Explain Piriformis syndrome etiology , clinical features , daignosis , treatment and physiotherapy managment
Reading File
Finding Sources
Finding Sources
Searching PubMed
"piriformis syndrome" diagnosis treatment
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Loading Image
I now have comprehensive, well-sourced content from multiple authoritative textbooks. Let me compile the complete answer.
Piriformis Syndrome
Anatomy (Foundation for Understanding)
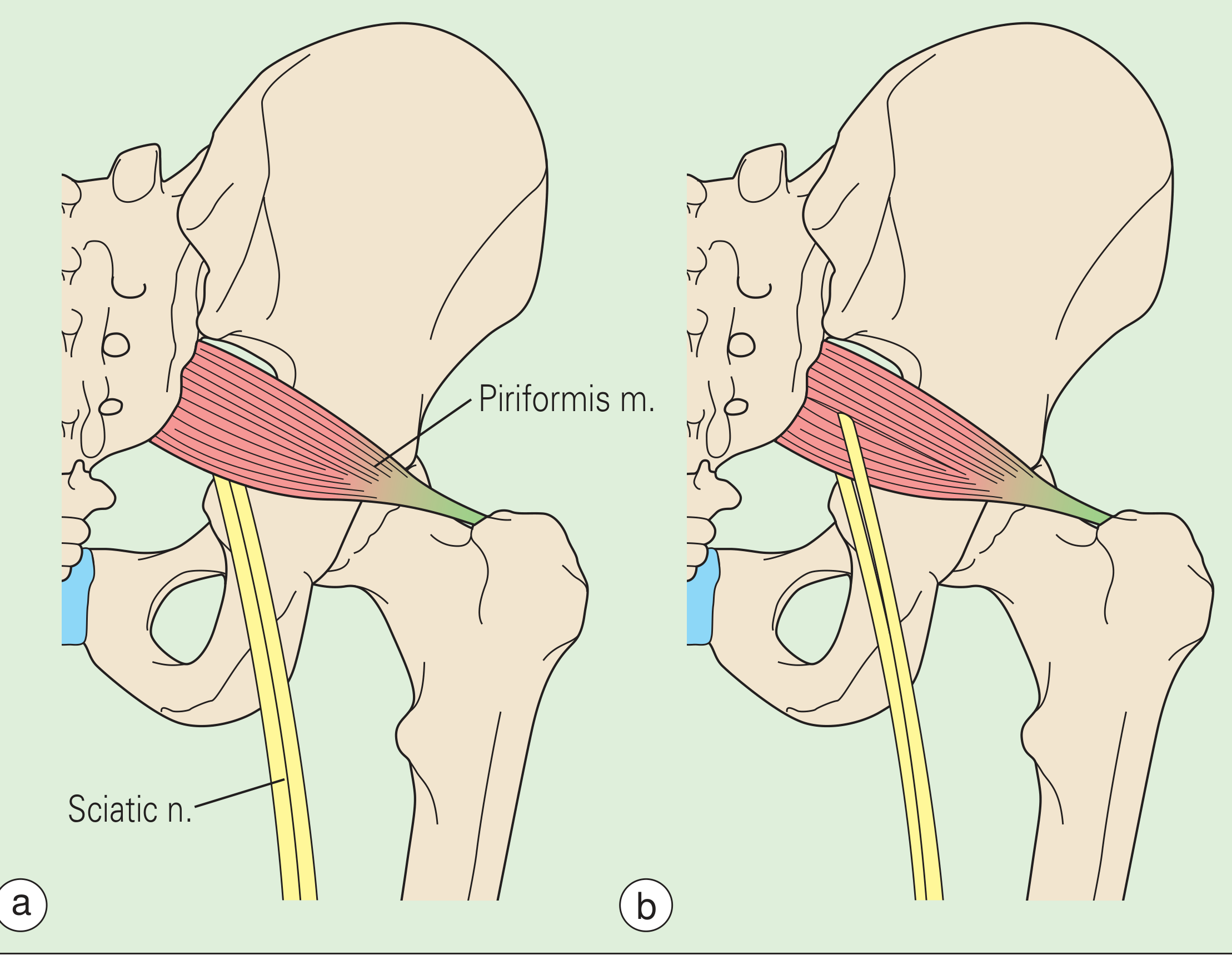
The piriformis muscle originates from the anterior surface of the sacrum and the gluteal surface of the ilium. It exits through the greater sciatic foramen and inserts on the medial aspect of the greater trochanter. Its primary actions are external rotation of the extended hip and internal rotation of the flexed hip, along with abduction in the flexed position.
The sciatic nerve (L4-S3) has a critical spatial relationship with this muscle:
- In 80-94% of people, the sciatic nerve passes anterior to the piriformis belly and exits below it (normal variant)
- In ~14%, the common peroneal division passes through the muscle belly between two heads (bipartite piriformis)
- Rarely, the nerve passes posterior to the muscle
Etiology
Piriformis syndrome results from compression or irritation of the sciatic nerve by the piriformis muscle. It accounts for approximately 5% of patients referred for back and leg pain, though it is widely underdiagnosed.
Primary vs. Secondary
| Type | Description |
|---|---|
| Primary | Intrinsic piriformis pathology: myofascial pain, myositis, anatomical variation (bipartite muscle, anomalous sciatic nerve course) |
| Secondary | Extrinsic causes acting on a normal muscle |
Specific Causes
- Trauma to the gluteal region - the leading cause; results in inflammation, hematoma, or fibrosis of the muscle leading to spasm and sciatic nerve irritation
- Anatomical variants - bipartite piriformis, sciatic nerve passing through the muscle (in these individuals, internal hip rotation directly stretches/compresses the nerve)
- Prolonged overuse - distance runners, cyclists, those with abnormal gait biomechanics
- Muscle hypertrophy - direct mechanical compression
- Ischial bursitis, fascia! constricting bands, or pelvic masses (tumors, hematoma, abscess) compressing the nerve at this level
- Post-surgical - following hip or pelvic surgery
- Infection - abscess in the piriformis region
- Rheumatology, 2-Volume Set (2022, Elsevier), p. 771
- Imaging Anatomy, Vol. 3 - Bones, Joints, Vessels and Nerves, p. 267
- Barash, Cullen, and Stoelting's Clinical Anesthesia 9e, p. 4760
Clinical Features
Symptoms
- Deep buttock pain - the hallmark; typically extends from the sacrum to the greater trochanter
- Radiation - pain and paresthesias radiate to the posterior thigh and may extend along the entire course of the sciatic nerve (posterior leg, foot)
- Aggravating factors: prolonged sitting (driving, biking), rising from sitting, climbing stairs, stooping and lifting, hip flexion + adduction + internal rotation (FADIR)
- Relieving factors: lying supine, walking, hip extension
- Neurologic symptoms: leg numbness and paresthesias when the sciatic nerve is significantly irritated; bowel/bladder symptoms are absent (distinguishing from true radiculopathy)
- Neurological examination is typically negative for motor deficits
Physical Examination Signs
| Sign | How to Elicit | Positive Finding |
|---|---|---|
| Pace sign | Resisted hip abduction in seated position with hip flexed | Pain and weakness |
| Freiberg sign | Forced internal rotation of the extended thigh | Buttock pain |
| Lasègue sign (piriformis variant) | Flexion, adduction, and internal rotation of the hip in supine (FADIR) | Buttock pain radiating to leg |
| Direct palpation | Deep pressure over the gluteal region / sciatic notch | Tenderness and reproduction of pain |
| Rectal/pelvic examination | Internal palpation of the piriformis | Muscle tenderness or palpable spasm |
Note: The straight-leg raise test may be normal or only mildly positive, helping differentiate from true lumbar radiculopathy.
- Barash, Cullen, and Stoelting's Clinical Anesthesia 9e, p. 4759-4760
- Rheumatology, 2-Volume Set (2022, Elsevier), p. 771
- Bradley and Daroff's Neurology in Clinical Practice, p. 4070
Diagnosis
Piriformis syndrome is primarily a clinical diagnosis of exclusion - it should be considered when symptoms of sciatic neuropathy exist without evidence of radiculopathy or spinal stenosis.
Investigations
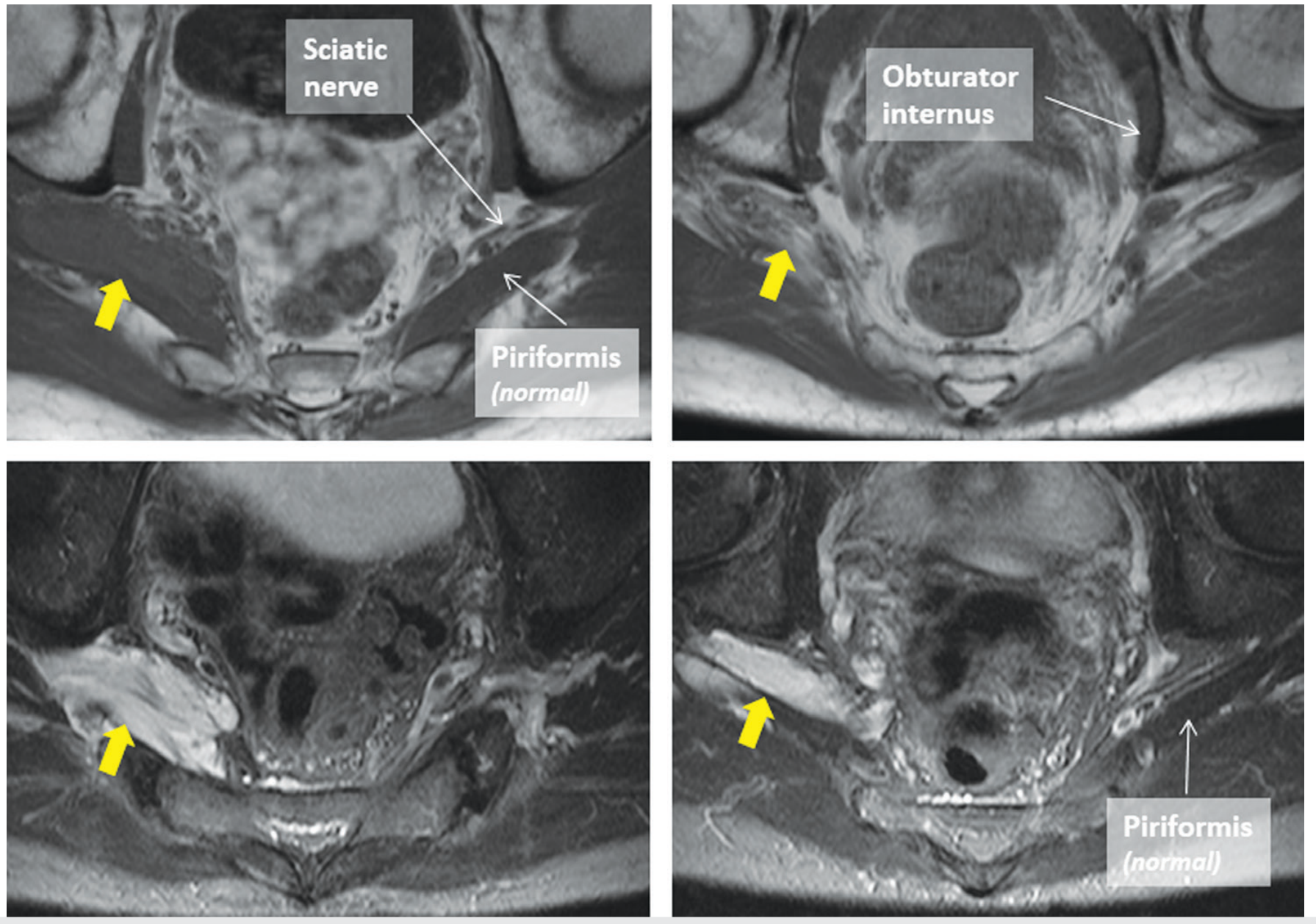
1. MRI (modality of choice)
- Detects inflammation, edema, or hypertrophy of the piriformis muscle
- Defines the spatial relationship between the piriformis and sciatic nerve
- Excludes lumbar disc herniation, spinal stenosis, pelvic mass, tumors, or hematoma
- MR neurography can show sciatic nerve signal changes at the piriformis level
2. EMG / Nerve Conduction Studies
- May detect myopathic or neuropathic changes in sciatic-innervated muscles
- H-reflex delay (peroneal nerve) in the FADIR position vs. neutral position is a positive finding
- Useful to confirm sciatic nerve involvement and exclude L4-S1 radiculopathy
3. Ultrasound
- Can image the piriformis muscle and compare side to side for hypertrophy or asymmetry
- Can guide diagnostic/therapeutic injections
4. CT scan - less useful but guides injection procedures
5. Diagnostic injection
- Local anesthetic (± steroid) injection into the piriformis muscle under CT, fluoroscopy, ultrasound, or nerve stimulator guidance
- Relief of symptoms confirms the diagnosis
Differential Diagnosis
| Condition | Distinguishing Feature |
|---|---|
| Lumbar disc herniation (L4-S1) | Positive SLR, positive neurological signs, disc pathology on MRI |
| Spinal stenosis | Neurogenic claudication, bilateral symptoms, MRI changes |
| Sacroiliac joint syndrome | SI joint line tenderness, positive FABER/Gaenslen tests, SI joint injection response |
| Greater trochanteric bursitis | Lateral hip pain, tenderness at greater trochanter |
| Ischiogluteal bursitis | Pain on direct ischial tuberosity pressure |
- Rheumatology, 2-Volume Set (2022, Elsevier), p. 771
- Bradley and Daroff's Neurology in Clinical Practice, p. 4074
Treatment
Step 1: Conservative (First-Line)
| Intervention | Details |
|---|---|
| NSAIDs | Reduce inflammation and pain (e.g., ibuprofen, naproxen) |
| Muscle relaxants | Address piriformis spasm (e.g., cyclobenzaprine, methocarbamol) |
| Analgesics | Pain control |
| Activity modification | Avoid prolonged sitting, avoid aggravating movements |
| Physical therapy | Core of conservative management (detailed below) |
Step 2: Injection Therapies
Corticosteroid + Local Anesthetic injection into piriformis
- Breaks the pain/muscle spasm cycle
- Guided by CT, fluoroscopy, ultrasound, or electrical nerve stimulation
- May provide weeks to months of relief
Botulinum Toxin (Botox) injection
- Directly reduces muscle spasm by blocking neuromuscular junction
- Can benefit patients who fail corticosteroid injections
- A 2025 review (PMID: 41224378) supports ultrasound-guided botulinum toxin infiltration for piriformis syndrome
Step 3: Surgical (Last Resort)
-
Indicated when conservative measures (usually 6+ months) have failed
-
Procedure: Release of the piriformis from its insertion on the femur, with reattachment in a shortened position, or division of the tendon to decompress the sciatic nerve
-
Controversy exists about indications and expected effectiveness
-
Surgical decompression of the sciatic nerve may be combined with piriformis tenotomy
-
Rheumatology, 2-Volume Set (2022, Elsevier), p. 771
-
Barash, Cullen, and Stoelting's Clinical Anesthesia 9e, p. 4760
-
Bradley and Daroff's Neurology in Clinical Practice, p. 4079
Physiotherapy Management
Physiotherapy is the cornerstone of non-operative treatment and is used at every stage. Goals are to reduce pain, relieve muscle spasm, restore normal muscle length, correct biomechanical faults, and prevent recurrence.
Phase 1: Acute Phase (Pain Relief and Protection)
- Activity modification - avoid prolonged sitting and aggravating positions
- Cryotherapy (ice packs to gluteal region) - 15-20 minutes, several times daily to reduce inflammation
- TENS / Electrotherapy - for pain modulation
- Soft tissue massage - gentle effleurage and petrissage of gluteal region to reduce muscle guarding
- Positional education - how to sit, sleep, and move without aggravating the piriformis
Phase 2: Flexibility and Muscle Length Restoration (Core of PT)
Piriformis stretching - the most important intervention:
- Supine piriformis stretch - Lying supine, cross the affected leg over the opposite knee (figure-4 position), gently pull both legs toward the chest; hold 30 seconds x 3 sets
- Seated piriformis stretch - Seated on chair, place ankle of affected side on opposite knee, lean forward; hold 30 seconds
- Prone stretching - Hip in flexed, adducted, internally rotated (FADIR) position with gentle overpressure
Hip flexor stretching (psoas, iliacus) - tight hip flexors alter pelvic mechanics and increase piriformis loading
Lumbar spine mobilization - if lumbar mobility is restricted, it places compensatory demand on the piriformis
Phase 3: Strengthening and Neuromuscular Control
- Gluteus medius/minimus strengthening - weakness of these muscles is often a contributing factor (side-lying hip abduction, clamshells, resistance band work)
- Gluteus maximus strengthening - bridges, single-leg bridges, hip thrusts
- Core stabilization - transverse abdominis activation, plank progressions, dead bugs; improves lumbopelvic stability and reduces compensatory piriformis overload
- Hip external rotator strengthening - once acute pain has resolved, progressive resistance training of the piriformis and other external rotators (not in the acute phase)
Phase 4: Functional Rehabilitation
- Gait retraining - correction of excessive hip adduction/internal rotation during walking or running (common in female runners with wide Q-angle)
- Running mechanics - increase step rate, reduce crossover gait pattern
- Sport-specific or activity-specific training - gradual return to sport, cycling, lifting
Phase 5: Modalities Used in Physiotherapy
| Modality | Purpose |
|---|---|
| Ultrasound therapy | Deep tissue heating, promotes tissue extensibility before stretching |
| TENS / IFT | Pain modulation |
| Dry needling / trigger point release | Addresses myofascial trigger points in the piriformis and surrounding muscles |
| Deep tissue massage / myofascial release | Reduces muscle tension, improves circulation |
| Heat therapy | Before exercise to warm the muscle |
| Neural mobilization / sciatic nerve flossing | Improves sciatic nerve mobility if neural tension is a component |
Sciatic Nerve Flossing (Neural Mobilization)
Performed in supine: dorsiflex the foot + extend the knee + flex the hip, then reverse - this "flosses" the sciatic nerve through the piriformis and can relieve neural tension symptoms.
Recent Evidence (2024-2026)
Two recent systematic reviews update the understanding of this condition:
- A 2025 systematic review of case reports (PMID: 41068685) consolidates presentations and management strategies
- A 2026 systematic review on anatomical basis (PMID: 41690265) refines the role of anatomical variants in causing symptoms
- A 2024 review by Lo & Robinson (PMID: 38697742) in Handbook of Clinical Neurology provides updated diagnostic and management algorithms
- The concept of "deep gluteal syndrome" is increasingly used to encompass piriformis syndrome along with other causes of sciatic nerve entrapment in the deep gluteal space; a 2025 narrative review (PMID: 41095750) explores muscle-tendon pathologies beyond nerve entrapment in this region
Summary
| Aspect | Key Points |
|---|---|
| Definition | Compression/irritation of sciatic nerve by piriformis muscle at the greater sciatic foramen |
| Leading cause | Gluteal trauma → muscle spasm/inflammation; anatomical variants |
| Classic symptom | Deep buttock pain ± radiation down posterior leg, worsened by sitting |
| Key signs | Pace sign, Freiberg sign, FADIR (Lasègue) sign; no neurological deficits |
| Diagnosis | Clinical + MRI (excludes differentials); EMG (H-reflex delay in FADIR) |
| Treatment | NSAIDs + muscle relaxants → PT → corticosteroid/BTX injection → surgery |
| PT focus | Piriformis stretching, glute strengthening, core stability, neural mobilization |
This is a shared conversation. Sign in to Orris to start your own chat.