I'm finding for medicinal chemistry, topic sympathomimetic and para sympathomimetic drugs synthesis it's basica and uses
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have all the key information needed for a comprehensive answer. Let me compile the full response.
Sympathomimetic & Parasympathomimetic Drugs - Medicinal Chemistry
Source: Katzung's Basic & Clinical Pharmacology, 16th Ed. | Goodman & Gilman's Pharmacological Basis of Therapeutics
PART 1: SYMPATHOMIMETIC DRUGS
1. Parent Structure & Basic Chemistry
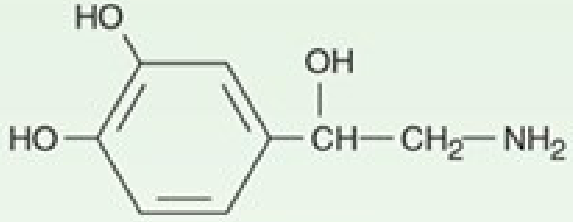
Phenylethylamine is the parent compound from which all sympathomimetic drugs are derived. It consists of a benzene ring with a β-CH₂-α-CH₂-NH₂ side chain.
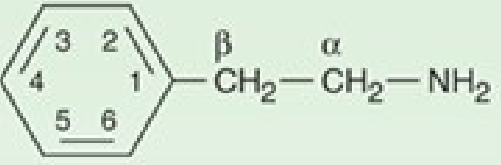
Catecholamines are produced by adding -OH groups at positions 3 and 4 of the benzene ring (the "catechol" nucleus). Key endogenous catecholamines are dopamine, norepinephrine (NE), and epinephrine (Epi).
2. Structure-Activity Relationships (SAR) - Medicinal Chemistry Core
Three sites of chemical modification determine receptor selectivity and pharmacokinetics:
A. Substitution on the Benzene Ring
| Modification | Effect |
|---|---|
| -OH at positions 3 & 4 (catechol) | Maximum α and β activity |
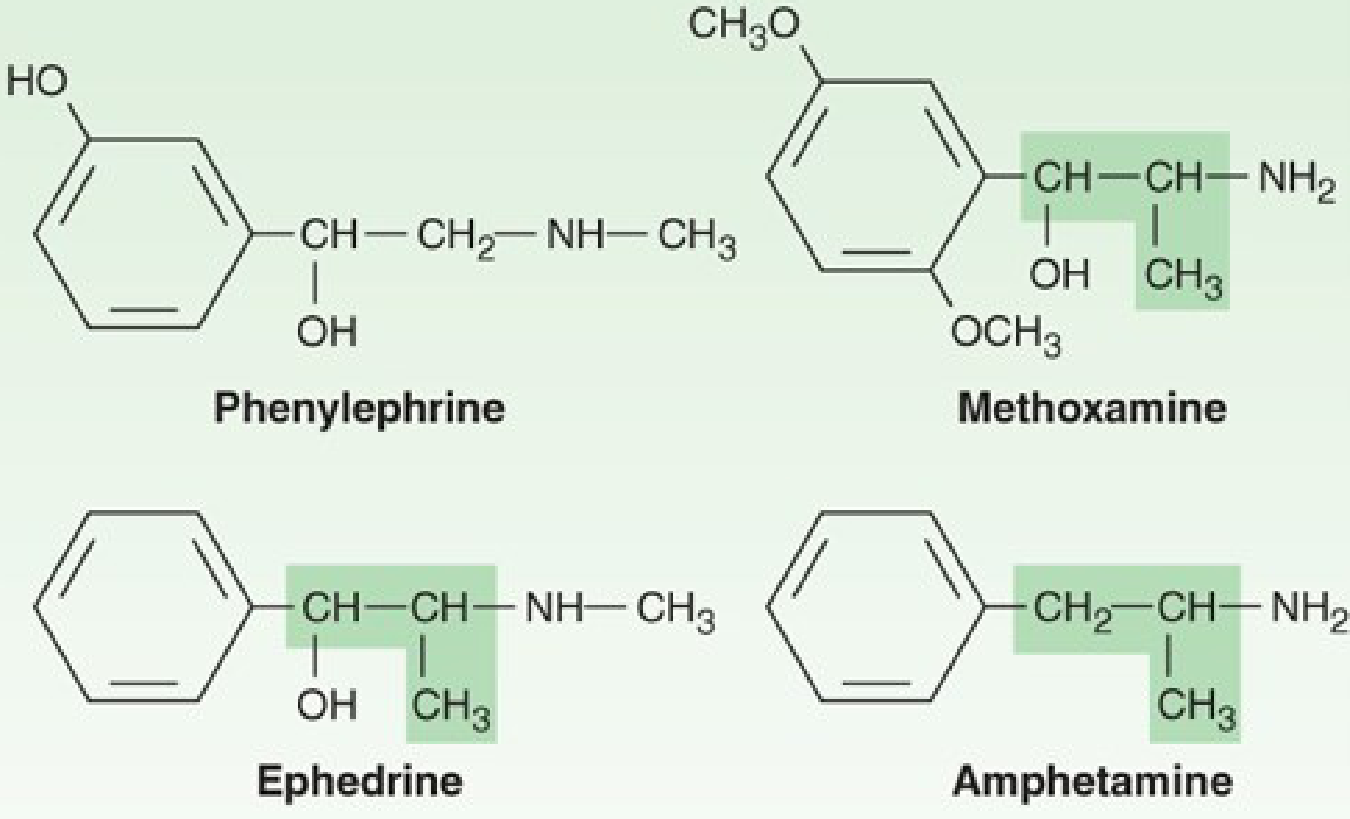
| Loss of one -OH | 100-fold reduction in potency; remaining activity becomes more selective (e.g., phenylephrine = α₁ selective) |
| -OCH₃ in place of -OH (methoxamine) | Resistant to COMT; longer duration |
| No ring -OH groups (ephedrine, amphetamine) | Orally active, longer duration, CNS penetration |
The catechol -OH groups make drugs susceptible to inactivation by COMT (catechol-O-methyltransferase), so catecholamines are NOT orally active. Removal of one or both ring -OHs makes the drug orally bioavailable and CNS-penetrant.
B. Substitution on the Alpha (α) Carbon
| Modification | Effect |
|---|---|
| α-methyl group (e.g., ephedrine, amphetamine) | Blocks MAO metabolism → prolonged action; indirect-acting (releases stored NE) |
| No α-methyl (catecholamines) | Rapid metabolism by MAO |
C. Substitution on the Nitrogen (Amino Group)
| N-substituent | Receptor Preference |
|---|---|
| H (primary amine, norepinephrine) | α₁ = α₂; β₁ >> β₂ |
| -CH₃ (epinephrine) | α and β equally |
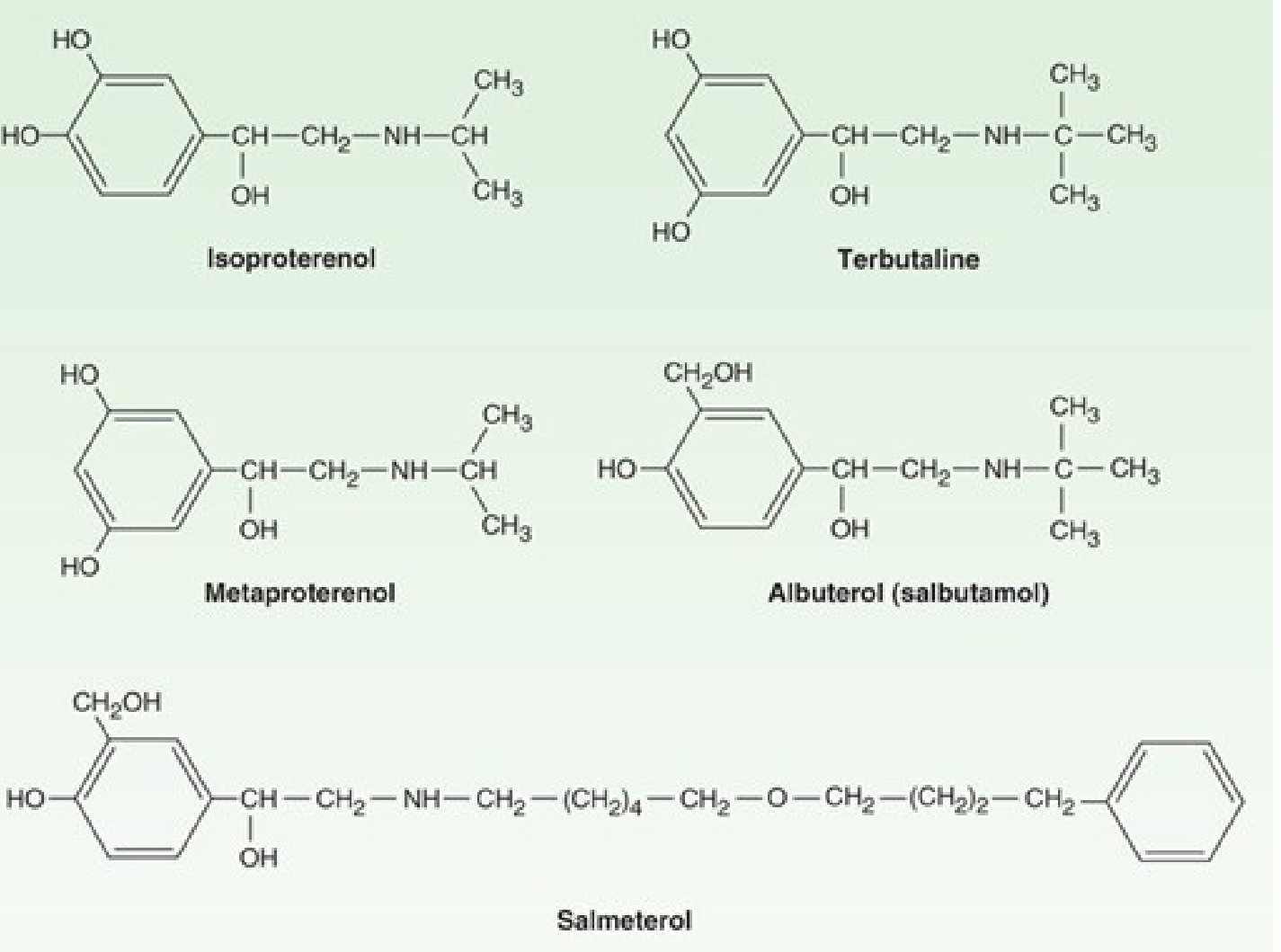
| -CH(CH₃)₂ isopropyl (isoproterenol) | β₁ = β₂ (pure β agonist) |
| Larger bulky groups (terbutaline, albuterol) | β₂ selective |
Key rule: Increasing the size of N-alkyl substituents progressively shifts selectivity from α toward β, and from β₁ toward β₂.
3. Chemical Structures of Key Sympathomimetics
Catecholamines (endogenous):
Non-catecholamine sympathomimetics:
β₂-Selective analogs (for asthma):
4. Synthesis Basics
Epinephrine (Adrenaline) - Biosynthetic pathway (also used in semi-synthesis):
Tyrosine → DOPA → Dopamine → Norepinephrine → Epinephrine
Chemically:
- Start with pyrocatechol (3,4-dihydroxybenzene)
- Condense with chloroacetaldehyde to give the glycol → aminoketone → reduce to give norepinephrine
- N-methylation of norepinephrine (using formaldehyde/reduction or methyl iodide) → epinephrine
Albuterol (Salbutamol) synthesis key point:
- The catechol ring is modified by replacing the 4-OH with a -CH₂OH group (saligenin moiety)
- This resists COMT degradation → longer duration, β₂-selective
Amphetamine from ephedrine:
- Simple dehydroxylation of ephedrine (removal of the β-OH group and the 3,4-ring OH groups)
- This also explains why pseudoephedrine sales are restricted (precursor to methamphetamine)
5. Mechanism of Action & Receptor Selectivity
| Drug | Receptor | Mechanism |
|---|---|---|
| Epinephrine | α₁, α₂, β₁, β₂ | Direct agonist |
| Norepinephrine | α₁, α₂, β₁ | Direct agonist |
| Isoproterenol | β₁ = β₂ | Direct agonist |
| Albuterol/Salbutamol | β₂ selective | Direct agonist |
| Salmeterol | β₂ (long-acting) | Direct agonist |
| Phenylephrine | α₁ selective | Direct agonist |
| Clonidine | α₂ selective | Direct agonist |
| Ephedrine | α + β | Mixed (direct + indirect - releases NE) |
| Amphetamine | α + β | Indirect (releases NE from vesicles) |
| Cocaine | Blocks NE reuptake | Indirect |
6. Therapeutic Uses of Sympathomimetics
| Drug | Use |
|---|---|
| Epinephrine | Anaphylaxis, cardiac arrest, bronchospasm |
| Norepinephrine | Cardiogenic/septic shock (vasopressor) |
| Dopamine | Shock, acute heart failure (dose-dependent: DA₁ at low dose → renal dilation; β₁ at moderate; α₁ at high) |
| Dobutamine | Cardiac inotrope (β₁ selective), heart failure |
| Albuterol/Salbutamol | Bronchodilator - acute asthma (β₂ agonist, inhaled) |
| Salmeterol/Formoterol | Long-acting bronchodilator - COPD/asthma prophylaxis |
| Phenylephrine | Nasal decongestant, mydriasis, BP support |
| Clonidine | Hypertension, ADHD, opioid withdrawal |
| Midodrine | Orthostatic hypotension (prodrug → desglymidodrine) |
| Ephedrine | Nasal decongestant, hypotension under anaesthesia |
| Amphetamine/dextroamphetamine | ADHD, narcolepsy |
PART 2: PARASYMPATHOMIMETIC (CHOLINOMIMETIC) DRUGS
1. Classification
Parasympathomimetics
├── Direct-acting (bind cholinoceptors directly)
│ ├── Choline esters: ACh, Methacholine, Carbachol, Bethanechol
│ └── Alkaloids: Muscarine, Pilocarpine, Nicotine, Lobeline
└── Indirect-acting (AChE inhibitors - increase endogenous ACh)
├── Reversible: Physostigmine, Neostigmine, Pyridostigmine, Edrophonium
└── Irreversible: Organophosphates (echothiophate, sarin, parathion)
2. Chemical Structure of Choline Esters
All choline esters share the quaternary ammonium structure:
- Acetylcholine (ACh): CH₃-CO-O-CH₂-CH₂-N⁺(CH₃)₃
- Acetic acid ester of choline
- Rapidly hydrolyzed by AChE; very short action
- Methacholine: β-methyl group added to choline moiety
- More resistant to AChE hydrolysis
- Selective muscarinic agonist (β-methyl reduces nicotinic activity)
- Carbachol: Carbamic acid ester of choline (replaces acetyl with carbamoyl -NH-CO-)
- Completely resistant to AChE hydrolysis
- Activates both muscarinic and nicotinic receptors
- Bethanechol: Carbamic acid ester of β-methyl choline
- Resistant to hydrolysis + muscarinic selective (β-methyl group)
- Most clinically used choline ester
The muscarinic receptor shows strict stereoselectivity: (S)-bethanechol is ~1000× more potent than (R)-bethanechol.
3. Alkaloids as Parasympathomimetics
| Alkaloid | Source | Main Receptor | Key Feature |
|---|---|---|---|
| Muscarine | Amanita muscaria mushroom | Muscarinic | Prototype; no clinical use |
| Pilocarpine | Pilocarpus jaborandi | Muscarinic (M₃) | Tertiary amine → CNS penetrant; used in glaucoma |
| Nicotine | Tobacco | Nicotinic (NM, NN) | Low dose = stimulate; high dose = depolarizing block |
| Lobeline | Lobelia inflata | Nicotinic | Weak nicotinic agonist |
4. Indirect-Acting Agents: Anticholinesterases
Mechanism: Inhibit acetylcholinesterase (AChE) → ACh accumulates at all cholinergic synapses
Reversible AChE inhibitors:
| Drug | Structure/Type | Duration | Use |
|---|---|---|---|
| Edrophonium | Quaternary; ionic bond only | Very short (5-15 min) | Diagnosis of myasthenia gravis |
| Neostigmine | Quaternary; carbamic ester | Short | Myasthenia gravis, reverse neuromuscular block, postoperative ileus |
| Pyridostigmine | Quaternary; carbamic ester | Medium | Myasthenia gravis (preferred) |
| Physostigmine | Tertiary amine; carbamic ester | Short | Glaucoma, anticholinergic overdose (CNS penetrant) |
| Donepezil/Rivastigmine/Galantamine | Tertiary; CNS-selective | Long | Alzheimer's disease |
Irreversible AChE inhibitors (Organophosphates):
- Echothiophate (ophthalmic - glaucoma)
- Agricultural: Parathion, malathion
- Chemical warfare: Sarin, soman, VX
- Bond covalently to serine -OH of AChE ("aging" makes bond permanent)
- Treated with pralidoxime (2-PAM) if given before aging + atropine
5. Receptor Subtypes Targeted
| Receptor | Location | Effect when activated |
|---|---|---|
| M₁ | Nerves, CNS | IP₃/DAG cascade; gastric acid secretion |
| M₂ | Heart, nerve terminals | ↓ HR, ↓ AV conduction (Gᵢ) |
| M₃ | Glands, smooth muscle, endothelium | Secretion, smooth muscle contraction, NO-mediated vasodilation |
| M₄ | CNS | Inhibition of cAMP |
| Nicotinic (Nm) | Neuromuscular junction | Skeletal muscle contraction |
| Nicotinic (Nn) | Autonomic ganglia, adrenal medulla | Ganglionic transmission |
6. Therapeutic Uses of Parasympathomimetics
| Drug | Use |
|---|---|
| Bethanechol | Urinary retention, postoperative ileus (M₃ agonist) |
| Pilocarpine | Glaucoma (miosis, ↑ trabecular outflow); dry mouth (Sjogren's) |
| Carbachol | Glaucoma (ophthalmic), intraocular surgery (miosis) |
| Echothiophate | Refractory glaucoma (long-acting AChE inhibitor) |
| Neostigmine | Myasthenia gravis; reverse neuromuscular blockade; Ogilvie syndrome |
| Pyridostigmine | Myasthenia gravis (treatment of choice) |
| Edrophonium | Tensilon test for myasthenia gravis diagnosis |
| Physostigmine | Atropine/anticholinergic poisoning antidote |
| Donepezil | Alzheimer's disease (CNS AChE inhibitor) |
| Cevimeline | Sjogren's syndrome (selective M₃ agonist) |
Summary Comparison Table
| Feature | Sympathomimetics | Parasympathomimetics |
|---|---|---|
| Mimics | Sympathetic (adrenergic) NS | Parasympathetic (cholinergic) NS |
| Transmitter mimic | Norepinephrine / Epinephrine | Acetylcholine |
| Receptors targeted | α₁, α₂, β₁, β₂, DA₁, DA₂ | M₁-M₅ (muscarinic), Nm, Nn (nicotinic) |
| Parent structure | Phenylethylamine | Choline ester / Alkaloid |
| Key SAR site | N-substitution (α→β selectivity) | β-methyl reduces nicotinic activity |
| Clinical category | Vasopressors, bronchodilators, decongestants | Glaucoma, myasthenia, Alzheimer's, ileus |
- Katzung's Basic and Clinical Pharmacology, 16th Edition (Chapters 7 & 9)
- Goodman & Gilman's Pharmacological Basis of Therapeutics
- Barash's Clinical Anesthesia, 9th Edition
This is a shared conversation. Sign in to Orris to start your own chat.