Teach me pediatrics topics ASD , VSD, PDA - comparison table with etiology, pathogenesis,& hemodynamics, signs and symptoms, investigations, management, complications, Differentials
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
I now have comprehensive data from multiple authoritative textbooks. Let me compile the full detailed comparison table response.
ASD vs VSD vs PDA - Complete Pediatric Comparison
Sources: Robbins & Kumar Pathologic Basis of Disease, Goldman-Cecil Medicine, Sabiston Textbook of Surgery, Schwartz's Principles of Surgery, Creasy & Resnik's Maternal-Fetal Medicine
Hemodynamic Overview Diagram
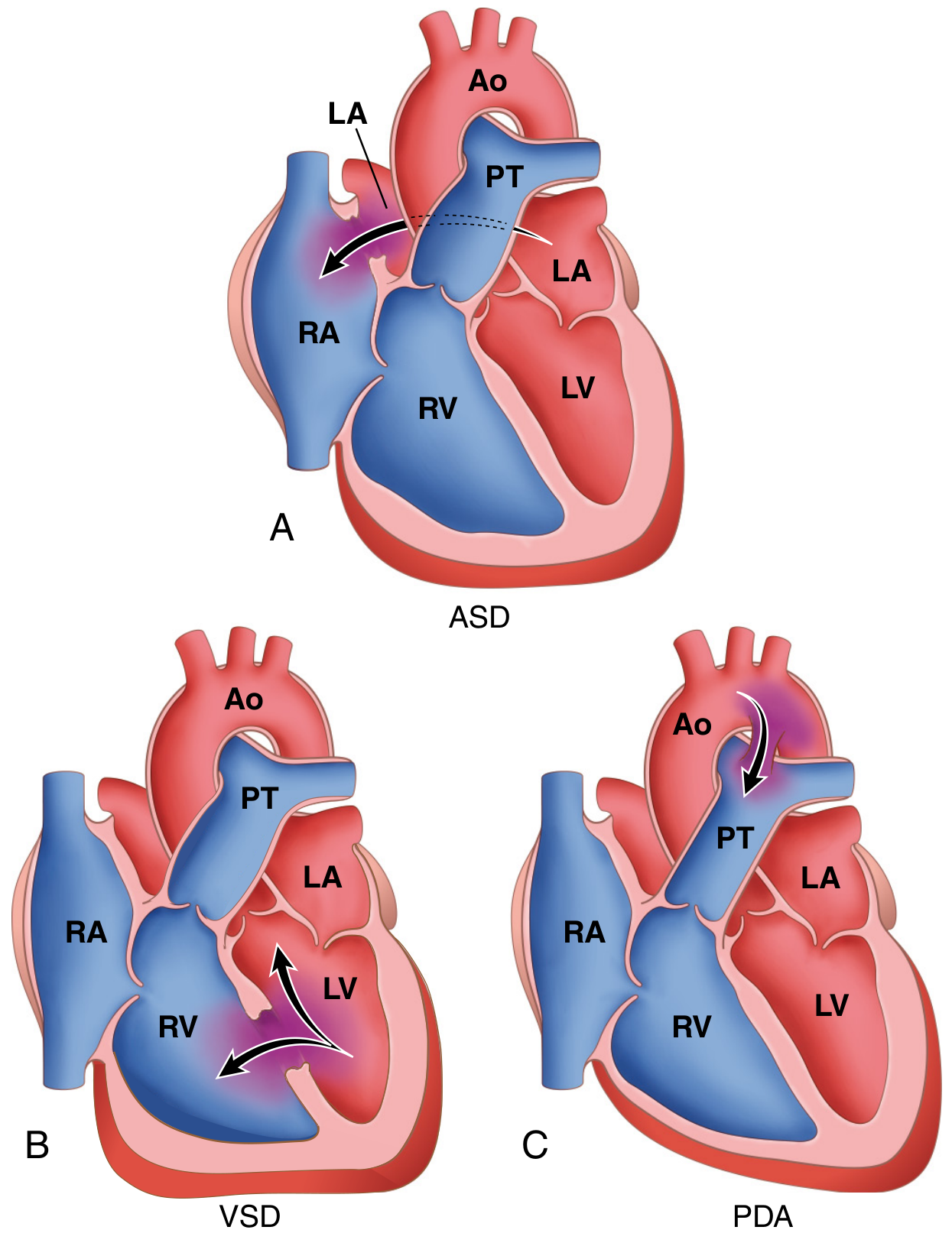
Fig. 12.3 - Robbins, Cotran & Kumar Pathologic Basis of Disease: Common congenital causes of left-to-right shunts
1. ETIOLOGY & CLASSIFICATION
| Feature | ASD | VSD | PDA |
|---|---|---|---|
| Incidence | 13 per 10,000 live births; ~10% of all CHD | Most common CHD - 20-30% of all CHD | ~1 per 2000 births; incidence dramatically increases with prematurity (up to 75% at 28-30 weeks gestation) |
| Sex predilection | Female > Male (2:1) | Equal | Female > Male (2:1) |
| Embryologic basis | Failure of closure of the interatrial septum during development; septum primum/secundum anomaly | Incomplete closure of the interventricular septum | Persistence of the 6th aortic arch derivative connecting pulmonary artery to descending aorta |
| Types / Classification | Secundum (90%) - deficient septum secundum near fossa ovalis; Primum (5%) - near AV valves, often + AV valve defects; Sinus venosus (5%) - near SVC entry, may have anomalous pulmonary venous drainage | Perimembranous / paramembranous (80%) - membranous septum below aortic valve; Muscular (most common by number, multiple possible - "Swiss-cheese"); Inlet/AV canal - below tricuspid valve; Outlet/Supracristal - conal septum below pulmonary valve | Isolated (90%); also seen with complex CHD where duct-dependent circulation may be critical |
| Associated conditions | Down syndrome (primum type); Holt-Oram syndrome; Ellis-van Creveld syndrome | Trisomy 21 (Down), Trisomy 18; Tetralogy of Fallot (component); DiGeorge syndrome; Turner syndrome | Rubella syndrome; prematurity; Trisomy 21; high-altitude birth |
| Genetic/risk factors | Maternal rubella, alcohol, TBX5 mutation (Holt-Oram) | GATA4 mutations; maternal diabetes, alcohol | Prematurity is the biggest risk factor; maternal rubella |
2. PATHOGENESIS & HEMODYNAMICS
| Feature | ASD | VSD | PDA |
|---|---|---|---|
| Shunt direction (initial) | Left atrium → Right atrium (L-to-R) | Left ventricle → Right ventricle (L-to-R) | Aorta → Pulmonary artery (L-to-R) - continuous, both systole and diastole |
| Driving pressure | Left atrial pressure slightly > Right atrial pressure (low pressure difference ~5 mmHg) | LV pressure >> RV pressure during systole (~120 vs 25 mmHg - large gradient) | Aortic systolic AND diastolic pressure > Pulmonary artery pressure (continuous gradient) |
| Primary hemodynamic consequence | Right heart volume overload → RV/RA enlargement; increased pulmonary blood flow | Left heart volume overload → LA and LV dilation; ± pulmonary hypertension depending on size | Left heart volume overload (LA, LV); reduced systemic diastolic pressure due to diastolic runoff |
| Qp:Qs | Can be >3:1 with large defects | >1.5:1 in moderate-severe defects | Depends on duct size; continuous flow in both phases |
| Pulmonary vascular effects | Pulmonary hypertension is uncommon/late in secundum ASD; PVR generally normal | Large defects → pulmonary HTN early in life; irreversible changes possible within first year | Large ducts → pulmonary HTN; Eisenmenger in 5% |
| Eisenmenger development | Rare in secundum ASD; possible with large or primum defects | ~10% of patients with large/unrestrictive VSDs | ~5% of isolated PDAs |
| Special hemodynamic feature | Transient R-to-L shunting with increased intrathoracic pressure (Valsalva, coughing) - paradoxical embolism risk | Small VSDs: negligible; Large VSDs: equal LV-RV pressures; diastolic filling abnormalities in LA | Diastolic shunt lowers aortic diastolic pressure → bounding pulses; "diastolic steal" from coronary/systemic circulation |
| Spontaneous closure | Rare (small secundum may reduce in size) | ~50% of small muscular VSDs; 80% close by 1 month; only 25% still closing by 12 months | Functional closure in 10-15 hours post-term birth; common in premature infants with indomethacin treatment |
3. SIGNS & SYMPTOMS
| Feature | ASD | VSD | PDA |
|---|---|---|---|
| Presentation timing | Often asymptomatic until adulthood (3rd-5th decade); >70% symptomatic by 5th decade | Large defects: symptoms from birth/infancy; small defects: asymptomatic for years | Narrow PDA: asymptomatic; large PDA: failure to thrive, recurrent respiratory infections; premature infants: respiratory distress |
| Key symptoms | Exercise intolerance, dyspnea on exertion, fatigue, palpitations, recurrent respiratory infections in children | Heart failure symptoms: tachypnea, poor feeding, failure to thrive, recurrent respiratory infections, excessive sweating during feeds | Tachypnea, poor feeding, failure to thrive; dyspnea/palpitations in older patients |
| Cyanosis | Absent initially; appears only with Eisenmenger (differential cyanosis NOT typical for ASD) | Absent initially; cyanosis with Eisenmenger reversal | Absent initially; with Eisenmenger: differential cyanosis - lower extremity cyanosis/clubbing more than upper extremity (PA blood flows to descending aorta below left subclavian) |
| Heart sounds | Wide, FIXED splitting of S2 (hallmark - does not vary with respiration); P2 may be loud | Loud P2 if pulmonary hypertension; variable S2 splitting | Normal S2 obscured by murmur; P2 loud with pulmonary HTN |
| Murmur | Soft ejection systolic murmur at 2nd left intercostal space (increased flow across pulmonary valve, NOT across the defect itself); mid-diastolic rumble at lower left sternal border (increased tricuspid flow) if large shunt | Loud, harsh pan-systolic (holosystolic) murmur at left lower sternal border (3rd-4th ICS); thrill often palpable; small "restrictive" VSDs may have louder murmur (maladie de Roger) | Continuous "machinery" murmur at left infraclavicular area / 1st-2nd left ICS (Gibson murmur) - begins after S1, peaks at S2, continues through diastole; louder in left infraclavicular region |
| Pulse character | Normal | Normal or prominent if large shunt | Bounding/waterhammer pulses with wide pulse pressure (diastolic runoff into pulmonary circulation) |
| Precordial findings | Right ventricular heave (parasternal); dilated pulmonary artery palpable at 2nd left ICS | Palpable thrill at left lower sternal border; right ventricular heave if large | Left ventricular heave; bounding peripheral pulses |
| Other signs | Signs of right heart failure in adults | Hepatomegaly, failure to thrive in large VSDs | Tachycardia; hyperactive precordium |
4. INVESTIGATIONS
| Investigation | ASD | VSD | PDA |
|---|---|---|---|
| ECG | Incomplete RBBB (rSr' pattern in V1, V2) - hallmark; Right axis deviation (secundum); Left axis deviation (primum); PR prolongation; atrial fibrillation/flutter in adults | Right ventricular hypertrophy (large defects); left atrial enlargement; left ventricular hypertrophy | Left ventricular hypertrophy; left atrial enlargement in large PDA; normal in small PDA |
| Chest X-ray | Pulmonary plethora (increased vascular markings both lung fields); dilated main PA and branches; RA and RV enlargement; aortic knuckle normal/small | Cardiomegaly; pulmonary plethora; LA and LV enlargement; prominent pulmonary artery | Cardiomegaly; pulmonary plethora; prominent ascending aorta and pulmonary artery; LA/LV enlargement; calcification at duct in older patients |
| Echocardiography | Diagnostic - identifies defect size/location; Doppler quantifies shunt (Qp:Qs) and PA pressures; may miss sinus venosus ASD on TTE → use TEE; bubble study (agitated saline) for PFO | Diagnostic - visualizes defect, quantifies shunt; identifies associated lesions; Doppler for PA pressure estimation | May not directly visualize duct but Doppler signal identifies it; assesses LA/LV size, PA pressure |
| Cardiac catheterization | "Step-up" in O2 saturation at right atrial level; Qp:Qs calculation; pulmonary vascular resistance | "Step-up" in O2 saturation at right ventricular level; Qp:Qs; PA pressure measurement; needed pre-operatively for older patients | "Step-up" at PA level; Qp:Qs ratio; catheterization for pulmonary vascular resistance assessment before closure in borderline cases |
| Special tests | TEE for sinus venosus or ambiguous TTE; cardiac MRI for complex anatomy | Cardiac MRI for complex VSDs; TEE intraoperatively | Cardiac catheterization if Eisenmenger suspected; CT angiography |
5. MANAGEMENT
| Aspect | ASD | VSD | PDA |
|---|---|---|---|
| Medical (conservative) | Observation for small defects; manage arrhythmias with beta-blockers or calcium channel blockers; infective endocarditis (IE) prophylaxis NOT routinely needed | Observation for small VSDs (high spontaneous closure rate); diuretics + ACE inhibitors for heart failure; anti-failure treatment to allow spontaneous closure | Premature infants: Indomethacin (COX inhibitor - reduces prostaglandin E2) or Ibuprofen IV - accelerates closure; Acetaminophen (alternative); surgical ligation if pharmacotherapy fails |
| Interventional / Catheter-based | Transcatheter closure (now >60% of ASD interventions) - Amplatzer Septal Occluder for secundum defects up to 3.5 cm with adequate rims; requires adequate septal rims | Amplatzer device closure - good results; risk of heart block with paramembranous device closure (proximity to conduction system) | Transcatheter coil or device occlusion - treatment of choice in most centers; Amplatzer duct occluder |
| Surgical | Surgical patch closure (direct suture, autologous pericardium, or prosthetic patch) on cardiopulmonary bypass - indicated for primum, sinus venosus, and defects not suitable for device closure | Patch repair on CPB with moderate hypothermia and cardioplegic arrest; right atrial approach for most; right ventriculotomy for apical muscular VSDs; pulmonary artery band as temporizing for "Swiss-cheese" VSDs | Surgical ligation/division via left posterolateral thoracotomy - gold standard in premature infants not responding to indomethacin; video-assisted thoracoscopic surgery (VATS) available |
| Indications for closure | Right-sided heart enlargement with or without symptoms; Qp:Qs >1.5:1; before school age recommended | Large defects: repair in infancy to prevent irreversible pulmonary vascular changes; moderate defects: close if Qp:Qs >1.5:1; small restrictive: observe | Any hemodynamically significant PDA; small PDA: close due to endarteritis risk (0.45%/year after 2nd decade) |
| Contraindication to closure | Eisenmenger syndrome (irreversible pulmonary HTN) | Eisenmenger syndrome | Eisenmenger with R-to-L shunt; severe irreversible pulmonary HTN |
6. COMPLICATIONS
| Complication | ASD | VSD | PDA |
|---|---|---|---|
| Pulmonary hypertension / Eisenmenger | Late, less common in secundum; possible with large/primum defects | ~10% of large unrepaired VSDs; develops early (first year of life with large defects) | ~5% of isolated PDAs |
| Arrhythmias | Atrial fibrillation, atrial flutter, SVT - common in adults; intraatrial reentrant tachycardia post-surgical repair | Less common; conduction defects post-surgery (LBBB, heart block) | Atrial arrhythmias with large shunts |
| Heart failure | Right heart failure (RV volume overload); leading long-term morbidity | Biventricular failure with large VSDs; leading cause of death if large defect untreated | Congestive heart failure - leading cause of death in untreated isolated PDA (~30% mortality untreated) |
| Infective endocarditis / endarteritis | Low risk for unclosed ASD (IE prophylaxis not routinely recommended) | Risk present, especially with small VSDs (turbulent jet); prophylaxis considered | Endarteritis - ~0.45%/year especially with small PDA; rarely fatal with early antibiotic treatment |
| Paradoxical embolism / Stroke | R-to-L shunting (even transient with Valsalva) enables venous thrombus crossing to systemic circulation → CVA | Less significant | Differential embolism to lower extremities with Eisenmenger |
| Aortic regurgitation | Uncommon | Supracristal/outlet VSDs → aortic cusp prolapse → aortic regurgitation | Uncommon |
| Recurrent respiratory infections | Common in children with large shunts | Common with large left-to-right shunts | Common |
| Post-repair complications | Arrhythmias (scar-related AFL), residual shunt, device embolization | Residual VSD, heart block (esp. paramembranous device closure), arrhythmias | Recurrent PDA, chylothorax (surgical), vocal cord palsy (left recurrent laryngeal nerve injury) |
7. DIFFERENTIALS
| Differential | Why it mimics | How to distinguish |
|---|---|---|
| Patent Foramen Ovale (PFO) | Like ASD but no fixed shunt at rest | PFO: no fixed shunt on TTE; only R-to-L with Valsalva on TEE + bubble study; no RA/RV enlargement |
| Pulmonary stenosis | Ejection systolic murmur at 2nd left ICS like ASD | PS: S2 is normally split but NOT fixed; harsh murmur with ejection click; RV hypertrophy on ECG; echo confirms |
| Mitral stenosis | Mid-diastolic murmur (large ASD may have tricuspid flow rumble) | MS: murmur at apex, opening snap, no fixed S2 split; LA not RA enlargement |
| VSD vs ASD | Both are left-to-right shunts | VSD: harsh holosystolic murmur LLSB with thrill; LV enlargement; O2 step-up at RV level; no fixed S2 split |
| VSD vs AVSD | Both septal defects | AVSD: left axis deviation on ECG; associated AV valve abnormality; Down syndrome common |
| PDA vs Aortopulmonary window | Both continuous murmurs | AP window: murmur at upper sternal border; diagnosed on echo/angio; requires surgical repair (no catheter closure) |
| PDA vs Peripheral pulmonic stenosis | Continuous murmur | PPS: radiates to axillae and back; no bounding pulses; seen in neonates, Williams syndrome, Alagille syndrome |
| PDA vs Aortic stenosis + AR (to-and-fro) | Continuous-sounding murmur | AS+AR: murmur changes with posture; maximal at aortic area; echocardiography diagnostic |
| Eisenmenger syndrome (any) | Cyanosis + pulmonary HTN may obscure original defect | History; differential cyanosis in PDA (toes > fingers); cardiac catheterization for O2 step-up level |
Quick Memory Aid: The "3 Left-to-Right Shunts"
| ASD | VSD | PDA | |
|---|---|---|---|
| Where | Atrial septum | Ventricular septum | Aorta to PA |
| Murmur | Soft ESM (2nd LICS) + Fixed split S2 | Harsh PSM (LLSB) + thrill | Continuous "machinery" (left infraclavicular) |
| O2 step-up at | Right atrium | Right ventricle | Pulmonary artery |
| Heart enlarged | RV + RA | LV + LA (± RV with PHT) | LV + LA |
| ECG | IRBBB + RAD | RVH / LVH | LVH |
| Spontaneous closure | Rare | Common (small muscular) | Yes (term infants); indomethacin (premature) |
| Special feature | Fixed S2 split | Restrictive small VSD = louder murmur | Bounding pulses + wide pulse pressure |
| Eisenmenger | Rare | 10% (large) | 5% |
Key Exam Points to Remember:
- ASD hallmark: Wide, fixed S2 splitting that does not change with respiration - this is pathognomonic
- VSD: Most common CHD overall; harsh holosystolic murmur with thrill at LLSB; large VSDs can have equal LV/RV pressures (so murmur may be softer than expected)
- PDA: Indomethacin works in premature infants (prostaglandin-mediated closure); doesn't work well in term infants where functional closure has already failed; differential cyanosis (feet > hands) is diagnostic of PDA + Eisenmenger
- Eisenmenger: Irreversible pulmonary HTN with shunt reversal - closure is contraindicated once established
- All three start as L-to-R shunts → pulmonary overcirculation → pulmonary HTN → R-to-L reversal → cyanosis (Eisenmenger)
Next is cyanotic congenital heart diseases -etiolgy, pathogenesis & hemodynamics, cigns and symptoms, investigations management and complications comparison table
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Loading Image
I now have excellent content from multiple authoritative sources, plus two key diagrams. Let me compile the comprehensive comparison table.
Cyanotic Congenital Heart Diseases - Complete Comparison
Sources: Robbins & Kumar Basic Pathology, Rosen's Emergency Medicine, Sabiston Textbook of Surgery, Schwartz's Principles of Surgery, Robbins, Cotran & Kumar Pathologic Basis of Disease
Classification by Pulmonary Blood Flow
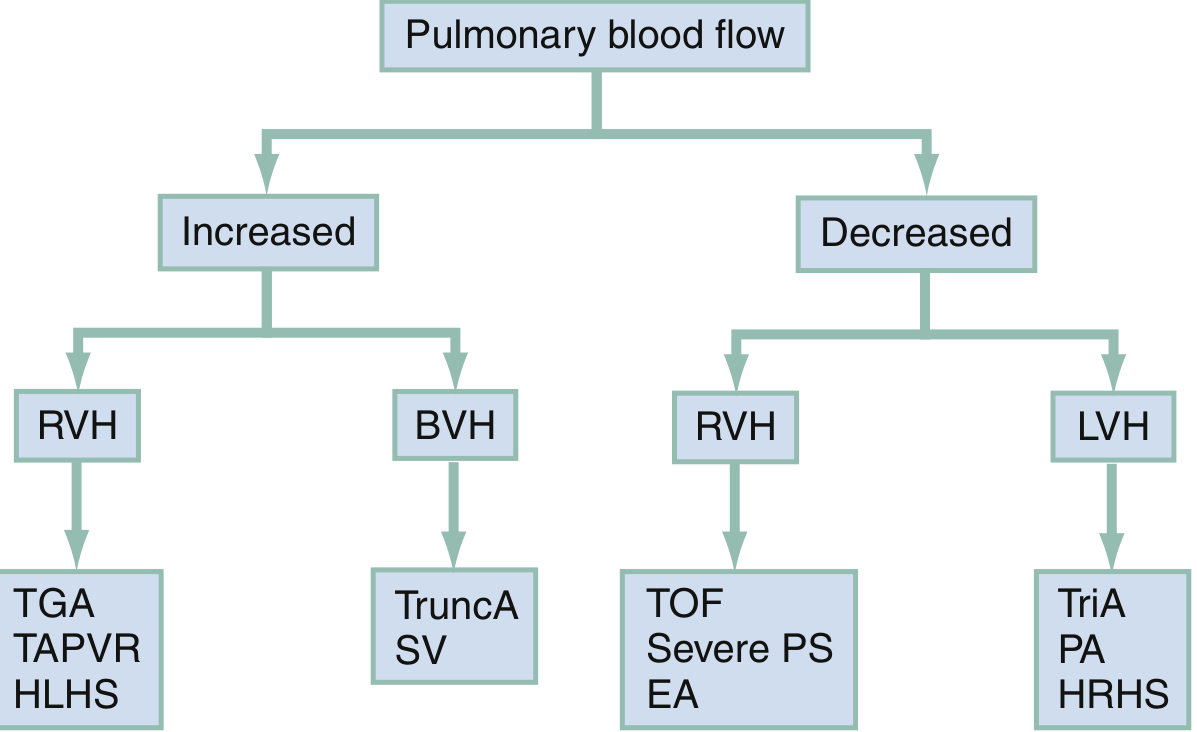
Clinical diagnostic framework: Increased vs Decreased pulmonary blood flow, and ventricular hypertrophy pattern
The "5 T's" of Cyanotic CHD
| TOF | TGA | Tricuspid Atresia | Truncus Arteriosus | TAPVR | |
|---|---|---|---|---|---|
| Full name | Tetralogy of Fallot | Transposition of Great Arteries (D-TGA) | Tricuspid Atresia | Persistent Truncus Arteriosus | Total Anomalous Pulmonary Venous Return |
| Incidence / Frequency | Most common cyanotic CHD beyond infancy; ~5% of all CHD | 2-3 per 10,000 live births; most common cyanotic CHD in neonates | 2-3% of all CHD; most common form of functionally single-ventricle physiology | 1-2% of all CHD; rare | 1-2% of all cardiac malformations |
| Pulmonary blood flow | Decreased | Increased | Decreased (usually) | Increased (massively) | Increased (but obstructed = emergency) |
| ECG pattern | RVH | RVH | LVH (unique - left ventricle does all the work) | BVH (biventricular hypertrophy) | RVH |
TOF Anatomy Diagram
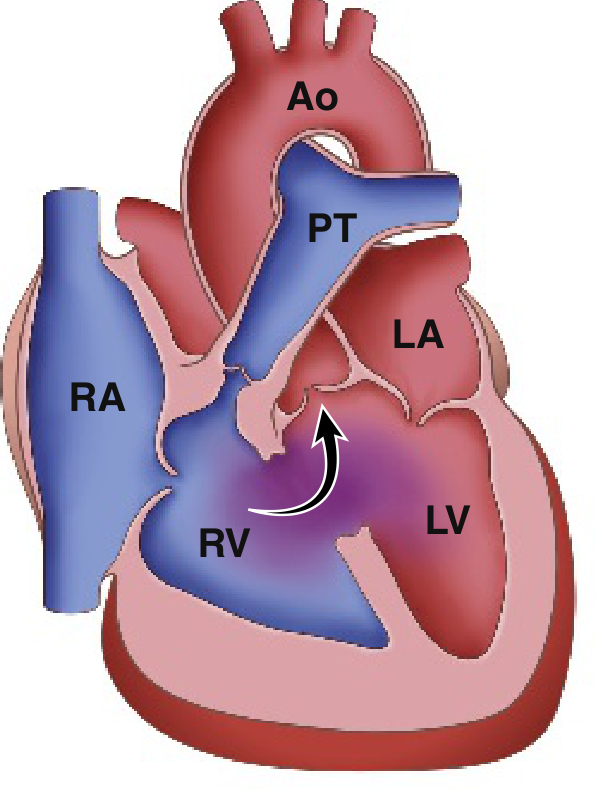
Fig. 9.4A - Robbins & Kumar Basic Pathology: Classic Tetralogy of Fallot. Arrow = R-to-L shunt from RV through VSD into overriding aorta
1. ETIOLOGY & EMBRYOLOGY
| Feature | TOF | TGA (D-TGA) | Tricuspid Atresia | Truncus Arteriosus | TAPVR |
|---|---|---|---|---|---|
| Embryologic defect | Anterosuperior displacement of the infundibular septum → abnormal septation between pulmonary trunk and aortic root; single embryologic error causing all 4 features | Failure of the aortopulmonary septum to spiral during division; results in aorta arising from RV and PA from LV (ventriculoarterial discordance with concordant AV connections) | Unequal division of the AV canal → absent tricuspid valve; mitral valve becomes larger than normal; RV is underdeveloped (hypoplastic) | Arrest of separation of the embryonic truncus arteriosus into aorta and PA; single great vessel overrides ventricular septum (VSD always present); neural crest cell migration failure | Failure of the pulmonary vein evagination from the posterior LA surface to fuse with pulmonary venous plexus around lung buds; persistent connection to splanchnic plexus |
| Associated conditions | Right-sided aortic arch (25%); ASD; anomalous coronary origin; 22q11 deletion (DiGeorge); Down syndrome | Usually isolated; associated with VSD (TGA-VSD) or intact ventricular septum (TGA-IVS); aortic arch hypoplasia/coarctation with VSD variant | ASD (obligatory - PFO/ASD needed to survive); VSD (variable); PDA (pulmonary blood flow often duct-dependent) | DiGeorge syndrome / 22q11 deletion (neural crest association); truncal valve abnormalities (bi- or quadricuspid 30-40%); anomalous coronary arteries (50%) | ASD/PFO (obligatory - only route for oxygenated blood to reach LA); associated with asplenia/polysplenia syndromes |
| Risk factors | Maternal diabetes; alcohol; phenylketonuria; rubella; genetic (22q11) | Maternal diabetes (strongest association); male sex predominance | Sporadic; occasional association with TGA | 22q11 microdeletion; sporadic | Sporadic; associated with asplenia syndrome |
| Sex ratio | M = F | Male predominance (2:1) | M = F | M = F | M = F |
2. PATHOGENESIS & HEMODYNAMICS
| Feature | TOF | TGA (D-TGA) | Tricuspid Atresia | Truncus Arteriosus | TAPVR |
|---|---|---|---|---|---|
| Core anatomical defect | 4 components: (1) large unrestrictive VSD; (2) RVOTO (subpulmonic stenosis most common, also valvular or pulmonary atresia); (3) overriding aorta receiving blood from both ventricles; (4) RVH | Aorta arises from RV (anterior, rightward); PA arises from LV (posterior, leftward) - parallel circulations instead of normal series connection | No connection between RA and RV (tricuspid valve atretic); hypoplastic RV; obligatory ASD for survival; pulmonary flow via PDA or small VSD | Single great artery (truncus) overrides the VSD and gives rise to both aorta and PA; coronary arteries also from truncus | All 4 pulmonary veins drain into systemic venous system (RA or its tributaries) instead of LA; oxygenated blood reaches LA only via ASD/PFO |
| Shunt direction | R-to-L across VSD (due to RVOTO raising RV pressure above LV); deoxygenated blood enters aorta | Parallel circuits - no true shunting; pulmonary and systemic circulations run in parallel, not series; mixing only at level of ASD, VSD, or PDA | R-to-L at atrial level (RA → LA through ASD) | Obligatory mixing at truncal level (VSD + truncal valve); then non-restrictive L-to-R shunt into pulmonary circulation | Obligatory mixing at RA level; both venous streams mix in RA → L-to-R at atrial level (ASD/PFO) for LA filling |
| Mechanism of cyanosis | RVOTO diverts deoxygenated RV blood through VSD into overriding aorta → systemic desaturation | Aorta receives only deoxygenated systemic venous return (from RV); PA receives only oxygenated pulmonary venous return (from LV) - circulations are disconnected unless mixing occurs | Deoxygenated blood from RA crosses ASD into LA, mixes with pulmonary venous return, enters systemic circulation | Mixing of systemic and pulmonary venous blood at truncal level; SpO2 ~85% (depends on Qp:Qs ratio) | All oxygenated pulmonary venous blood diverted to RA; mixed (partially oxygenated) blood crosses ASD to LA |
| Pulmonary blood flow | Decreased (RVOTO restricts flow) | Increased (entire LV output goes to PA) - leads to pulmonary overcirculation | Decreased (usually duct-dependent) | Massively increased - entire cardiac output passes through both lungs; rapid development of pulmonary vascular disease | Depends on obstruction: Unobstructed TAPVR = increased (pulmonary overcirculation + CHF); Obstructed TAPVR = decreased (pulmonary edema, severe cyanosis - surgical emergency) |
| Hemodynamic consequence | RV pressure = LV pressure (unrestrictive VSD equalizes pressures); degree of cyanosis proportional to RVOTO severity; LV normal size | LV faces low pulmonary vascular resistance → LV may become thin and incapable of supporting systemic circulation over time; RA-LA mixing determines survival saturation | LV volume-overloaded (receives both systemic and pulmonary return); RA enlarged; RV hypoplastic | Volume + pressure overload of both ventricles; rapid pulmonary HTN development (may develop by 6 months); truncal valve stenosis/regurgitation adds to load | Right heart dilated; pulmonary hypertension common; with obstruction: pulmonary venous HTN, pulmonary edema |
| Tet spells (TOF only) | Paroxysmal hypercyanotic spells: acute RVOTO worsening (infundibular spasm) → more R-to-L shunting → severe cyanosis → hypoxia → acidosis → worsens spasm (vicious cycle) | N/A | N/A | N/A | N/A |
| Special physiology | "Pink TOF" - if RVOTO is mild, initial L-to-R shunt with no cyanosis (resembles VSD); RVOTO worsens as child grows → increasing cyanosis over time | Survival depends entirely on mixing at ASD, VSD, or PDA; TGA-IVS = most critical (no mixing without intervention) | Pulmonary blood flow duct-dependent in most; some (with large VSD + no RVOTO) may have excess pulmonary flow + CHF | Pulmonary HTN earliest of all 5 Ts - irreversible changes possible by 6 months | Infracardiac type TAPVR with obstruction = TRUE surgical emergency (only cardiac surgery emergency with no palliation option) |
3. SIGNS & SYMPTOMS
| Feature | TOF | TGA (D-TGA) | Tricuspid Atresia | Truncus Arteriosus | TAPVR |
|---|---|---|---|---|---|
| Age of presentation | Not always at birth; worsening cyanosis over weeks-months; "pink TOF" may be asymptomatic initially | First days of life (especially TGA-IVS) - profound neonatal cyanosis | Within days of birth (duct-dependent pulmonary flow); some not until PDA closes | Neonatal period - CHF + cyanosis from birth | Unobstructed: CHF in first weeks; Obstructed: Severe cyanosis + respiratory distress at birth |
| Cyanosis | Progressive; worse with crying, feeding, exertion; relieved by squatting | Profound from birth (especially TGA-IVS); paradoxically "blue" despite normal-sounding heart initially | From birth; profound | Moderate; SpO2 ~85% (mixing at truncal level prevents extreme cyanosis) | Variable; obstructed type = profound cyanosis from birth |
| Squatting (TOF only) | Classic - child squats to relieve cyanosis: increases systemic vascular resistance → reduces R-to-L shunting → more blood goes to lungs | Not applicable | Not applicable | Not applicable | Not applicable |
| Tet spells | Hypercyanotic (Tet) spells: sudden onset intense cyanosis, irritability, hyperpnea, limpness, LOC; worst in morning/after feeding; may → syncope, CVA, death | No | No | No | No |
| Heart failure symptoms | Uncommon early (decreased pulmonary flow); failure to thrive | Tachypnea, poor feeding, tachycardia with large VSD variant (TGA-VSD); otherwise cardiac failure not prominent early | Uncommon (decreased flow); failure to thrive | Prominent CHF: tachypnea, poor feeding, diaphoresis, failure to thrive; CHF + cyanosis is classic combination | Unobstructed: CHF symptoms; Obstructed: severe respiratory distress, pulmonary edema |
| Murmur | Ejection systolic murmur at left sternal border (RVOTO); VSD itself is usually silent (unrestrictive = equal pressures); paradox: louder murmur = less severe TOF (more obstruction = softer murmur as less flow crosses RVOT) | Absent or soft murmur in TGA-IVS; murmurs relate to associated defects (VSD, PS) | Soft; related to associated VSD or ASD | Systolic murmur + sometimes diastolic component from truncal regurgitation; single S2 (only one semilunar valve) | Non-specific murmur or absent; features of right heart enlargement |
| S2 | Single S2 (pulmonary component absent/soft due to hypoplastic PA) | Single loud S2 (aorta is anterior - A2 is loud and P2 is posterior/obscured) | Variable | Single S2 (single semilunar valve) | May be widely split |
| Clubbing | Present - chronic hypoxemia | Present with uncorrected TGA | Present | Less prominent (SpO2 not as low) | Present with chronic uncorrected disease |
| Polycythemia | Present - compensatory; raises risk of cerebral venous thrombosis | Present in chronic cases | Present | Less marked | Present in unobstructed (long-standing) |
| Special signs | Infants: hyperpnea during spells; older children: growth retardation, exercise intolerance | "Egg on a string" appearance on CXR; profound cyanosis out of proportion to respiratory distress | Hepatomegaly; signs of RA enlargement | Bounding pulses (wide pulse pressure from pulmonary overcirculation); signs of CHF | Obstructed type: severe respiratory distress mimicking RDS |
4. INVESTIGATIONS
| Investigation | TOF | TGA (D-TGA) | Tricuspid Atresia | Truncus Arteriosus | TAPVR |
|---|---|---|---|---|---|
| ECG | RVH (right axis deviation, tall R in V1); right ventricular strain pattern | RVH (right axis deviation - paradoxically RV is "systemic" ventricle); may look normal at birth | LVH (hallmark - LV does all work); Left axis deviation (superior QRS axis); RA enlargement | BVH (biventricular hypertrophy); combined ventricular enlargement | RVH; right axis deviation; P pulmonale; RBBB pattern |
| Chest X-ray | "Boot-shaped" heart (coeur en sabot): RVH elevates cardiac apex; concavity at pulmonary artery segment; decreased pulmonary vascular markings (oligemic lung fields); right-sided aortic arch in 25% | "Egg on a string" / "egg on its side": narrow superior mediastinum (great vessels overlapping = no thymic shadow), oval-shaped cardiac silhouette; increased pulmonary vascular markings (plethoric lung fields) | Cardiomegaly (RA + LV enlarged); normal or decreased pulmonary markings depending on pulmonary flow; left-sided cardiac apex (due to LV dominance) | Cardiomegaly (biventricular); increased pulmonary vascular markings; right-sided aortic arch in 30%; absent main PA segment (replaced by truncal artery) | "Snowman"/"Figure-of-8" appearance (supracardiac type - left SVC + left innominate vein form top of snowman + cardiac shadow = bottom); increased markings in unobstructed; white-out/pulmonary edema in obstructed |
| Echocardiography | Diagnostic: VSD, overriding aorta (>50% override), RVOTO, RVH; PA size assessment; coronary artery anatomy | Diagnostic: demonstrates AV concordance + ventriculoarterial discordance; identifies associated VSD, PS, ASD; LV morphology assessment for arterial switch timing | Shows absent tricuspid valve, hypoplastic RV, ASD, VSD; LV dilation; great vessel relationship; PDA assessment | Single truncal valve (trileaflet, bicuspid, or quadricuspid); VSD; PA origin from truncus; truncal valve regurgitation/stenosis | Identifies site of anomalous pulmonary venous drainage; presence/absence of obstruction; ASD/PFO; right heart dilation |
| Cardiac catheterization | O2 saturation step-DOWN at RV level; PA pressure low; coronary anatomy if echo inconclusive; not routine for diagnosis | O2 saturation "step-up" pattern complex; useful to assess pulmonary vascular resistance; less needed if echo diagnostic | Angiography shows anatomy; PA pressure and resistance measurement | PA pressures and resistance measurement (critical for surgical planning); truncal valve assessment | PA pressure and resistance; differentiate types; obstructed vs unobstructed |
| Cardiac MRI/CT | Coronary artery anatomy, PA branch sizes pre-operatively | LV mass and function assessment (pre-arterial switch); post-operative baffle assessment | Pre-Fontan anatomical mapping; pulmonary artery sizes | Pulmonary artery anatomy; coronary origins (50% anomalous) | Pulmonary vein anatomy; drainage pathway assessment |
| Hyperoxia test | PaO2 fails to rise significantly above 150 mmHg on 100% O2 (distinguishes cardiac from pulmonary cyanosis) | PaO2 fails to rise | PaO2 fails to rise | PaO2 minimal rise | PaO2 minimal rise |
5. MANAGEMENT
| Aspect | TOF | TGA (D-TGA) | Tricuspid Atresia | Truncus Arteriosus | TAPVR |
|---|---|---|---|---|---|
| Emergency stabilization | PGE1 if duct-dependent (severe RVOTO/pulmonary atresia variant); Tet spell management: knee-chest position, IV morphine, IV beta-blocker (propranolol), IV phenylephrine (↑SVR), O2, fluids, correct acidosis | PGE1 immediately to maintain/open PDA for mixing; balloon atrial septostomy (Rashkind procedure) to create/enlarge ASD for adequate atrial mixing; achieves SpO2 70-80% | PGE1 if duct-dependent; stabilize with ASD if too small | PGE1 usually NOT used (would worsen pulmonary overcirculation); anti-failure therapy (diuretics, digoxin) | Obstructed TAPVR = true surgical emergency - no palliation possible; immediate surgery; PGE1 contraindicated (would worsen pulmonary overcirculation) |
| Palliative surgery | Blalock-Taussig (BT) shunt (modified - subclavian artery to PA with Gore-Tex conduit) if complete repair not feasible (small infant, hypoplastic PA); increases pulmonary blood flow | Balloon atrial septostomy (Rashkind) is itself palliative to bridge to definitive repair | Staged palliation (mandatory for single ventricle physiology): Stage 1: Blalock-Taussig shunt (if too little PBF) OR PA banding (if too much PBF); Stage 2: Glenn shunt (SVC to PA, bidirectional cavopulmonary connection) at ~6 months; Stage 3: Fontan completion (IVC to PA) at 2-4 years | PA banding if early repair not feasible | N/A for obstructed type (emergency repair only) |
| Definitive surgery | Complete intracardiac repair on CPB: VSD patch closure + RVOTO relief (resection of infundibular muscle, pulmonary valvotomy/valvectomy ± transannular patch); ideally in first 6 months | Arterial Switch Operation (ASO) / Jatene procedure - definitive repair; aorta re-anastomosed to LV, PA re-anastomosed to RV; coronary buttons transferred; must be done within first 2-3 weeks of life before LV "deconditions" to low pulmonary pressure | Fontan procedure (total cavopulmonary connection): IVC connected to PA; RA excluded from systemic circulation; single ventricle (LV) pumps to systemic and pulmonary circuits in series | Complete repair on CPB in neonatal period: (1) Pulmonary arteries detached from truncus + connected to RV via conduit; (2) VSD closed to direct LV output to truncus (aorta); early repair essential (pulmonary HTN by 6 months) | Surgical re-anastomosis of pulmonary veins to LA; ASD closure; resection of obstructing membrane; emergent in obstructed type |
| Historical operations (TGA) | N/A | Mustard/Senning procedure (atrial switch - now historical): intraatrial baffles redirect venous blood; physiologically corrected but morphologic RV remains systemic ventricle → long-term RV failure | N/A | N/A | N/A |
| Medical management | Propranolol for Tet spell prophylaxis; iron supplementation (iron deficiency worsens polycythemia complications) | PGE1 infusion preoperatively; anti-failure therapy for TGA-VSD with CHF | Diuretics + ACE inhibitors for volume overload; anti-coagulation post-Fontan (warfarin/aspirin) | Diuretics, digoxin, ACE inhibitors preoperatively; rapid deterioration means early surgical planning | Furosemide for pulmonary edema in obstructed type (bridge to surgery only) |
| Timing of definitive repair | Complete repair: ideally 3-6 months (avoid polycythemia complications); symptomatic neonates with duct-dependent flow: emergency BT shunt or primary repair | ASO: within first 2-3 weeks of life (before LV regression); TGA-VSD: up to 6-8 weeks | Glenn: ~6 months; Fontan: 2-4 years | Neonatal period (within first few weeks); do NOT delay - PVR irreversible by 6 months | Obstructed: immediate surgical emergency (hours); unobstructed: within first few weeks |
6. COMPLICATIONS
| Complication | TOF | TGA (D-TGA) | Tricuspid Atresia | Truncus Arteriosus | TAPVR |
|---|---|---|---|---|---|
| If untreated | Death; cerebral abscess (paradoxical emboli), cerebral venous thrombosis (polycythemia), progressive hypoxia, infective endocarditis | Death within weeks (TGA-IVS); progressive cyanosis and hypoxia | Death from hypoxia; high early mortality | Rapidly progressive CHF + pulmonary HTN; death usually in infancy | Obstructed: death in hours/days; unobstructed: CHF → death within months-years |
| Post-repair | Pulmonary regurgitation (most common long-term issue after transannular patch repair) → progressive RV dilation → RV failure → arrhythmias; residual RVOTO; residual VSD; ventricular arrhythmias / sudden death (RBBB + left anterior fascicular block = bifascicular block is common post-repair marker); pulmonary valve replacement often needed in adulthood | Atrial switch (historical): RV failure (morphologic RV as systemic ventricle), atrial arrhythmias, baffle obstruction/leak, sudden death; ASO: coronary artery problems (kinking/stenosis), neoaortic root dilation, pulmonary stenosis at anastomosis | Fontan circulation complications: protein-losing enteropathy (PLE - 10%), plastic bronchitis, Fontan failure, arrhythmias (atrial flutter), thromboembolism, hepatic fibrosis/cirrhosis (long-term), lymphatic dysfunction | Truncal valve regurgitation (progressive - most important); conduit failure/obstruction (RV-to-PA conduit requires replacement as child grows); pulmonary HTN if late repair | Pulmonary vein stenosis (most feared post-repair complication - difficult to treat); recurrent obstruction; arrhythmias; residual ASD |
| Infective endocarditis | Risk present (repaired/unrepaired) - IE prophylaxis recommended | Risk post-operatively | Risk present | Risk present | Risk present |
| Polycythemia/hyperviscosity | Cerebral venous thrombosis; cerebral abscess (paradoxical embolism through VSD) | Present | Present | Mild | Present |
| Arrhythmias | Ventricular arrhythmias post-repair (scarring from ventriculotomy); RBBB common; sudden cardiac death (lifetime risk) | Atrial arrhythmias (especially post-atrial switch) | Atrial arrhythmias (especially post-Fontan) | Conduction abnormalities | Arrhythmias post-repair |
Quick Comparison Summary Table
| Feature | TOF | TGA | Tricuspid Atresia | Truncus Arteriosus | TAPVR |
|---|---|---|---|---|---|
| Cyanosis onset | Weeks-months | Day 1-2 of life | Within days | Birth | Birth (obstructed) or weeks (unobstructed) |
| Pulmonary flow | Decreased | Increased | Decreased | Massively increased | Increased (or obstructed = emergency) |
| CXR finding | Boot-shaped heart | Egg on string | Cardiomegaly + LAH | Cardiomegaly + plethora + no main PA shadow | Snowman sign (supracardiac type) |
| ECG hallmark | RVH | RVH | LVH + LAD | BVH | RVH |
| Emergency Rx | PGE1 (severe); Knee-chest for Tet spell | PGE1 + Rashkind septostomy | PGE1 | Anti-failure (NOT PGE1) | Immediate surgery (obstructed) |
| Definitive Rx | Complete repair + RVOTO relief | Arterial Switch Op (within 2-3 weeks) | Staged Fontan (Glenn → Fontan) | Neonatal complete repair | Pulmonary vein re-anastomosis to LA |
| Key complication | PR → RV failure; VT/SCD | RV failure (Mustard/Senning era); coronary stenosis (ASO) | Fontan failure, PLE | Truncal valve regurgitation; conduit failure | Pulmonary vein stenosis (post-repair) |
| Murmur character | Ejection systolic (RVOTO); single S2 | Absent/soft; single loud S2 | Variable | Systolic ± diastolic; single S2 | Non-specific or absent |
| Unique sign | Squatting; Tet spells | Cyanosis out of proportion to respiratory distress | LVH on ECG (paradox) | CHF + cyanosis together | Snowman CXR; "white-out" if obstructed |
Key Memory Mnemonics
The 5 T's: Truncus, Transposition, Tricuspid atresia, Tetralogy of Fallot, TAPVR
TOF "PROVE": Pulmonary stenosis (RVOTO), Right ventricular hypertrophy, Overriding aorta, VSD, (E) = all from one Embryologic defect (infundibular septal displacement)
TGA rule: "Arteries are transposed" = Aorta from RV (wrong!), PA from LV (wrong!) = parallel circuits = death unless mixing
Tet spell management "MOPKF": Morphine, O2, Propranolol/Phenylephrine, Knee-chest position, Fluids + bicarbonate
TAPVR CXR snowman = only in supracardiac type (left vertical vein + left innominate vein + SVC forms "head"; cardiac shadow = "body")
Tricuspid Atresia LVH on ECG = because morphologic LV pumps EVERYTHING (both systemic and pulmonary circuits)
Sources: Rosen's Emergency Medicine p. 1372-1411; Robbins & Kumar Basic Pathology p. 271-325; Sabiston Textbook of Surgery p. 2696-2750; Schwartz's Principles of Surgery p. 398-700; Robbins, Cotran & Kumar Pathologic Basis of Disease p. 990-1003
This is a shared conversation. Sign in to Orris to start your own chat.