Thyroid profile
Reading File
Finding Sources
Finding Sources
Searching the Web
thyroid profile tests TSH T3 T4 normal values interpretation 2024
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Excellent - I now have comprehensive data from multiple authoritative textbooks. Here is the full thyroid profile overview:
Thyroid Profile
The thyroid profile (thyroid function tests) is a panel of blood tests used to evaluate the function of the thyroid gland. It typically includes TSH, free T4, free T3, and sometimes total T4/T3 and antibodies.
Hypothalamic-Pituitary-Thyroid (HPT) Axis
The HPT axis is the regulatory backbone of thyroid function:
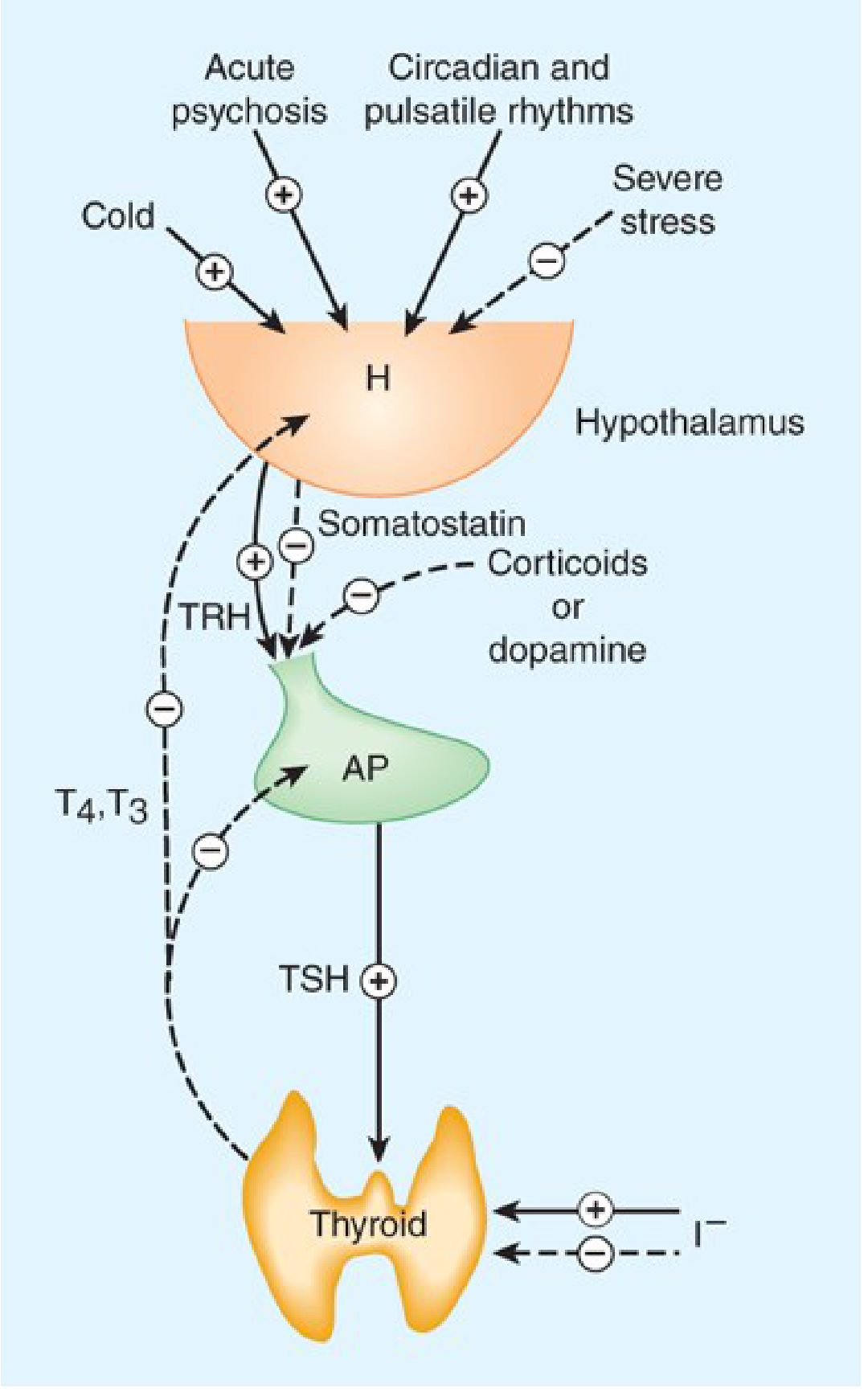
- Hypothalamus secretes TRH (thyrotropin-releasing hormone)
- TRH stimulates the anterior pituitary to release TSH (thyroid-stimulating hormone)
- TSH stimulates the thyroid gland to synthesize and release T3 and T4
- T3/T4 exert negative feedback on both the pituitary (suppressing TSH) and the hypothalamus (suppressing TRH)
- External factors: Cold and acute psychosis stimulate the axis; severe stress and corticoids/dopamine inhibit it
(Katzung's Basic and Clinical Pharmacology, 16th Ed)
The Tests - Normal Reference Ranges
| Test | Normal Value | Hypothyroidism | Hyperthyroidism |
|---|---|---|---|
| Total T4 | 4.8-10.4 mcg/dL (62-134 nmol/L) | Low | High |
| Total T3 | 59-156 ng/dL (0.9-2.4 nmol/L) | Normal or Low | High |
| Free T4 (FT4) | 0.8-1.4 ng/dL (10-18 pmol/L) | Low | High |
| Free T3 (FT3) | 169-371 ng/dL (2.6-5.7 pmol/L) | Low | High |
| TSH | 0.45-4.12 µIU/mL | High | Low |
| 123I uptake (24h) | 5-35% | Low | High |
| Anti-Tg antibodies | <200 IU/mL | Often present | Usually present |
| Anti-TPO antibodies (ATPO) | ≤100 WHO units | Often present | Usually present |
| Serum thyroglobulin | Women: 1.5-38.5 mcg/L; Men: 1.4-29.2 mcg/L | Not indicated | Not indicated |
| TSI / TSH-R Ab | Negative (<140% of baseline) | Not indicated | Elevated in Graves' disease |
(Katzung's Basic and Clinical Pharmacology, 16th Ed, p. 1077)
Individual Tests Explained
1. TSH (Thyroid-Stimulating Hormone)
- The single most sensitive screening test for thyroid dysfunction
- If TSH is normal, thyroid function is almost certainly normal
- TSH is the first test to change in thyroid disease:
- High TSH = Primary hypothyroidism (thyroid under-producing, pituitary compensating)
- Low TSH = Hyperthyroidism or secondary/tertiary hypothyroidism
- Reference: 0.45-4.12 µIU/mL (adults)
- Pregnancy-specific ranges: 1st trimester 0.26-2.66; 2nd trimester 0.55-2.73; 3rd trimester 0.43-2.91 mIU/L
2. Free T4 (FT4) - Preferred over Total T4
- Biologically active, unbound fraction of thyroxine
- Not affected by changes in thyroid-binding globulin (TBG) unlike total T4
- Total T4 is seldom measured nowadays - FT4 has largely replaced it
- Reference: 0.8-1.4 ng/dL
3. Free T3 (FT3)
- Active form; T4 is converted to T3 peripherally by deiodinases
- More useful than total T3 in clinical practice
- Helpful in T3 toxicosis (elevated T3 with normal T4)
- Reference: 2.0-4.4 pg/mL
4. Total T4 and Total T3
- Include both protein-bound and free fractions
- Can be falsely elevated or depressed by changes in TBG (e.g., estrogen raises TBG, androgens lower TBG) without actual thyroid disease
- Seldom used clinically now that free hormone assays are available
(Harper's Illustrated Biochemistry, 32nd Ed)
Interpreting the Pattern
| TSH | FT4 | FT3 | Interpretation |
|---|---|---|---|
| High | Low | Low | Primary hypothyroidism |
| Low | High | High | Primary hyperthyroidism |
| Low/normal | Low | Low | Secondary (pituitary) or tertiary (hypothalamic) hypothyroidism |
| Low | Normal | Normal | Subclinical hyperthyroidism |
| High | Normal | Normal | Subclinical hypothyroidism |
| Normal | Low (total only) | - | Low TBG state (androgens, nephrotic syndrome) |
| Normal | High (total only) | - | High TBG state (estrogens, pregnancy, OCP) |
Thyroid Antibodies
| Antibody | Significance |
|---|---|
| Anti-TPO (thyroid peroxidase) | Hashimoto's thyroiditis, Graves' disease; ≤100 WHO units normal |
| Anti-thyroglobulin (Anti-Tg) | Hashimoto's, thyroid cancer monitoring; <200 IU/mL normal |
| TSH receptor antibody (TSI / TRAb) | Specific for Graves' disease; causes hyperthyroidism by mimicking TSH |
Drug Effects on Thyroid Tests
Drugs can cause both in vitro and in vivo effects - this is a common source of misinterpretation (Henry's Clinical Diagnosis and Management by Laboratory Methods; Washington Manual of Medical Therapeutics):
Drugs causing decreased T4/T3 (true hypothyroidism - TSH elevated):
- Iodine (amiodarone, radiographic contrast), lithium, some tyrosine kinase inhibitors, immune checkpoint inhibitors
Drugs suppressing TSH without true hypothyroidism:
- Glucocorticoids (high dose), dopamine - suppress TSH secretion
Drugs affecting TBG (TSH remains normal):
- Increase TBG (raise total T4/T3 but not free): Estrogens, tamoxifen, raloxifene, methadone, heroin, SERMs
- Decrease TBG (lower total T4/T3 but not free): Androgens
Drugs displacing T4 from binding proteins (TSH normal):
- Furosemide (high dose), salicylates, phenytoin, carbamazepine
Drugs inhibiting T4 → T3 conversion:
- Amiodarone (complex effects - can cause hypo- or hyperthyroidism), glucocorticoids, high-dose propranolol (useful in thyroid storm)
Drugs causing lab artifact only:
- Biotin - interferes with immunoassays, causing false results without real thyroid dysfunction
Key Clinical Points
- Start with TSH - it is the most sensitive marker and often sufficient for screening
- Use FT4 (not total T4) for confirming thyroid hormone levels
- Add FT3 when T3 toxicosis is suspected or when monitoring hyperthyroidism treatment
- TSI/TRAb confirms Graves' disease
- Anti-TPO is the best antibody for diagnosing Hashimoto's thyroiditis
- Thyroglobulin is used as a tumor marker after thyroidectomy for differentiated thyroid cancer
- Always check the medication list before interpreting any thyroid test - many common drugs interfere
Sources: Katzung's Basic and Clinical Pharmacology, 16th Ed | Harper's Illustrated Biochemistry, 32nd Ed | Henry's Clinical Diagnosis and Management by Laboratory Methods | Washington Manual of Medical Therapeutics | Goodman & Gilman's Pharmacological Basis of Therapeutics
This is a shared conversation. Sign in to Orris to start your own chat.