess T2 Biomarkers</b>', TH),
Paragraph('<b>Biologic of Choice</b>', TH),
Paragraph('<b>Key Consideration</b>', TH)],
[Paragraph('<b>Allergic</b>: IgE 30–700 IU/mL + perennial\nallergen sensitisation (any eos level)', TC_B),
colored_cell('OMALIZUMAB\nor biosimilar', LIGHT_PURPLE, PURPLE, True),
'Skin prick test / RAST positive; also consider if CRSwNP present'],
[Paragraph('<b>Eosinophilic</b>: Blood eos ≥300/µL\n(no allergic features / IgE not eligible)', TC_B),
colored_cell('MEPOLIZUMAB\nBENRALIZUMAB\nDEPEMABOKIMAB★', LIGHT_RED, RED, True),
'Depemokimab preferred if 6-monthly dosing desired; benralizumab for q8w maintenance'],
[Paragraph('<b>High eosinophils</b>: Blood eos ≥400/µL\n(overweight/obese patient)', TC_B),
colored_cell('RESLIZUMAB\n(IV, weight-based)', LIGHT_ORANGE, ORANGE, True),
'Weight-based dosing may be advantageous in obese patients'],
[Paragraph('<b>T2 + Atopic dermatitis, CRSwNP, or\neosinophilic oesophagitis comorbidity</b>', TC_B),
colored_cell('DUPILUMAB\n(IL-4Rα)', LIGHT_BLUE, MED_BLUE, True),
'"One airway, one disease" – addresses multiple atopic manifestations simultaneously'],
[Paragraph('<b>Uncertain T2 phenotype</b>: Low eos, low FeNO;\nor T2-low / paucigranulocytic', TC_B),
colored_cell('TEZEPELUMAB\n(anti-TSLP)', LIGHT_TEAL, TEAL, True),
'Only biologic with no minimum biomarker threshold; broadest efficacy spectrum'],
[Paragraph('<b>Multiple positive biomarkers</b>: Elevated eos\nAND elevated IgE AND high FeNO', TC_B),
colored_cell('SELECT BASED ON:\nComorbidities / Cost\nRoute / Frequency', LIGHT_GREEN, GREEN, True),
'No head-to-head RCTs; GINA 2026 decision tree uses comorbidities + patient preference'],
]
algo_t = Table(algo_data, colWidths=[5.5*cm, 3.8*cm, W-9.3*cm], repeatRows=1)
algo_t.setStyle(TableStyle([
('BACKGROUND', (0,0), (-1,0), PURPLE),
('TEXTCOLOR', (0,0), (-1,0), WHITE),
('GRID', (0,0), (-1,-1), 0.5, GREY_MED),
('ROWBACKGROUNDS', (0,1), (-1,-1), [WHITE, GREY_LIGHT]),
('VALIGN', (0,0), (-1,-1), 'MIDDLE'),
('TOPPADDING', (0,0), (-1,-1), 5),
('BOTTOMPADDING', (0,0), (-1,-1), 5),
('LEFTPADDING', (0,0), (-1,-1), 5),
('RIGHTPADDING', (0,0), (-1,-1), 5),
]))
story.append(algo_t)
story.append(PageBreak())
# ══════════════════════════════════════════════════════════════════
# PAGE 4 – ACUTE SEVERE ASTHMA / STATUS ASTHMATICUS
# ══════════════════════════════════════════════════════════════════
story.append(SP(0.2))
story.append(section_header('4. ACUTE SEVERE ASTHMA & STATUS ASTHMATICUS', RED))
story.append(SP(0.3))
# ABG evolution
story.append(p('ABG EVOLUTION IN ACUTE ASTHMA ATTACK', H2))
story.append(HR(RED, 1.5, 2, 5))
abg_data = [
[Paragraph('<b>Stage</b>', TH),
Paragraph('<b>PaO₂</b>', TH),
Paragraph('<b>PaCO₂</b>', TH),
Paragraph('<b>pH</b>', TH),
Paragraph('<b>SpO₂</b>', TH),
Paragraph('<b>Interpretation / Action</b>', TH)],
[colored_cell('EARLY\nMILD', LIGHT_GREEN, GREEN, True),
colored_cell('Normal\nor ↓ mildly', LIGHT_GREEN, GREEN),
colored_cell('↓ <40\nHypocapnia', LIGHT_GREEN, GREEN, True),
colored_cell('↑ >7.45\nAlkalosis', LIGHT_GREEN, GREEN),
colored_cell('>95%', LIGHT_GREEN, GREEN),
'Tachypnoea compensates; hyperventilation. Treat with SABA + ICS.'],
[colored_cell('MODERATE', LIGHT_YELLOW, YELLOW, True),
colored_cell('↓ 60–80', LIGHT_YELLOW, YELLOW),
colored_cell('Normal\n~35–45\n⚠ DANGER', LIGHT_RED, RED, True),
colored_cell('Normal\n7.40–7.45', LIGHT_YELLOW, YELLOW),
colored_cell('90–95%', LIGHT_YELLOW, YELLOW),
'⚠ NORMAL PaCO₂ in DISTRESSED asthmatic = impending respiratory failure. Aggressive treatment.'],
[colored_cell('SEVERE /\nFAILURE', LIGHT_RED, RED, True),
colored_cell('↓↓ <60', LIGHT_RED, RED),
colored_cell('↑ >45\nHypercapnia', LIGHT_RED, RED, True),
colored_cell('↓ <7.35\nAcidosis', LIGHT_RED, RED, True),
colored_cell('<90%', LIGHT_RED, RED),
'⚠ INTUBATE. Permissive hypercapnia strategy. Aim pH ≥7.2; bicarbonate if needed.'],
]
abg_t = Table(abg_data, colWidths=[1.8*cm, 1.8*cm, 2.5*cm, 2.2*cm, 1.8*cm, W-10.1*cm],
repeatRows=1)
abg_t.setStyle(TableStyle([
('BACKGROUND', (0,0), (-1,0), RED),
('GRID', (0,0), (-1,-1), 0.5, GREY_MED),
('VALIGN', (0,0), (-1,-1), 'MIDDLE'),
('ALIGN', (0,0), (-1,0), 'CENTER'),
('TOPPADDING', (0,0), (-1,-1), 5),
('BOTTOMPADDING', (0,0), (-1,-1), 5),
('LEFTPADDING', (0,0), (-1,-1), 5),
('RIGHTPADDING', (0,0), (-1,-1), 5),
]))
story.append(abg_t)
story.append(SP(0.3))
# Severity grading
story.append(p('SEVERITY GRADING', H2))
story.append(HR(RED, 1.5, 2, 5))
sev_headers = ['Feature', 'Mild-Moderate', 'Severe', 'Life-Threatening']
sev_rows = [
['Speech', 'Full sentences', 'Phrases', 'Words / unable to speak'],
['RR (breaths/min)', '20–25', '25–30', '>30'],
['HR (bpm)', '<110', '110–120', '>120'],
['PEFR (% best/predicted)', '>50–75%', '33–50%', '<33% ("brittle")'],
['SpO₂', '>95%', '92–95%', '<92%'],
['Wheeze', 'Moderate', 'Loud', '★ SILENT CHEST (DANGER)'],
['Mental status', 'Normal', 'Agitated', '★ Drowsy / confused'],
['PaCO₂', '<40 (hypocapnia)', '<40', '★ ≥45 (fatigue/failure)'],
]
sev_col = [4.0*cm, 3.5*cm, 3.0*cm, W-10.5*cm]
data = [[Paragraph(h, TH) for h in sev_headers]] + \
[[Paragraph(str(r[i]), TC) for i in range(4)] for r in sev_rows]
# Highlight danger signs in last column
for i, r in enumerate(sev_rows):
if '★' in r[3]:
data[i+1][3] = Paragraph(r[3].replace('★',''), WARN)
sev_t = Table(data, colWidths=sev_col, repeatRows=1)
sev_t.setStyle(TableStyle([
('BACKGROUND', (0,0), (-1,0), RED),
('GRID', (0,0), (-1,-1), 0.5, GREY_MED),
('ROWBACKGROUNDS', (0,1), (-1,-1), [WHITE, GREY_LIGHT]),
('VALIGN', (0,0), (-1,-1), 'MIDDLE'),
('TOPPADDING', (0,0), (-1,-1), 4),
('BOTTOMPADDING', (0,0), (-1,-1), 4),
('LEFTPADDING', (0,0), (-1,-1), 5),
('RIGHTPADDING', (0,0), (-1,-1), 5),
# Highlight life-threatening column
('BACKGROUND', (3,1), (3,-1), colors.HexColor('#FFF5F5')),
('TEXTCOLOR', (3,1), (3,-1), RED),
]))
story.append(sev_t)
story.append(SP(0.3))
# Management protocol
story.append(p('ACUTE MANAGEMENT PROTOCOL (GINA 2026)', H2))
story.append(HR(RED, 1.5, 2, 5))
mgmt_data = [
[Paragraph('<b>TIME</b>', TH),
Paragraph('<b>INTERVENTION</b>', TH),
Paragraph('<b>DOSE / DETAILS</b>', TH)],
[colored_cell('0–20 min\nIMM-\nEDIATE', LIGHT_RED, RED, True),
Paragraph('1. Supplemental O₂\n2. SABA (salbutamol)\n3. Ipratropium bromide\n4. Systemic corticosteroids', TC_B),
Paragraph('SpO₂ target 93–95% (avoid hyperoxia, GINA 2026)\n'
'MDI+spacer: 4–8 puffs; or nebuliser 2.5–5mg; repeat ×3 q20min\n'
'4–8 puffs MDI or 0.5mg neb; with each salbutamol dose (up to ×3)\n'
'Prednisolone 40–50mg PO or Hydrocortisone 100–200mg IV', TC)],
[colored_cell('1–2 h\nNO RESP-\nONSE', LIGHT_ORANGE, ORANGE, True),
Paragraph('5. IV Magnesium sulfate\n6. IV salbutamol infusion\n7. IV aminophylline\n8. Measure PEFR/FEV₁', TC_B),
Paragraph('2g IV over 20 min (single dose); reduces hospitalisation + intubation\n'
'5–15 mcg/kg/min; continuous; if not responding to inhaled\n'
'Loading 5mg/kg over 20min (if not on oral theophylline); rarely used\n'
'PEFR >60% → likely discharge with step-up; <60% → admit', TC)],
[colored_cell('If\nFAILING', LIGHT_RED, RED, True),
Paragraph('9. NIV (BiPAP)\n10. Heliox\n11. INTUBATION', TC_B),
Paragraph('BiPAP well-tolerated; reduces intubation rate; avoids ICU in selected patients\n'
'60:40 He:O₂; reduces turbulence; decreases WOB; use while preparing for intubation\n'
'RSI with KETAMINE (preferred: bronchodilator properties); avoid propofol if hypotensive', TC)],
[colored_cell('MV\nSTRATEGY', GREY_DARK, WHITE, True),
Paragraph('Mechanical ventilation\nin status asthmaticus', TC_B),
Paragraph('Low RR (8–12/min); low TV (6–8 mL/kg IBW); long expiratory time (I:E 1:3 or 1:4)\n'
'Permissive hypercapnia: allow PaCO₂ to rise; target pH ≥7.2; NaHCO₃ if pH <7.2\n'
'Monitor auto-PEEP (dynamic hyperinflation); consider NMB short-term\n'
'Volatile anaesthetics (isoflurane/sevoflurane) for refractory bronchospasm', TC)],
]
mgmt_t = Table(mgmt_data, colWidths=[2.2*cm, 4.8*cm, W-7.0*cm], repeatRows=1)
mgmt_t.setStyle(TableStyle([
('BACKGROUND', (0,0), (-1,0), RED),
('GRID', (0,0), (-1,-1), 0.5, GREY_MED),
('VALIGN', (0,0), (-1,-1), 'MIDDLE'),
('TOPPADDING', (0,0), (-1,-1), 5),
('BOTTOMPADDING', (0,0), (-1,-1), 5),
('LEFTPADDING', (0,0), (-1,-1), 5),
('RIGHTPADDING', (0,0), (-1,-1), 5),
]))
story.append(mgmt_t)
story.append(SP(0.3))
# ATS/IDSA severe criteria
story.append(info_box(
'ATS/IDSA CRITERIA FOR SEVERE / ICU ASTHMA',
[
p('<b>Major criteria (1 = ICU):</b> Invasive mechanical ventilation; '
'haemodynamic compromise requiring vasopressor support', BODY),
p('<b>Minor criteria (≥3 = ICU):</b> RR ≥30; PaO₂/FiO₂ ≤250; multilobar infiltrates; '
'confusion/disorientation; uremia (BUN ≥20 mg/dL); WBC <4000 cells/mm³; '
'platelets <100,000; hypothermia (<36°C); hypotension requiring aggressive fluid resuscitation', BODY),
], LIGHT_RED, RED))
story.append(PageBreak())
# ══════════════════════════════════════════════════════════════════
# PAGE 5 – ASTHMA MORTALITY RISK & SPECIAL SITUATIONS
# ══════════════════════════════════════════════════════════════════
story.append(SP(0.2))
story.append(section_header('5. MORTALITY RISK FACTORS & SPECIAL CLINICAL SCENARIOS', ORANGE))
story.append(SP(0.3))
# Mortality risk factors
story.append(p('FATALITY RISK INDICATORS (GINA 2026 – NEW EMPHASIS)', H2))
story.append(HR(ORANGE, 1.5, 2, 5))
risk_col1 = [
'<b>1.</b> Previous near-fatal attack (intubation / ICU)',
'<b>2.</b> Hospitalisation for asthma in past 12 months',
'<b>3.</b> ≥2 ED visits in past 6 months',
'<b>4.</b> ≥2 courses of systemic corticosteroids in past year',
'<b>5.</b> Overuse of SABAs (>1 canister/month)',
'<b>6.</b> Currently not using ICS or non-adherent to ICS',
]
risk_col2 = [
'<b>7.</b> No written asthma action plan',
'<b>8.</b> Illicit drug use',
'<b>9.</b> Depression or anxiety',
'<b>10.</b> Severe psychosocial problems',
'<b>11.</b> Lower socioeconomic status / limited healthcare access',
'<b>12.</b> Food allergy + confirmed asthma (anaphylaxis risk)',
]
risk_data = [
[Paragraph('<b>⚠ HIGH-RISK PATIENT INDICATORS</b>', TH),
Paragraph('<b>⚠ FURTHER RISK FACTORS</b>', TH)],
]
for i in range(6):
risk_data.append([
Paragraph(risk_col1[i], BODY),
Paragraph(risk_col2[i], BODY),
])
risk_t = Table(risk_data, colWidths=[W/2, W/2])
risk_t.setStyle(TableStyle([
('BACKGROUND', (0,0), (-1,0), ORANGE),
('ROWBACKGROUNDS', (0,1), (-1,-1), [LIGHT_ORANGE, WHITE]),
('GRID', (0,0), (-1,-1), 0.5, GREY_MED),
('VALIGN', (0,0), (-1,-1), 'MIDDLE'),
('TOPPADDING', (0,0), (-1,-1), 5),
('BOTTOMPADDING', (0,0), (-1,-1), 5),
('LEFTPADDING', (0,0), (-1,-1), 8),
('RIGHTPADDING', (0,0), (-1,-1), 8),
]))
story.append(risk_t)
story.append(SP(0.4))
# Special scenarios
story.append(p('SPECIAL CLINICAL SCENARIOS', H2))
story.append(HR(ORANGE, 1.5, 2, 5))
# Two-column layout for special scenarios
col_w = (W - 0.4*cm) / 2
# AERD
aerd_data = [
[Paragraph('<b>ASPIRIN-EXACERBATED RESPIRATORY DISEASE (AERD)</b>', TC_B)],
[Paragraph('<b>Triad:</b> Asthma + Nasal polyposis + NSAID/aspirin sensitivity\n'
'<b>Mechanism:</b> COX-1 inhibition → ↓PGE₂ + ↑CysLTs → bronchoconstriction\n'
'<b>Diagnosis:</b> Aspirin oral/inhalation challenge (gold standard)\n'
'<b>Tx:</b> Avoid COX-1 inhibitors; LTRAs; aspirin desensitisation; dupilumab/tezepelumab for nasal polyps\n'
'<b>Periostin:</b> Highest among asthma endotypes (mean 64.7 ng/mL)', BODY)],
]
aerd_t = Table(aerd_data, colWidths=[col_w])
aerd_t.setStyle(TableStyle([
('BACKGROUND', (0,0), (-1,-1), LIGHT_ORANGE),
('BOX', (0,0), (-1,-1), 1, ORANGE),
('LEFTPADDING', (0,0), (-1,-1), 7),
('RIGHTPADDING', (0,0), (-1,-1), 7),
('TOPPADDING', (0,0), (-1,-1), 5),
('BOTTOMPADDING', (0,0), (-1,-1), 5),
]))
# ACO
aco_data = [
[Paragraph('<b>ASTHMA-COPD OVERLAP (ACO)</b>', TC_B)],
[Paragraph('<b>Features:</b> Variable symptoms (asthma) + incomplete reversibility + smoking history (COPD)\n'
'<b>Spirometry:</b> Partial reversibility; FEV₁/FVC <0.70 post-BD\n'
'<b>Key rule:</b> ICS is MANDATORY (reduces mortality vs withdrawal)\n'
'<b>Add-on:</b> LABA + LAMA both may be used\n'
'⚠ SABA monotherapy is CONTRAINDICATED in ACO', BODY)],
]
aco_t = Table(aco_data, colWidths=[col_w])
aco_t.setStyle(TableStyle([
('BACKGROUND', (0,0), (-1,-1), LIGHT_TEAL),
('BOX', (0,0), (-1,-1), 1, TEAL),
('LEFTPADDING', (0,0), (-1,-1), 7),
('RIGHTPADDING', (0,0), (-1,-1), 7),
('TOPPADDING', (0,0), (-1,-1), 5),
('BOTTOMPADDING', (0,0), (-1,-1), 5),
]))
# Pregnancy
preg_data = [
[Paragraph('<b>ASTHMA IN PREGNANCY</b>', TC_B)],
[Paragraph('<b>~4%</b> of pregnant women have asthma; 1/3 worsen during pregnancy\n'
'<b>Risk:</b> Moderate-severe asthma → preterm labour, LBW, perinatal death, pre-eclampsia\n'
'<b>ABG normal:</b> pH 7.45, PaCO₂ 27–32 mmHg → "normal" PaCO₂ 40 = hypercapnia!\n'
'<b>FEV₁ and PEFR:</b> Unchanged in pregnancy – useful for monitoring\n'
'<b>Safety:</b> ICS (all safe); salbutamol safe; montelukast avoid if possible', BODY)],
]
preg_t = Table(preg_data, colWidths=[col_w])
preg_t.setStyle(TableStyle([
('BACKGROUND', (0,0), (-1,-1), LIGHT_PURPLE),
('BOX', (0,0), (-1,-1), 1, PURPLE),
('LEFTPADDING', (0,0), (-1,-1), 7),
('RIGHTPADDING', (0,0), (-1,-1), 7),
('TOPPADDING', (0,0), (-1,-1), 5),
('BOTTOMPADDING', (0,0), (-1,-1), 5),
]))
# EIB
eib_data = [
[Paragraph('<b>EXERCISE-INDUCED BRONCHOCONSTRICTION (EIB)</b>', TC_B)],
[Paragraph('<b>Mechanism:</b> Hyperventilation → airway desiccation → osmolarity change → mediator release\n'
'<b>Peak:</b> 5–15 min post-exercise; resolves 30–60 min spontaneously\n'
'<b>Diagnosis:</b> >10–15% fall in FEV₁ at 15–30 min post-exercise challenge\n'
'<b>Refractory period:</b> 2h window after exercise → less bronchoconstriction (mast cell depletion)\n'
'<b>Rx:</b> Pre-treatment SABA 15–20 min before; warm-up; ICS long-term', BODY)],
]
eib_t = Table(eib_data, colWidths=[col_w])
eib_t.setStyle(TableStyle([
('BACKGROUND', (0,0), (-1,-1), LIGHT_GREEN),
('BOX', (0,0), (-1,-1), 1, GREEN),
('LEFTPADDING', (0,0), (-1,-1), 7),
('RIGHTPADDING', (0,0), (-1,-1), 7),
('TOPPADDING', (0,0), (-1,-1), 5),
('BOTTOMPADDING', (0,0), (-1,-1), 5),
]))
# Layout in 2 columns
two_col = Table(
[[aerd_t, aco_t],
[SP(0.25), SP(0.25)],
[preg_t, eib_t]],
colWidths=[col_w, col_w]
)
two_col.setStyle(TableStyle([
('LEFTPADDING', (0,0), (-1,-1), 0),
('RIGHTPADDING', (0,0), (-1,-1), 0),
('TOPPADDING', (0,0), (-1,-1), 0),
('BOTTOMPADDING', (0,0), (-1,-1), 0),
('INNERGRID', (0,0), (-1,-1), 0, WHITE),
('BOX', (0,0), (-1,-1), 0, WHITE),
('COLPADDING', (0,0), (-1,-1), 5),
]))
story.append(two_col)
story.append(SP(0.4))
# ── COMORBIDITIES TABLE ──
story.append(p('KEY COMORBIDITIES AFFECTING ASTHMA CONTROL', H2))
story.append(HR(ORANGE, 1.5, 2, 5))
comor_headers = ['Comorbidity', 'Impact on Asthma', 'Management']
comor_rows = [
['Rhinosinusitis / Nasal polyps',
'Worsens AHR via inflammatory mediators, post-nasal drip, neural reflexes',
'Intranasal steroids (reduce AHR + ED visits); biologics for polyps (dupilumab, tezepelumab)'],
['GERD',
'Independent predictor of exacerbations; microaspiration + vagal reflexes',
'Treat symptomatic GERD (PPI ± lifestyle); asymptomatic GERD treatment NOT beneficial'],
['Obesity',
'2–4× hospitalisation risk; non-eosinophilic pattern; mechanical restriction + adipokines',
'Weight loss (bariatric surgery reduces exacerbations); non-T2 management; LAMA add-on'],
['OSA',
'Increased exacerbation severity; AHI correlates with exacerbations; OCS worsens OSA',
'CPAP → improves QoL, reduces exacerbations, reduces bronchodilator use'],
['Anxiety / Depression',
'Increased exacerbation rates; may not distinguish anxiety from asthma',
'Psychological support; distinguish from VCD; optimise asthma control'],
['Vocal cord dysfunction (ILO)',
'Can mimic OR coexist with asthma; inspiratory stridor; commoner in women',
'Laryngoscopy during symptoms; speech therapy; treat anxiety; NOT responsive to bronchodilators'],
]
story.append(make_table(comor_headers, comor_rows,
[4.0*cm, 5.5*cm, W-9.5*cm], header_bg=ORANGE))
story.append(PageBreak())
# ══════════════════════════════════════════════════════════════════
# PAGE 6 – DRUG MECHANISMS & QUICK REFERENCE
# ══════════════════════════════════════════════════════════════════
story.append(SP(0.2))
story.append(section_header('6. DRUG MECHANISMS & QUICK REFERENCE', MED_BLUE))
story.append(SP(0.3))
# Drug mechanism table
story.append(p('MECHANISM OF ACTION – KEY DRUG CLASSES', H2))
story.append(HR(MED_BLUE, 1.5, 2, 5))
drug_headers = ['Drug Class', 'Mechanism', 'Key Points']
drug_rows = [
[p('<b>SABA\n</b>Salbutamol,\nLevalbuterol', TC_B),
'β₂ receptor → Gs → ↑cAMP → PKA → MLCK inhibition\n+ opens K⁺ channels → hyperpolarisation → SM relaxation',
'⚠ NEVER use as monotherapy (increased mortality). '
'Onset 3–5 min. Duration 4–6h. Side effects: tremor, tachycardia, hypokalaemia, Type B lactic acidosis.'],
[p('<b>LABA\n</b>Formoterol (rapid)\nSalmeterol (slow)', TC_B),
'Same as SABA. Formoterol = moderate lipophilicity (rapid + sustained).\nSalmeterol = anchored in exosite (slow onset)',
'Duration ~12h. FORMOTEROL can be reliever (rapid onset). SALMETEROL cannot. '
'NEVER use as monotherapy in asthma.'],
[p('<b>ICS\n</b>Budesonide,\nFluticasone,\nCiclesonide', TC_B),
'Binds GR → nuclear translocation → trans-repression of NF-κB/AP-1\n→ ↓IL-4, IL-5, IL-13, TNF-α, iNOS',
'Oral bioavailability: Beclomethasone 20%; Budesonide 10–15%; Fluticasone ~1%; Mometasone <1%; '
'Ciclesonide = pro-drug (activated in lung). Reduces FeNO + eosinophils + AHR. '
'Side effects: growth suppression (children), osteoporosis, cataracts.'],
[p('<b>LAMA\n</b>Tiotropium,\nUmeclidinium', TC_B),
'M₃ receptor blockade → ↓ACh-induced smooth muscle contraction;\nfunctional selectivity M₃/M₁ > M₂',
'Add-on Step 4–5. Note: blocking M₂ (autoinhibitory) would → ↑ACh release – '
'LAMAs have favourable kinetics avoiding this. Side effects: dry mouth, urinary retention, glaucoma (high dose).'],
[p('<b>LTRA\n</b>Montelukast,\nZafirlukast', TC_B),
'CysLT₁ receptor antagonism → blocks LTC₄/LTD₄/LTE₄\n→ ↓bronchoconstriction, ↓mucus, ↓eosinophil recruitment',
'⚠ FDA BLACK BOX: Montelukast → serious neuropsychiatric effects (suicidal ideation, depression). '
'Alternative Step 2. Good for AERD and EIB. Reduces BOTH early and late phase response.'],
[p('<b>IV Mg²⁺\n</b>Sulphate', TC_B),
'Competes with Ca²⁺ → inhibits smooth muscle contraction;\nantagonises Ca²⁺-dependent mediator release from mast cells',
'2g IV over 20 min. Single dose. For severe/life-threatening acute asthma. '
'Reduces hospitalisation rate and intubation need. Safe; mild hypotension risk.'],
[p('<b>Theophylline', TC_B),
'Inhibits phosphodiesterase → ↑cAMP + ↑cGMP\nAlso: adenosine receptor antagonism; restores HDAC2 activity (low dose)',
'Now RARELY used for asthma. Narrow therapeutic window. '
'Interactions: erythromycin, ciprofloxacin, rifampicin. '
'Low-dose theophylline may partially reverse steroid resistance via HDAC2.'],
]
story.append(make_table(drug_headers, drug_rows,
[2.8*cm, 5.0*cm, W-7.8*cm]))
story.append(SP(0.4))
# ICS potency/bioavailability comparison
story.append(p('ICS COMPARISON – ORAL BIOAVAILABILITY & PROPERTIES', H2))
story.append(HR(MED_BLUE, 1.5, 2, 5))
ics_headers = ['ICS Agent', 'Oral Bioavail.', 'Half-life', 'Special Feature', 'Pregnancy']
ics_rows = [
['Beclomethasone dipropionate', '~20%', '0.5h (BDP) → 17-BMP active', 'Oldest; oropharyngeal deposition issue; pMDI fine particle', 'B'],
['Budesonide', '~10–15%', '2–3h', 'Both pMDI and DPI; reference standard ICS', '★ Safe'],
['Fluticasone propionate', '~1%', '14h', 'High topical potency; commonly combined with salmeterol/vilanterol', 'B'],
['Fluticasone furoate', 'Negligible', '24h', 'Once-daily; only with vilanterol (ultra-LABA)', 'B'],
['Mometasone furoate', '<1%', '5h', 'Very low oral BA; combined with formoterol/indacaterol', 'C'],
['Ciclesonide', '<1%', '0.7h (parent) 45h (active)', 'Pro-drug activated in lung by esterases; NO oropharyngeal deposition', 'C'],
]
story.append(make_table(ics_headers, ics_rows,
[3.8*cm, 2.5*cm, 3.2*cm, 5.0*cm, 1.8*cm]))
story.append(SP(0.3))
# Quick reference summary box
story.append(info_box(
'📋 QUICK CLINICAL REFERENCE SUMMARY',
[
p('<b>T2 biomarkers positive (FeNO ≥40, eos ≥300, IgE elevated) + severe:</b> Step up to biologic. '
'Choose based on dominant comorbidity (atopic → omalizumab/dupilumab; eosinophilic → anti-IL-5; '
'no biomarker dominance → tezepelumab).', BODY),
p('<b>Normal PaCO₂ in a distressed asthmatic = DANGER:</b> Impending respiratory failure. '
'Do not be falsely reassured. Prepare for intubation.', WARN),
p('<b>ICS/formoterol (AIR) is now preferred at ALL steps</b> per GINA 2026 – not just steps 3–4.', BODY),
p('<b>Before stepping up:</b> Always check adherence (responsible for ≥50% of "refractory" cases), '
'inhaler technique, triggers, and comorbidities first.', BODY),
p('<b>Permissive hypercapnia</b> during MV in status asthmaticus: accept PaCO₂ rising; '
'target pH ≥7.2; use NaHCO₃ if pH <7.2; ketamine for induction.', BODY),
p('<b>Montelukast:</b> FDA black box warning for neuropsychiatric effects – inform patients before prescribing.', WARN),
p('<b>Depemokimab (GINA 2026):</b> Newest anti-IL-5 biologic; SC every 6 months; '
'longest dosing interval of any approved biologic for asthma.', BODY),
], LIGHT_BLUE, MED_BLUE))
story.append(SP(0.4))
# Sources
story.append(HR(GREY_MED, 0.5, 4, 4))
story.append(p('<b>Sources:</b> GINA Global Strategy for Asthma Management and Prevention 2026 (released May 5, 2026); '
'Harrison\'s Principles of Internal Medicine 22E (2025), Chapter 298; '
'Goodman & Gilman\'s Pharmacological Basis of Therapeutics, Chapter 44; '
'Fishman\'s Pulmonary Diseases and Disorders; '
'Murray & Nadel\'s Textbook of Respiratory Medicine; '
'Systematic Reviews: PMID 40520782 (biologics umbrella review, 2025).', NOTE))
story.append(p('Prepared for Respiratory Medicine PGT educational use. '
'Not a substitute for clinical judgment. All treatment decisions should be guided by '
'local guidelines, specialist review, and individual patient assessment.', NOTE))
return story
# ─────────────────────────── MAIN ─────────────────────────────────────
def main():
doc = make_doc()
story = build_story()
# Build with page templates
doc.build(
story,
onFirstPage=build_cover,
onLaterPages=build_page_header_footer,
)
print(f'✅ PDF created: {OUTPUT}')
if __name__ == '__main__':
main()
cd /home/daytona/workspace/asthma-pdf && python3 generate_asthma_pdf.py 2>&1
~/asthma-pdf/generate_asthma_pdf.py
Successfully replaced 1 instance(s) of the string in '/home/daytona/workspace/asthma-pdf/generate_asthma_pdf.py'
cd /home/daytona/workspace/asthma-pdf && python3 generate_asthma_pdf.py 2>&1
~/asthma-pdf/generate_asthma_pdf.py
Successfully replaced 1 instance(s) of the string in '/home/daytona/workspace/asthma-pdf/generate_asthma_pdf.py'
cd /home/daytona/workspace/asthma-pdf && python3 generate_asthma_pdf.py 2>&1
ls -lh /home/daytona/workspace/asthma-pdf/Asthma_Management_Reference.pdf
Asthma Management Reference
PDF Document · PDF
What's inside (6 pages, colour-coded)
| Page | Content |
|---|---|
| Cover | Title page with 4 topic tiles (GINA 2026, Biologics, Acute Asthma, Biomarkers) |
| Page 1 | Definition, epidemiology key facts, diagnostic criteria table, biomarker interpretation table (FeNO / Blood Eos / IgE / Sputum Eos / Periostin) |
| Page 2 | GINA 2026 5-step algorithm (colour-coded Steps 1–5), AIR paradigm box, stepping up/down rules, OCS minimisation guidance |
| Page 3 | T2 inflammatory cascade diagram, all 8 biologics comparison table (targets, routes, thresholds, notes), biologic selection algorithm by phenotype |
| Page 4 | ABG evolution in acute asthma (colour-coded stages), severity grading table, GINA 2026 acute management protocol, ATS/IDSA severe CAP criteria |
| Pages 5–6 | GINA 2026 fatality risk indicators, special scenarios (AERD, ACO, pregnancy, EIB) in 2-column layout, comorbidities table, drug mechanism table, ICS comparison table, quick clinical reference summary box |
Tell me about copd in detail for final exam
"COPD" AND "GOLD guidelines" AND "management"
GOLD 2025 2026 COPD guidelines update management classification
https://pmc.ncbi.nlm.nih.gov/articles/PMC13109179
"COPD" AND "exacerbation" AND "treatment"
COPD - Comprehensive Final Exam Guide
Based on GOLD 2026 | Harrison's 22E | Fishman's Pulmonary | Robbins Pathology | Katzung Pharmacology
1. DEFINITION
2. EPIDEMIOLOGY
| Parameter | Value |
|---|---|
| Global prevalence | ~391 million people; ~10% of adults |
| Global mortality | 3rd leading cause of death worldwide |
| US deaths | ~150,000/year |
| Economic cost | >$40 billion/year in the US alone |
| Smoker risk | Previously cited as 15-30% of smokers; now higher with CT data showing subclinical disease in many more |
3. ETIOLOGY & RISK FACTORS
Major Risk Factors
- Cigarette smoking (by far the most important): dose-dependent; pack-years correlate with severity
- Biomass fuel exposure (cooking smoke - major cause in low-income countries, especially women)
- Occupational exposures: coal dust, silica, grain dust, cadmium
- Air pollution (indoor + outdoor)
- Recurrent respiratory infections in childhood
- Low birth weight / impaired lung development
- Alpha-1 antitrypsin (A1AT) deficiency - genetic cause
Alpha-1 Antitrypsin Deficiency (Important Exam Topic)
- Autosomal co-dominant inheritance
- PiZZ phenotype = severe deficiency; PiMZ = intermediate
- A1AT is a serine protease inhibitor that neutralises neutrophil elastase
- Deficiency → unopposed elastase activity → panacinar emphysema (lower lobe predominant)
- Also causes liver cirrhosis (misfolded protein accumulates in hepatocytes)
- ATS recommends testing all patients with persistent airflow obstruction for A1AT levels
- Treatment: intravenous A1AT augmentation therapy (weekly IV infusions)
4. PATHOLOGY
4a. Emphysema Types
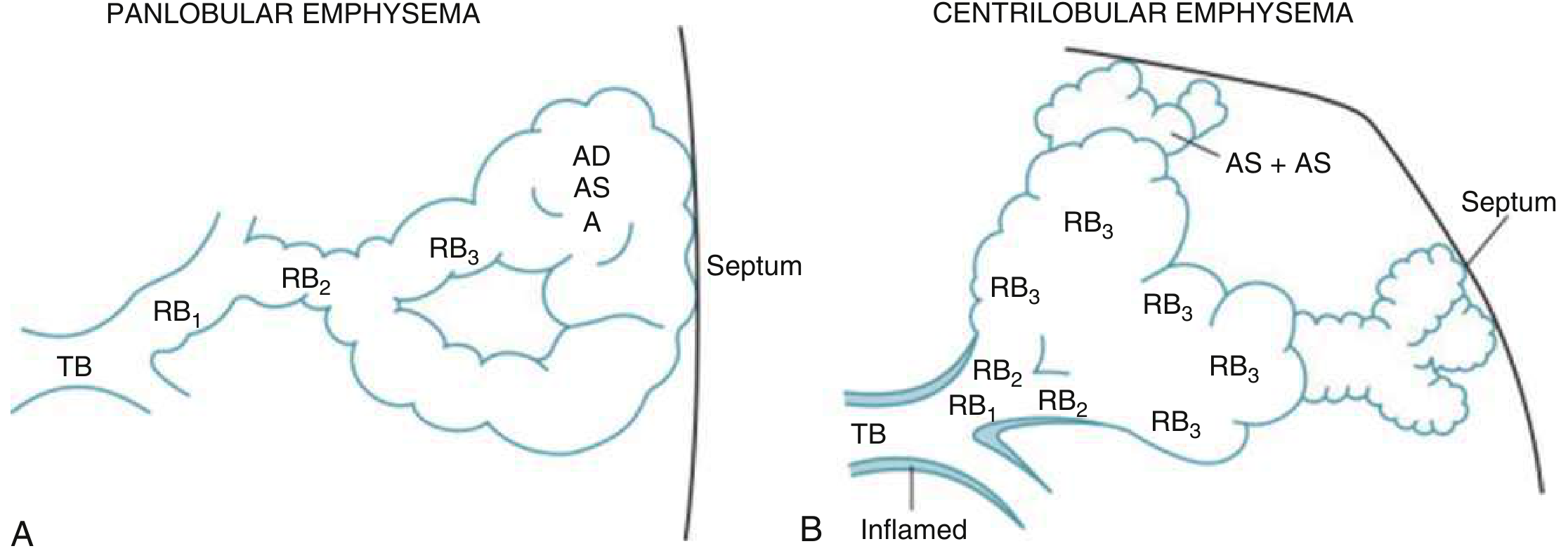
| Type | Anatomy | Cause | Distribution |
|---|---|---|---|
| Centriacinar (Centrilobular) | Enlargement of proximal respiratory bronchioles (RB1-3); alveolar sacs preserved | Cigarette smoking | Upper lobe predominant |
| Panacinar (Panlobular) | Uniform destruction of entire acinus from TB to alveolar sacs | A1AT deficiency | Lower lobe predominant |
| Paraseptal | Distal acinus; subpleural; near septa | Often idiopathic | Upper lobe; causes spontaneous pneumothorax |
| Irregular (Scar) | Around areas of fibrosis/scarring | Post-inflammatory | Adjacent to scars |
4b. Chronic Bronchitis Pathology
- Clinical definition: Productive cough for ≥3 months in ≥2 consecutive years (no other cause)
- Pathological changes:
- Reid index >0.4 (gland thickness / bronchial wall thickness; normal <0.4)
- Hyperplasia of submucosal mucous glands (Reid index)
- Goblet cell metaplasia in small airways
- Inflammatory infiltrate (predominantly neutrophilic)
- Bronchiolar wall fibrosis
- Ciliary dysfunction → impaired mucociliary clearance
- MUC5AC concentration increased 10-fold, MUC5B 3-fold in severe COPD (Fishman's)
5. PATHOPHYSIOLOGY
5a. Protease-Antiprotease Imbalance
- Trigger: Cigarette smoke / noxious particles → oxidative stress → recruit neutrophils and macrophages
- Neutrophils release elastase (matrix metalloproteinases + serine proteases)
- A1AT (produced by liver) normally inhibits neutrophil elastase
- Oxidative stress from cigarette smoke inactivates A1AT
- Net result: Unopposed elastase destroys elastin and type IV collagen in alveolar walls → enlarged airspaces → emphysema
- Loss of elastic recoil → airway collapse on expiration → airflow obstruction
5b. Inflammation Profile
- Dominant cell: Neutrophil (unlike asthma which is eosinophilic)
- Also: CD8+ T-cells, macrophages, mast cells in some patients
- Inflammatory mediators: IL-8, TNF-α, LTB₄, MMP-9, MMP-12
- ICS are poorly effective because neutrophilic inflammation is corticosteroid-resistant
5c. Small Airway Disease
- Earliest change: Inflammation and fibrosis of small airways (<2mm diameter)
- Small airways account for only 25% of total airway resistance normally, but become major site of obstruction in COPD
- Small airway obstruction precedes detectable spirometric changes
- CT can detect small airway mucus plugging even with preserved FEV₁
5d. Dynamic Hyperinflation (Important Exam Mechanism)
- Loss of elastic recoil → static hyperinflation (increased FRC at rest)
- During exercise: increased ventilatory demand + insufficient expiratory time → air trapping → dynamic hyperinflation
- End-expiratory lung volume (EELV) rises → inspiratory reserve volume (IRV) falls critically
- Creates neuromechanical uncoupling (effort disproportionate to VT response) → sensation of dyspnoea
- Barrel chest = compensatory increase in AP diameter due to chronically elevated FRC
- Flattened diaphragm on CXR/CT due to hyperinflation
5e. Gas Exchange Abnormalities
- V/Q mismatch is the primary mechanism of hypoxaemia in COPD
- Perfused but poorly ventilated alveoli (low V/Q) → venous admixture → ↓PaO₂
- Unlike asthma, A-a gradient is elevated (measured PaO₂ << calculated PAO₂)
- Alveolar gas equation: PAO₂ = PiO₂ - PaCO₂/R = 150 - PaCO₂/0.8
- Early COPD: Hypoxaemia + hypocapnia (hyperventilation compensates)
- Late COPD (type B "blue bloater"): Hypoxaemia + hypercapnia + respiratory acidosis
- Emphysema patients tend to maintain normocarbia longer ("pink puffer")
5f. Pink Puffer vs Blue Bloater (Classic Teaching)
| Feature | Pink Puffer (Emphysema type) | Blue Bloater (Bronchitic type) |
|---|---|---|
| Dominant pathology | Emphysema | Chronic bronchitis |
| Body habitus | Thin, cachexic | Overweight |
| Cyanosis | Absent (pink) | Present (blue) |
| SpO₂ | Relatively preserved | Low |
| PaCO₂ | Normal/low (hyperventilates) | Elevated (hypercapnic) |
| Cor pulmonale | Late | Earlier |
| Pursed-lip breathing | Yes | No |
| Note: In clinical reality, most patients are mixed |
6. CLINICAL FEATURES
Symptoms (Classic Triad)
- Dyspnoea - progressive, worse on exertion; described as "breathlessness" or "air hunger"; MRC scale used
- Chronic cough - may be intermittent; productive or dry
- Sputum production - chronic bronchitis phenotype; purulent during exacerbations
Signs
| Sign | Mechanism |
|---|---|
| Barrel chest (↑ AP diameter) | Static hyperinflation |
| Pursed-lip breathing | Self-PEEP to prevent dynamic airway collapse |
| Accessory muscle use (SCM, scalenes) | Increased WOB; hyperinflation flattens diaphragm |
| Hoover sign | Paradoxical inward movement of lower ribs on inspiration |
| Reduced breath sounds | Airway obstruction + hyperinflation |
| Wheeze | Airway narrowing |
| Prolonged expiratory phase | Increased airway resistance |
| Cyanosis | Hypoxaemia (type B phenotype) |
| Ankle oedema + JVP elevation | Cor pulmonale (right heart failure) |
| Tripod positioning | Fixes shoulder girdle to use accessory muscles |
7. INVESTIGATIONS
Spirometry (Mandatory for Diagnosis)
| GOLD Grade | Post-BD FEV₁/FVC | FEV₁ (% predicted) |
|---|---|---|
| Diagnosis | < 0.70 | Any |
| GOLD 1 (Mild) | < 0.70 | ≥ 80% |
| GOLD 2 (Moderate) | < 0.70 | 50–79% |
| GOLD 3 (Severe) | < 0.70 | 30–49% |
| GOLD 4 (Very Severe) | < 0.70 | < 30% |
Chest X-Ray (CXR) Findings
- Hyperinflation: >6 anterior ribs visible; flat hemidiaphragms (below rib 6 anteriorly)
- Increased AP diameter on lateral view
- Hyperlucent lung fields (reduced vascular markings)
- Bullae formation
- Increased retrosternal airspace on lateral CXR
HRCT Thorax
- Low-attenuation areas = emphysema (quantified as % of lung below -950 HU threshold)
- Air trapping on expiratory CT
- Small airway mucus plugging
- Airway wall thickening (chronic bronchitis)
- Bronchiectasis (15-30% of COPD patients have concomitant bronchiectasis)
Blood Tests
- FBC: Polycythaemia (chronic hypoxia → ↑EPO → ↑RBC)
- ABG: Hypoxaemia ± hypercapnia; pH; HCO₃⁻ (chronic compensation)
- A1AT level: Test all patients with airflow obstruction (ATS recommendation)
- Blood eosinophil count (BEC): Critical biomarker for treatment decisions (ICS, dupilumab)
- BNP/NT-proBNP: Elevated in cor pulmonale / right heart failure
ECG
- P pulmonale (peaked P waves >2.5mm in II, III, aVF)
- Right axis deviation
- Right ventricular hypertrophy pattern
- Low voltage (hyperinflation)
8. GOLD ABE CLASSIFICATION (GOLD 2026 Update)
Assessment Dimensions
- Spirometry (GOLD grade 1-4) - for severity of airflow obstruction
- Symptoms - assessed with mMRC ≥2 or CAT ≥10
- Exacerbation history - key determinant of treatment
Groups A, B, E
| Group | Exacerbation History | Symptoms | Initial Therapy |
|---|---|---|---|
| A | 0 exacerbations in past year | mMRC 0–1 / CAT <10 | Short- or long-acting bronchodilator (LAMA preferred if available) |
| B | 0 exacerbations in past year | mMRC ≥2 / CAT ≥10 | LABA + LAMA (dual bronchodilation) |
| E ("Exacerbator") | ≥1 moderate exacerbation (NEW GOLD 2026) or ≥2 moderate or ≥1 severe | Any symptom level | LABA + LAMA ± ICS (based on blood eosinophils) |
9. PHARMACOLOGICAL MANAGEMENT
9a. Bronchodilators (Mainstay)
- Tiotropium (Spiriva), umeclidinium, glycopyrronium, aclidinium
- Mechanism: M₃ receptor blockade → ↓ACh-mediated bronchoconstriction; also reduce mucus secretion
- Once daily (tiotropium, umeclidinium) or twice daily
- Preferred initial bronchodilator in COPD (outperform LABAs on lung function + exacerbations in most head-to-head trials)
- Salmeterol, formoterol, indacaterol, olodaterol, vilanterol
- Duration 12h (salmeterol, formoterol) or 24h (indacaterol, vilanterol, olodaterol)
- Preferred for Group B and most Group E patients
- Greater bronchodilation + exacerbation reduction vs. monotherapy
- Examples: umeclidinium/vilanterol (Anoro), tiotropium/olodaterol (Spiolto), glycopyrronium/indacaterol (Ultibro)
- Salbutamol (SABA), ipratropium (SAMA)
- For rescue/PRN use
- Combined SABA+SAMA (combivent) for acute use
9b. Inhaled Corticosteroids (ICS) - Conditional Use
| Blood Eosinophil Count | ICS Recommendation |
|---|---|
| ≥300 cells/µL | ICS likely beneficial; add to LABA/LAMA |
| 100–299 cells/µL | Consider ICS; weigh benefits vs risks |
| <100 cells/µL | ICS unlikely to benefit; associated with ↑ pneumonia risk |
- Persistent exacerbations despite LABA+LAMA
- BEC ≥300 cells/µL
- Concurrent asthma-COPD overlap (ACO) - ICS mandatory
- Pneumonia (most important - relative risk ↑ with FP vs budesonide)
- Oral candidiasis
- HPA axis suppression
- Osteoporosis
9c. Triple Therapy (LABA + LAMA + ICS)
- For Group E patients with persistent exacerbations despite LABA+LAMA
- Particularly when BEC ≥100 (more benefit with higher eosinophils)
- GOLD 2026: Triple therapy threshold lowered; more prominently integrated
- Evidence: IMPACT, ETHOS, TRINITY, TRIBUTE trials - all show class effect in reducing exacerbations and improving FEV₁
- Budesonide/formoterol/glycopyrronium (Breztri Aerosphere)
- Fluticasone furoate/umeclidinium/vilanterol (Trelegy Ellipta)
9d. Roflumilast (PDE4 Inhibitor)
- Selective phosphodiesterase-4 inhibitor → ↑cAMP → anti-inflammatory
- Indication: GOLD 3-4 + chronic bronchitis phenotype + frequent exacerbations despite maximal ICS/LABA/LAMA
- Reduces exacerbations by ~15-17%
- Side effects: Nausea, diarrhoea, weight loss, psychiatric effects - limit use
- Note: Not a bronchodilator - purely anti-inflammatory
9e. Azithromycin (Long-term antibiotic)
- 250mg/day or 500mg 3×/week
- Reduces exacerbation frequency by ~27% in selected patients
- Mechanism: Anti-inflammatory + anti-bacterial (against H. influenzae, non-typeable H. influenzae)
- Concerns: Hearing loss, cardiac arrhythmias (QTc prolongation), antibiotic resistance
- Indication: Former/non-smokers, frequent exacerbators, elderly
9f. Mucolytics
- N-acetylcysteine (NAC), carbocisteine, erdosteine
- Reduce viscosity of mucus; some antioxidant effect
- Recent systematic review (PMID: 39413571, 2024): modest benefit on exacerbation reduction in stable COPD
- Indicated especially in chronic bronchitis phenotype
9g. Biologics (GOLD 2026 - New Integration)
- BOREAS and NOTUS trials
- Indication: COPD + chronic bronchitis phenotype + BEC ≥300 cells/µL + uncontrolled on triple therapy
- Reduces moderate-severe exacerbations by 30-34% + improves FEV₁
- Only biologic currently with strong evidence base for COPD
- GOLD 2026 positions this as an additional option after triple therapy failure in eosinophilic COPD
- PMID: 40626315 (2025 network meta-analysis) supports type-2 biologics in COPD
- Evidence emerging but not yet as strong as dupilumab
10. NON-PHARMACOLOGICAL MANAGEMENT
Smoking Cessation
- Single most effective intervention to slow FEV₁ decline
- Fletcher-Peto curves: accelerated FEV₁ decline in susceptible smokers; stops with cessation
- Methods: Nicotine replacement therapy (NRT), varenicline (preferred: 2× more effective), bupropion, behavioural support
- Even after decades of smoking - cessation slows progression
Pulmonary Rehabilitation (PR)
- Strongest evidence for improving dyspnoea, exercise capacity, and QoL
- Does NOT improve FEV₁ or mortality significantly in isolation
- Components: Aerobic exercise, strength training, education, nutritional support, psychosocial support
- Duration: 6-8 weeks (minimum); 12 weeks preferred
- Must be initiated within 4 weeks after exacerbation (post-exacerbation PR reduces readmissions)
Long-Term Oxygen Therapy (LTOT)
- PaO₂ ≤55 mmHg (7.3 kPa) at rest on room air
- PaO₂ 56-59 mmHg (7.3-8.0 kPa) PLUS one of: cor pulmonale, polycythaemia (Hct >55%), pulmonary hypertension
Vaccination (GOLD 2026 - Core Disease-Modifying Strategy)
| Vaccine | Recommendation |
|---|---|
| Influenza | Annual; all COPD patients |
| Pneumococcal (PCV13/PCV20 + PPSV23) | All COPD patients |
| COVID-19 | All COPD patients |
| RSV (RSVpreF / RSVmAb) | ≥60 years with COPD |
| Tdap/Td | If not previously vaccinated |
Lung Volume Reduction Surgery (LVRS)
- Removes most diseased portions of lung (typically upper lobes)
- Improves elastic recoil, reduces hyperinflation, improves diaphragm mechanics
- Best candidates: Upper-lobe predominant emphysema + low exercise capacity after PR
- NETT trial: Mortality benefit in upper-lobe COPD with low post-PR exercise
Bronchoscopic Lung Volume Reduction (BLVR)
- Endobronchial valves (Zephyr, Spiration): one-way valves → lobar atelectasis → reduce hyperinflation
- Coils, thermal vapour ablation - alternative modalities
- Requires absence of collateral ventilation (Chartis assessment or fissure completeness on CT)
Lung Transplantation
- End-stage COPD (GOLD 4) failing maximal therapy
- Single or bilateral lung transplant
- BODE index used for listing prioritisation (BMI, Obstruction, Dyspnoea, Exercise)
11. EXACERBATIONS OF COPD (AECOPD)
Definition
Triggers
- Viral infections: 50-80% (rhinovirus, influenza, parainfluenza, RSV, coronavirus)
- Bacterial infections: 40-60% H. influenzae (most common), Streptococcus pneumoniae, Moraxella catarrhalis, Pseudomonas (severe COPD)
- Air pollution
- Pulmonary embolism (frequently overlooked - check D-dimer/CTPA)
Severity Classification (GOLD 2026 Revised)
| Severity | Definition | Setting |
|---|---|---|
| Mild | Managed by patient alone; increased SABA only | Home |
| Moderate | Requires medical intervention; antibiotics ± steroids | Outpatient |
| Severe | Requires hospitalisation; life-threatening | Inpatient / ICU |
Management of Acute Exacerbation
- Increase dose/frequency of SABAs (salbutamol 2.5-5mg neb q20min)
- Add ipratropium 0.5mg neb
- Continue LABAs and LAMAs
- Prednisolone 30-40mg/day for 5 days (REDUCE trial: 5 days = 14 days; no benefit to longer)
- Reduces exacerbation duration and hospital stay
- Indicated if: purulent sputum AND increased dyspnoea AND increased sputum volume (Anthonisen criteria - 2 or 3 = antibiotics)
- Or if mechanically ventilated
- Choice: Amoxicillin/clavulanate, doxycycline, or azithromycin
- Pseudomonas coverage if: severe COPD (FEV₁ <30%), hospitalised, prior Pseudomonas infection, immunocompromised → ciprofloxacin or anti-pseudomonal beta-lactam
- Target SpO₂ 88-92% (controlled oxygen; avoid hyperoxia)
- High-flow O₂ → ↑ PaCO₂ (Haldane effect + absorption atelectasis + ↓hypoxic drive) → hypercapnic respiratory failure
- Indication: pH <7.35 + PaCO₂ >45 mmHg (type 2 respiratory failure)
- Reduces need for intubation by ~58%, reduces mortality ~48%
- IPAP 12-20 cmH₂O, EPAP 4-8 cmH₂O, FiO₂ titrated
- Contraindications: Vomiting, unable to protect airway, facial trauma, haemodynamic instability
- GOLD 2026 now includes HFNC as a modality in exacerbation management
- Better tolerated than NIV; useful in milder type 2 failure or NIV intolerance
- Failure of NIV, pH <7.25, haemodynamic instability
- Strategy: Low RR + longer expiratory time (I:E 1:3) to avoid auto-PEEP; permissive hypercapnia
12. COMPLICATIONS
| Complication | Mechanism |
|---|---|
| Cor pulmonale | Chronic hypoxia → hypoxic vasoconstriction → pulmonary hypertension → RV hypertrophy/failure |
| Polycythaemia | Chronic hypoxia → ↑EPO → ↑RBC mass |
| Spontaneous pneumothorax | Rupture of paraseptal bullae (especially young male with upper-lobe paraseptal emphysema) |
| Respiratory failure (Type 1 and 2) | Progressive V/Q mismatch; later hypoventilation |
| Pulmonary hypertension | Leads to CXR: prominent hila, right heart enlargement |
| Malnutrition/cachexia | Increased WOB + systemic inflammation (TNF-α) |
| Muscle wasting | Systemic inflammation + deconditioning |
| Depression/anxiety | ~40% prevalence; worsens outcomes |
| Lung cancer | 5-6× increased risk; smoking + inflammation + air trapping |
| Atrial fibrillation | Common comorbidity; hypoxia, catecholamines, RV strain |
13. PROGNOSTIC INDICES
BODE Index (Best validated prognostic tool)
| Variable | Score 0 | Score 1 | Score 2 | Score 3 |
|---|---|---|---|---|
| BMI | >21 | ≤21 | - | - |
| Obstruction (FEV₁%) | ≥65% | 50-64% | 36-49% | ≤35% |
| Dyspnoea (mMRC) | 0-1 | 2 | 3 | 4 |
| Exercise (6MWT, m) | ≥350 | 250-349 | 150-249 | ≤149 |
Other Predictors
- Exacerbation frequency (each exacerbation accelerates FEV₁ decline)
- 6-minute walk distance (6MWT) - most prognostically powerful single test
- FEV₁ decline rate (>50 mL/year = accelerated)
- CT emphysema quantification
14. ASTHMA-COPD OVERLAP (ACO)
- Features of both asthma and COPD: variable obstruction + incomplete reversibility
- Spirometry: Post-BD FEV₁/FVC <0.70 + some reversibility (FEV₁ ↑ ≥12% AND ≥200 mL)
- Often: atopic history, blood eosinophilia, elevated FeNO, smoking history
- Critical rule: ICS is MANDATORY in ACO (unlike pure COPD where it is conditional)
- LABA + LAMA can both be used
- ⚠ LABA monotherapy (without ICS) is contraindicated in ACO
15. KEY HIGH-YIELD EXAM POINTS
| Topic | High-Yield Fact |
|---|---|
| Diagnostic criterion | Post-BD FEV₁/FVC <0.70 (GOLD); not reversible to normal |
| Most common cause | Cigarette smoking |
| Genetic cause | A1AT deficiency → panacinar emphysema, lower lobes |
| Centriacinar emphysema | Smoking; upper lobes; most common type |
| Reid index | >0.4 in chronic bronchitis (gland/wall thickness) |
| Pink puffer vs blue bloater | Emphysema vs bronchitis phenotype |
| ABG in COPD exacerbation | pH ↓, PaCO₂ ↑, PaO₂ ↓ (type 2 RF) |
| O₂ target in COPD | 88-92% SpO₂ (NOT 95-98% - risk of hypercapnia) |
| Hypercapnia mechanism | V/Q mismatch + Haldane effect with high-flow O₂ |
| ICS in COPD | Only if BEC ≥300 OR persistent exacerbations; NOT first-line |
| ICS risk unique to COPD | Increased pneumonia risk |
| LABA monotherapy | CONTRAINDICATED in asthma; acceptable in COPD |
| GOLD 2026 Group E threshold | Lowered - now includes single moderate exacerbation |
| Triple therapy trials | IMPACT, ETHOS, TRINITY, TRIBUTE |
| LTOT indication | PaO₂ ≤55 mmHg OR 56-59 with cor pulmonale/polycythaemia |
| LTOT duration | ≥15 hours/day |
| Steroid course in exacerbation | 5 days prednisolone 30-40mg (REDUCE trial) |
| NIV indication | pH <7.35 + PaCO₂ >45 (type 2 RF) |
| Smoking cessation drug | Varenicline > NRT > bupropion |
| Most effective single intervention | Smoking cessation (slows FEV₁ decline) |
| New GOLD 2026 biologic | Dupilumab - for COPD + chronic bronchitis + BEC ≥300 on triple therapy |
| BODE score | BMI + Obstruction + Dyspnoea + Exercise; 0-10 |
| Roflumilast indication | GOLD 3-4 + chronic bronchitis + frequent exacerbators on maximal therapy |
Tell me about interstitial lung disease
ILD interstitial lung disease 2025 2026 guidelines ATS ERS classification treatment update
"interstitial lung disease" AND "diagnosis" AND "treatment"
Generate a comprehensive ILD reference PDF with classifications, diagnostics, and treatment algorithms
Tell me all about lakshya from gynae and obs.