Explain concordance and discordance in ecg
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Searching the Web
ECG concordance discordance LBBB Sgarbossa criteria explained
Reading File
Reading File
Loading Image
Loading Image
Here is a thorough explanation of concordance and discordance in ECG, with images directly from the textbooks.
Concordance and Discordance in ECG
Core Definitions
In ECG terminology, these terms describe the directional relationship between the QRS complex and the ST segment/T-wave in a given lead:
| Term | Meaning |
|---|---|
| Discordance | The ST segment/T-wave deflects in the opposite direction to the main QRS complex |
| Concordance | The ST segment/T-wave deflects in the same direction as the main QRS complex |
Why This Matters: The Rule of Appropriate Discordance
In normal depolarization, ventricular repolarization follows a predictable path that is largely opposite to depolarization - hence, the T-wave is normally discordant from the QRS in most leads. This becomes especially important in conditions that distort normal conduction:
- Left Bundle Branch Block (LBBB)
- Ventricular paced rhythms (VPR)
- Left Ventricular Hypertrophy (LVH)
In these conditions, the altered depolarization sequence creates abnormal repolarization. The expected (normal/benign) pattern is appropriate discordance: ST segments and T-waves that deflect opposite to the terminal QRS deflection. This is a secondary ST-T change, not ischemia.
The 5 Patterns in LBBB - Visual Guide
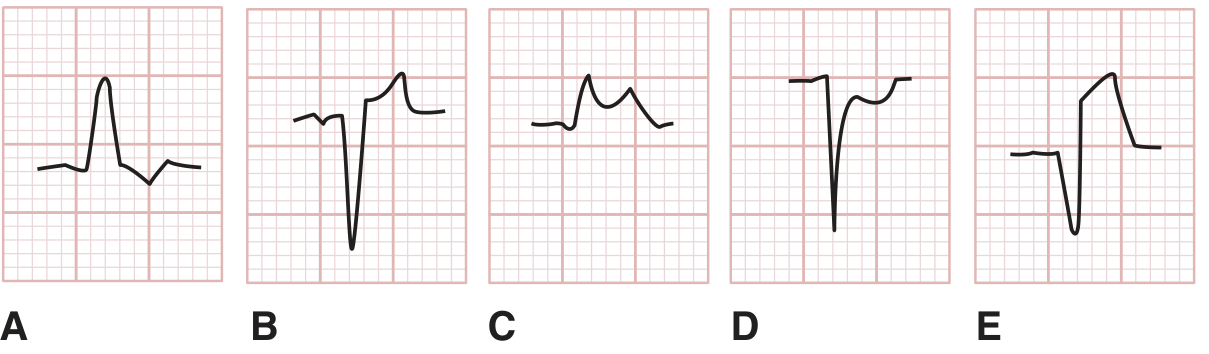
Figure from Tintinalli's Emergency Medicine - A Comprehensive Study
| Panel | Pattern | Interpretation |
|---|---|---|
| A | Upright QRS + ST depression below baseline (opposite direction) | Discordant ST depression - NORMAL in LBBB |
| B | Downgoing (negative) QRS + ST elevation above baseline (opposite direction) | Discordant ST elevation - NORMAL in LBBB |
| C | Upright QRS + ST elevation above baseline (same direction) | Concordant ST elevation - Strongly suggestive of AMI |
| D | Downgoing (negative) QRS + ST depression below baseline (same direction) | Concordant ST depression - Suggestive of AMI |
| E | Downgoing (negative) QRS + ST elevation >5 mm (opposite direction but excessive) | Excessively discordant STE - Weakly suggestive of AMI |
The Sgarbossa Criteria
These criteria, developed by Elena Sgarbossa in 1996, operationalize concordance/discordance to detect acute MI in the setting of LBBB or ventricular paced rhythm (from Rosen's Emergency Medicine):
Original Sgarbossa Criteria (Score-based; total ≥3 = 90% specific for AMI)
| Criterion | Score | Description |
|---|---|---|
| 1 | 5 | Concordant ST elevation ≥ 1 mm in any lead |
| 2 | 3 | Concordant ST depression ≥ 1 mm in V1, V2, or V3 |
| 3 | 2 | Excessively discordant ST elevation > 5 mm in leads with a negative QRS |
- Specificity: ~90% at score ≥3
- Sensitivity: only ~36% (the criteria miss many MIs)
Modified (Smith) Sgarbossa Criteria
The original Criterion 3 (>5 mm absolute) was arbitrary and non-specific - patients with large QRS voltages can easily exceed 5 mm without ischemia. The modified version replaces it with a proportionality rule:
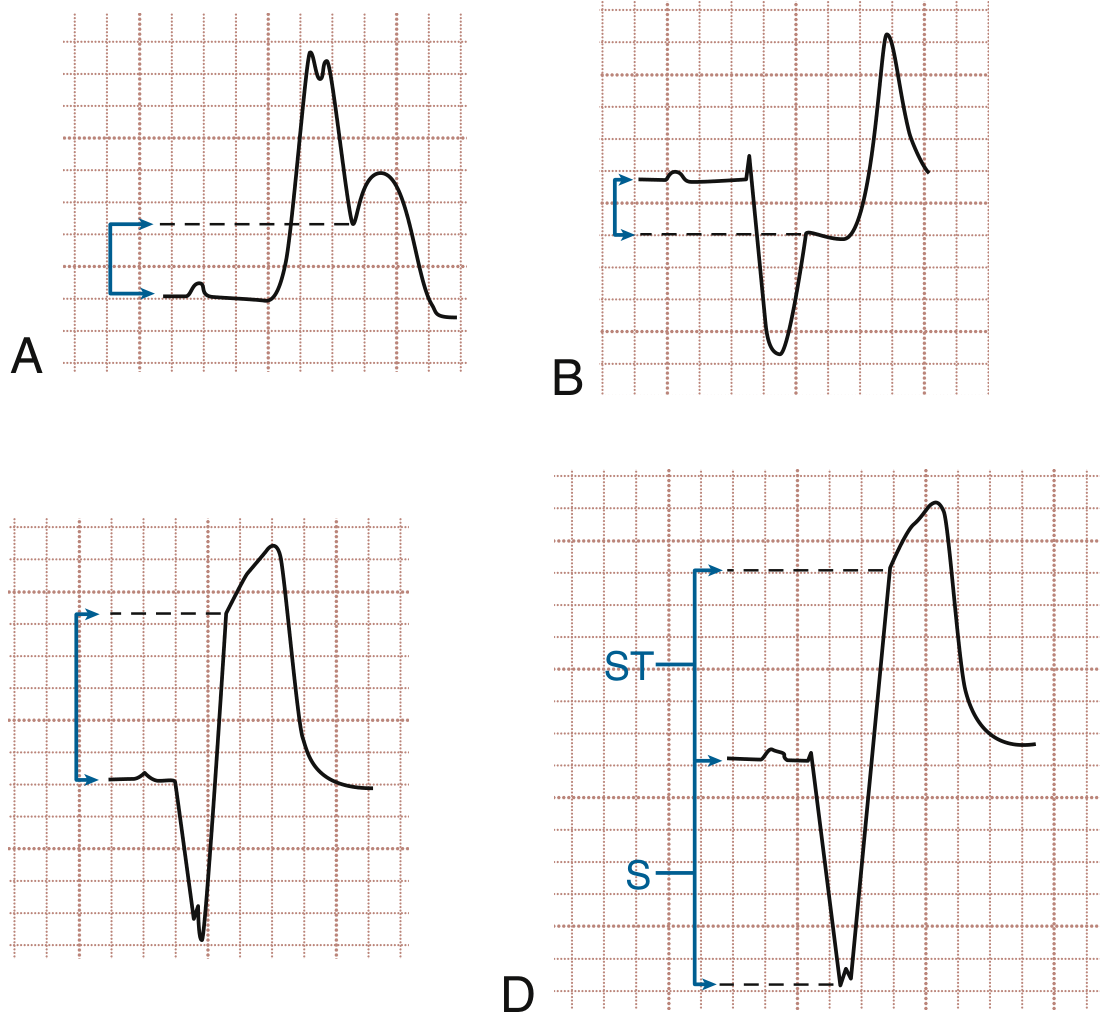
Figure from Rosen's Emergency Medicine - Sgarbossa criteria and ST/S ratio measurement
Modified Criterion 3: ST elevation is excessively discordant if the ST/S ratio > 0.25 (i.e., the ST elevation is more than 25% of the depth of the preceding S-wave).
This modified rule is both more sensitive and more specific than the original.
Concordance in Other Contexts
Precordial Concordance (in wide complex tachycardia)
Concordance also features in differentiating ventricular tachycardia (VT) from SVT with aberrancy:
- Positive concordance: All precordial leads (V1-V6) show upright QRS complexes - strongly suggests VT
- Negative concordance: All precordial leads show negative QRS complexes - strongly suggests VT
If all precordial leads deflect in the same direction (all positive or all negative), this is concordance - an important VT criterion in the Brugada algorithm.
Contiguous Lead Concordance (in STEMI)
The term "contiguous leads" refers to anatomically adjacent leads. ST elevation in contiguous leads (e.g., II, III, aVF for inferior MI) is the standard STEMI criterion - they are "concordant" in showing the same ischemic change.
Summary
| Setting | Discordance = | Concordance = |
|---|---|---|
| LBBB / Paced rhythm | Normal (appropriate secondary change) | Abnormal - suspect AMI |
| Wide complex tachycardia (V1-V6) | Mixed deflections - favors SVT | All leads same direction - favors VT |
| STEMI evaluation | ST changes in non-adjacent leads | ST changes in contiguous leads - diagnostic |
The take-home rule: in LBBB and paced rhythms, concordance is the enemy - it means ischemia is overcoming the expected repolarization pattern and must be taken seriously.
Sources: Tintinalli's Emergency Medicine (9th ed.), Rosen's Emergency Medicine (9th ed.), LITFL Sgarbossa Criteria
Properly explain respiratory breath sounds in all stages of pneumonia
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Searching the Web
breath sounds in stages of lobar pneumonia congestion red hepatization grey hepatization resolution auscultation findings
I now have comprehensive information from multiple authoritative sources. Here is the full explanation:
Respiratory Breath Sounds in All Stages of Pneumonia
Understanding breath sounds in pneumonia requires first understanding the four classic pathological stages of lobar pneumonia, because each stage creates a different physical environment in the alveoli and airways, which directly determines what is heard on auscultation.
Anatomical Basis: Two Patterns of Pneumonia
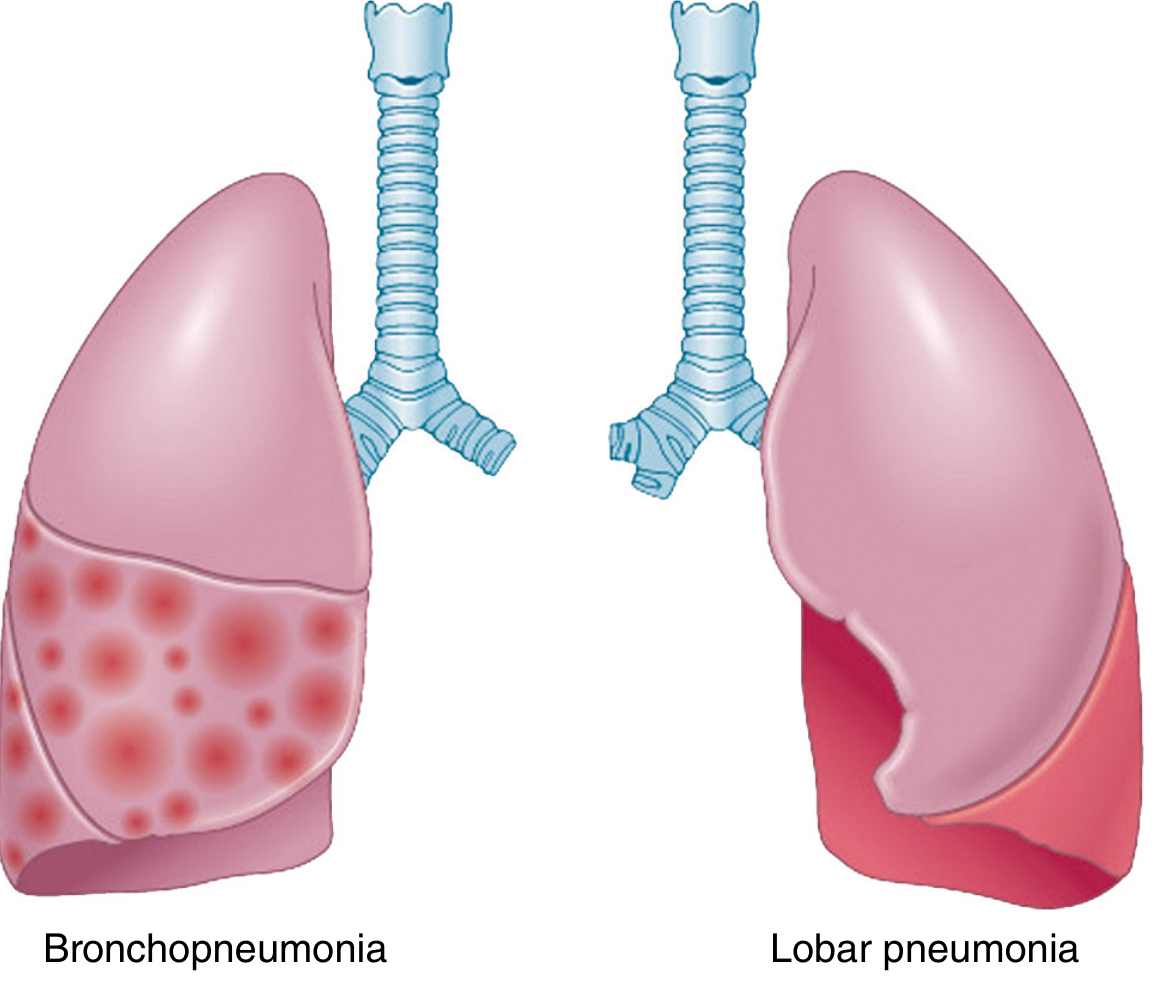
Comparison of bronchopneumonia (patchy, bilateral, multilobar) and lobar pneumonia (entire lobe uniformly consolidated) - Robbins Pathologic Basis of Disease
The stages below describe lobar pneumonia (most often caused by Streptococcus pneumoniae). Bronchopneumonia shows a patchy version of these changes and tends to produce less distinct, more diffuse findings.
The 4 Stages and Their Breath Sounds
Stage 1: Congestion (Days 1-2)
Pathology: The lung is heavy, boggy, and red. There is vascular engorgement and intra-alveolar edema fluid containing a few neutrophils and often numerous bacteria. The alveoli are filling with fluid, but air is still partially present.
Why it affects sounds: Fluid enters the alveoli but they are not yet fully collapsed or airless. As air moves through fluid-filled but partially open alveoli, it produces crackling sounds. The bronchi are still patent and transmit airway sounds reasonably well.
| Finding | Character | Reason |
|---|---|---|
| Breath sounds | Vesicular with decreased intensity, or early bronchial quality beginning | Partial fluid filling, air still present |
| Crackles (rales) | Fine, early inspiratory crackles | Fluid in alveoli - sudden reopening of fluid-coated alveoli during inspiration |
| Tactile fremitus | Slightly increased | Fluid is a better sound conductor than air |
| Percussion | May be normal or slightly dull | Lung not yet fully consolidated |
| Voice sounds | Slightly increased | Early fluid transmission |
| Pleural rub | May be present | Pleuritis if consolidation extends to the pleural surface |
Stage 2: Red Hepatization (Days 2-4)
Pathology: Massive confluent exudation - neutrophils, red blood cells, and fibrin flood the alveolar spaces. The lobe becomes red, firm, and airless with a liver-like consistency (hence "hepatization"). This is the peak of consolidation.
Why it affects sounds: The alveoli are now completely airless and solidified with exudate. Solid lung tissue transmits high-frequency sounds from the large airways directly to the chest wall - this is the basis of bronchial breathing in consolidation. The "air-cushion" effect of normal alveoli that normally filters and softens large-airway sounds is lost.
| Finding | Character | Reason |
|---|---|---|
| Breath sounds | Bronchial (tubular) breathing - loud, high-pitched, with equal inspiratory and expiratory phases, and a gap between them | Airless consolidated lung transmits bronchial sounds from major airways directly to chest wall |
| Crackles | Coarse crackles, may diminish as alveoli become fully consolidated | Less air-fluid interface as alveoli become completely solidified |
| Tactile fremitus | Markedly increased | Dense solid tissue is an excellent sound conductor |
| Percussion | Stony dull | Consolidated, airless lobe |
| Egophony (E to A change) | Present - patient says "EEE," clinician hears "AY" | Abnormal sound filtering through consolidated parenchyma - as Harrison's states, this strongly suggests lobar consolidation |
| Whispered pectoriloquy | Present - whispered sounds clearly audible | Sound conducted through solid medium |
| Bronchophony | Present - "99" sounds louder and clearer than normal | Enhanced transmission through consolidated lung |
| Pleural friction rub | May persist | Fibrinous pleuritis |
Key teaching point: Bronchial breathing over a peripheral lung zone (where vesicular sounds are expected) is a cardinal sign of lobar consolidation. According to Goldman-Cecil Medicine: "Bronchial breath sounds and egophony strongly suggest pneumonia with lobar consolidations."
Stage 3: Grey Hepatization (Days 4-8)
Pathology: Red blood cells disintegrate and are lysed. Neutrophils persist and fibrin remains, but the exudate becomes fibrinopurulent. The lobe becomes grey-brown and drier. Bacteria begin disappearing as the infection is contained - this stage corresponds with successful containment and begins the transition to recovery (as described in Harrison's Principles).
Why it affects sounds: The lung tissue remains consolidated but the exudate is beginning to change its consistency. Sounds remain similar to red hepatization, but may begin very subtly transitioning. Clinically, this stage is often difficult to distinguish from red hepatization by auscultation alone.
| Finding | Character | Reason |
|---|---|---|
| Breath sounds | Bronchial breathing persists, may begin to soften slightly | Consolidation still present but beginning to loosen |
| Crackles | May re-emerge as dry, coarse crackles | Alveolar exudate beginning to break down and become less homogeneous |
| Tactile fremitus | Still increased but may begin to decrease | Exudate drying out, slightly less homogeneous |
| Percussion | Still dull | Consolidation still present |
| Egophony/Whispered pectoriloquy | Persist | Lung still solidified |
Stage 4: Resolution (Days 8 onward)
Pathology: Enzymatic digestion breaks down the exudate into granular, semifluid debris. Macrophages return as the dominant cell and clear the debris. Material is resorbed, ingested by macrophages, or expectorated. Alveoli gradually re-aerate. The lung begins returning to normal.
Why it affects sounds: As fluid and debris are cleared, alveoli are partially re-filled with air but contain residual secretions. The air-fluid interface returns, generating crackles again - this time on resolution rather than on accumulation. Bronchial sounds gradually give way to normal vesicular sounds as alveoli re-expand.
| Finding | Character | Reason |
|---|---|---|
| Breath sounds | Transition from bronchial back to vesicular; "vesiculobronchial" mixed quality during transition | Progressive re-aeration of alveoli |
| Crackles | Re-emergence of fine to medium crackles (resolution crackles / "crepitations") | Reopening of secretion-coated alveoli during inspiration |
| Tactile fremitus | Decreasing toward normal | Less solid medium |
| Percussion | Improving from dull toward resonant | Re-aeration |
| Egophony/Whispered pectoriloquy | Fading and resolving | Less consolidation |
| Rhonchi | May appear | Secretions in medium airways being mobilized and expectorated |
Summary Table: Breath Sounds Across All Stages
| Feature | Stage 1: Congestion | Stage 2: Red Hepatization | Stage 3: Grey Hepatization | Stage 4: Resolution |
|---|---|---|---|---|
| Breath sounds | Vesicular (decreased) | Bronchial (tubular) | Bronchial (persisting) | Vesiculobronchial → Vesicular |
| Crackles | Fine early inspiratory | Coarse or diminished | Coarse | Medium-coarse (resolution crackles) |
| Percussion | Normal to slightly dull | Stony dull | Dull | Improving toward resonant |
| Tactile fremitus | Slightly increased | Markedly increased | Still increased | Decreasing |
| Egophony | Absent | Present | Present | Fading |
| Whispered pectoriloquy | Absent | Present | Present | Fading |
| Bronchophony | Absent | Present | Present | Fading |
| Pleural rub | Possible | Possible | Rare | Absent |
Why Bronchial Breathing Occurs in Consolidation - The Mechanism
Normal vesicular breathing is produced in peripheral lung tissue where air movement into millions of alveoli creates a soft, low-pitched rustling sound. This "cushions" and filters the louder bronchial sounds from central airways.
In consolidation, alveoli fill with solid exudate. The alveolar air cushion disappears. Large-airway bronchial sounds now travel through a solid, non-filtering medium directly to the chest wall - just like sound travels better through solid material than through air. The result is bronchial breathing heard peripherally where it does not normally belong.
Murray & Nadel's Textbook of Respiratory Medicine summarizes the consolidated lung findings as:
- Inspection: Possible lag or splinting on the affected side
- Palpation: Increased fremitus on affected side
- Percussion: Dullness
- Auscultation: Bronchial breath sounds; bronchophony, pectoriloquy, crackles
Important Clinical Notes
-
These "textbook" stages may not always be distinct in practice. As Harrison's notes, the stages may overlap, and modern antibiotic treatment often interrupts progression. A 2021 PMC study found that in most patients, different histological stages co-exist within the same lobe simultaneously, rather than following a strict sequential course.
-
Atypical (walking) pneumonia (caused by Mycoplasma, Legionella, viruses) tends to produce an interstitial rather than lobar pattern - findings are often subtle with fine bilateral crackles and no bronchial breathing, because true alveolar consolidation is less prominent.
-
Absence of findings does not exclude pneumonia. As Goldman-Cecil states: "none of these findings on physical examination is sufficiently sensitive or specific to avoid the need for imaging for radiographic validation."
-
A pleural friction rub (a leathery, creaking sound in early inspiration and expiration) may occur in early stages when fibrinous pleuritis develops at the lung surface and is a useful indicator of pleural involvement.
Sources: Robbins Pathologic Basis of Disease (10th ed.), Harrison's Principles of Internal Medicine (22nd ed., 2025), Goldman-Cecil Medicine, Murray & Nadel's Textbook of Respiratory Medicine, Frameworks for Internal Medicine
Compare breath sounds of lobar vs bronchopneumonia
Finding Sources
Finding Sources
Searching the Web
lobar pneumonia vs bronchopneumonia breath sounds auscultation differences clinical comparison
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
All needed information is now assembled. Here is the detailed comparison:
Breath Sounds: Lobar Pneumonia vs Bronchopneumonia
The Fundamental Anatomical Difference
Everything about the clinical and auscultatory differences between these two types flows from one core pathological fact:
| Lobar Pneumonia | Bronchopneumonia | |
|---|---|---|
| Pattern | Uniform, continuous consolidation of an entire lobe (or large segment) | Patchy, multifocal consolidation around bronchi and bronchioles |
| Distribution | Localized to one lobe - affects one region of the chest | Multilobar, bilateral, predominantly basal |
| Air content | Entire lobe becomes completely airless at peak | Islands of normal aerated lung remain between consolidated patches |
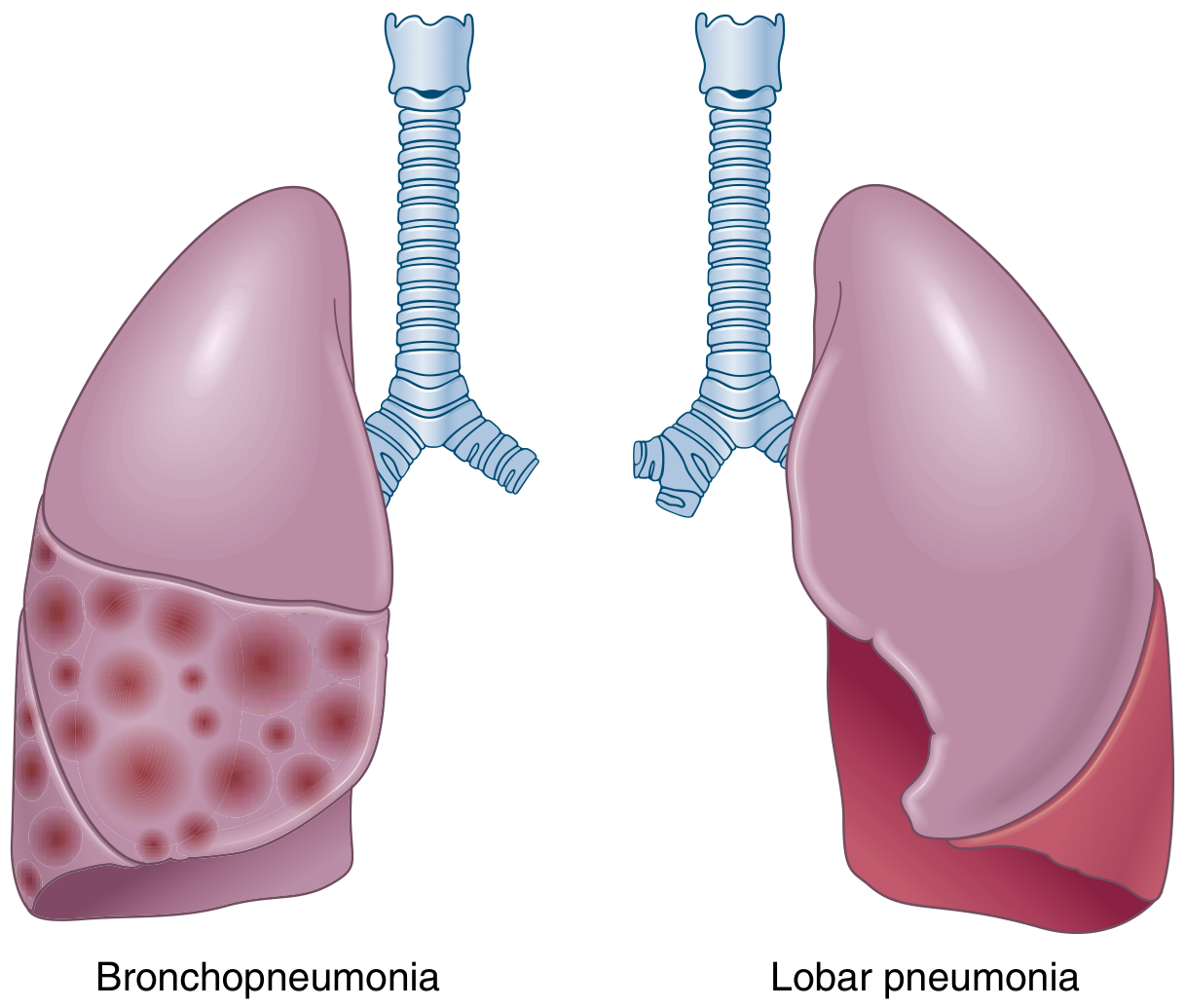
FIG. 11.29 - Robbins & Kumar Basic Pathology: Anatomic distribution of bronchopneumonia (patchy, scattered foci) and lobar pneumonia (entire lower lobe uniformly consolidated)
Gross Pathology - What Creates the Sounds
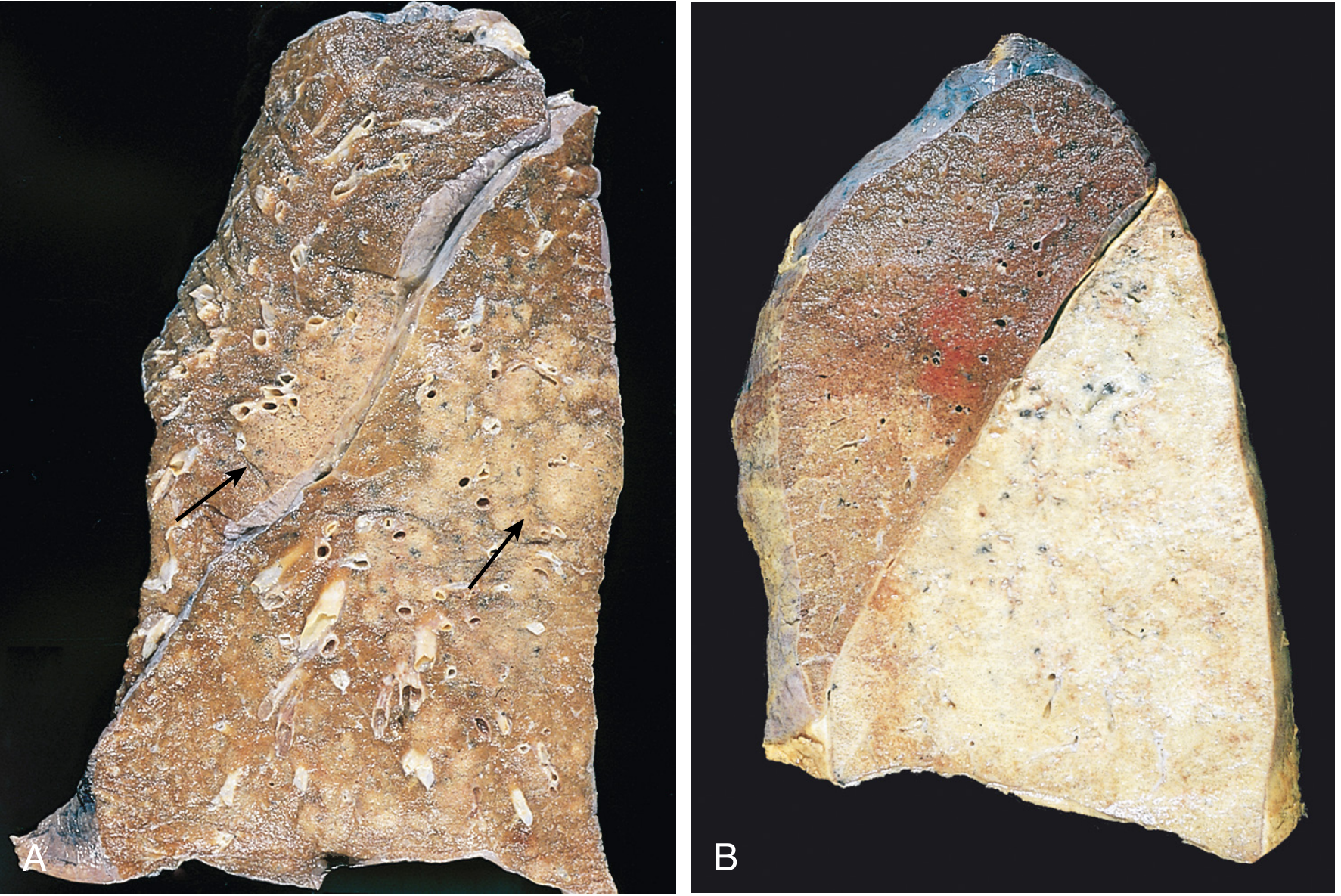
A: Bronchopneumonia - patches of consolidation (arrows) amid normal lung tissue. B: Lobar pneumonia (grey hepatization) - the entire lower lobe is uniformly, solidly consolidated. - Robbins Pathologic Basis of Disease
In bronchopneumonia (panel A), patches of consolidated lung are surrounded by still-aerated alveoli. In lobar pneumonia (panel B), the entire lobe is a single, homogeneous solid block with no residual air cushion.
Auscultation Comparison - All Findings
1. Breath Sounds (Primary Finding)
| Feature | Lobar Pneumonia | Bronchopneumonia |
|---|---|---|
| Type | Bronchial (tubular) breathing over the affected lobe | Diminished vesicular with no bronchial quality |
| Character | Loud, high-pitched, hollow/tubular; expiration = inspiration in intensity, with a gap | Soft, muffled vesicular sounds, reduced in intensity |
| Why | Entire lobe is airless solid - acts as a perfect conductor of large-airway bronchial sounds to chest wall | Patches of consolidation are small and surrounded by aerated lung which continues to dampen and filter sounds; no single large solid medium for sound conduction |
| Location | Clearly localized to one anatomical region (e.g., right lower lobe posteriorly) | Diffuse, bilateral, predominantly lower zones - no clear localization |
Key principle: Bronchial breathing requires a large, contiguous block of consolidated lung touching the chest wall to act as a sound conductor. In bronchopneumonia the patches are too small and scattered to produce this effect. Air in the surrounding alveoli continues to attenuate the sound.
2. Crackles (Adventitious Sounds)
| Feature | Lobar Pneumonia | Bronchopneumonia |
|---|---|---|
| Type | Fine-to-medium inspiratory crackles (early/late); may diminish at full consolidation | Coarse, medium inspiratory crackles - prominent throughout |
| Distribution | Localized to the affected lobe | Bilateral, diffuse, predominantly bibasilar |
| Character | At peak consolidation (red hepatization), crackles may become less prominent as alveoli are fully filled | Always present - more consistently heard because many alveoli are at the air-fluid boundary (partially consolidated) at all times |
| Why | At full consolidation, all alveoli are solid - no air-fluid interface to generate crackles; re-emerge in resolution | Patchy disease means there are always partially-filled alveoli collapsing on expiration and snapping open on inspiration |
3. Percussion Note
| Feature | Lobar Pneumonia | Bronchopneumonia |
|---|---|---|
| Note | Stony dull - over the entire consolidated lobe | Variable dullness - patchy areas of dullness interspersed with normal resonance |
| Distribution | Maps clearly to anatomical lobe borders | Patchy, bilateral lower zones, no sharp border |
| Reliability | High - large area gives consistent dullness | Lower - patchiness means percussion can be surprisingly normal in some areas |
4. Tactile Fremitus
| Feature | Lobar Pneumonia | Bronchopneumonia |
|---|---|---|
| Finding | Markedly increased over the consolidated lobe | Mildly or variably increased - inconsistent |
| Why | Solid, homogeneous medium transmits vibration from spoken voice powerfully | Patchy consolidation with adjacent normal lung; no uniform conductor |
5. Vocal Resonance Signs
| Sign | Lobar Pneumonia | Bronchopneumonia |
|---|---|---|
| Egophony (E→A change) | Present - characteristic sign of lobar consolidation | Usually absent or weakly present |
| Whispered pectoriloquy | Present - whispered words clearly audible | Absent |
| Bronchophony | Present - "99" sounds louder, clearer | Absent or inconsistent |
| Why the difference | Requires a large continuous solid medium to amplify and transmit vocal sounds unchanged from bronchi to chest wall | Small patches cannot generate this consistent amplification |
As Goldman-Cecil Medicine states: "Bronchial breath sounds and egophony strongly suggest pneumonia with lobar consolidations but often are not heard" - and are essentially absent in bronchopneumonia.
6. Additional Findings
| Finding | Lobar Pneumonia | Bronchopneumonia |
|---|---|---|
| Pleural friction rub | May be present - fibrinous pleuritis when consolidation reaches pleural surface | Usually absent |
| Rhonchi | May occur in early/late stages when secretions are mobile | Prominent - because the process starts in bronchi/bronchioles, secretions in medium airways produce rhonchi |
| Wheeze | Rare | May occur if peribronchial inflammation causes airway narrowing |
| Breath sound location | One side, one lobe - localizable | Both sides, lower zones - diffuse |
Complete Comparison Summary
| Physical Sign | Lobar Pneumonia | Bronchopneumonia |
|---|---|---|
| Breath sounds | Bronchial (tubular), localized | Diminished vesicular, diffuse bilateral |
| Crackles | Fine early; absent at peak consolidation; coarse at resolution | Coarse, persistent, bilateral basal |
| Rhonchi | Uncommon | Common (airway-centred disease) |
| Percussion | Stony dull over entire lobe | Patchy dullness bilaterally |
| Tactile fremitus | Markedly increased | Mildly/variably increased |
| Egophony | Present | Absent |
| Whispered pectoriloquy | Present | Absent |
| Bronchophony | Present | Absent |
| Pleural rub | Possible | Absent |
| Laterality | Unilateral, lobar | Bilateral, basal |
| Localization | Sharp, maps to lobe | Diffuse, no sharp border |
Why This Matters Clinically
- A patient with classic lobar consolidation signs (bronchial breathing + egophony + increased fremitus + stony dullness) almost certainly has bacterial lobar pneumonia (classically Streptococcus pneumoniae).
- A patient with bilateral coarse crackles + rhonchi + patchy dullness without bronchial breathing or egophony likely has bronchopneumonia (common in elderly, post-viral, aspiration, hospital-acquired, Staphylococcus, gram-negatives).
- Bronchopneumonia is more common than classic lobar pneumonia in modern clinical practice - many textbook "lobar" findings are now rarely seen because antibiotic treatment interrupts progression before full consolidation develops.
Sources: Robbins Pathologic Basis of Disease (10th ed.), Robbins & Kumar Basic Pathology (11th ed.), Goldman-Cecil Medicine, Murray & Nadel's Textbook of Respiratory Medicine, Harrison's Principles of Internal Medicine (22nd ed.)
This is a shared conversation. Sign in to Orris to start your own chat.