
6afbc0b2-0e25-4d4a-b161-ee8bfa2e647a.jpeg
Provide a detailed explanation of the topics in image for mbbs 1st tear student
analyse_media
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Loading Image
I have all the material I need. Here is the full, detailed explanation of all four chapters from Unit XII - The Integrated Physiology for MBBS 1st year students.
Unit XII: The Integrated Physiology
MBBS 1st Year - Complete Chapter Notes
Chapter 102: Regulation of Body Temperature in Humans
Normal Body Temperature
The body maintains two distinct temperature zones:
- Core temperature (deep tissues): highly regulated, normally 97°F - 99.5°F (36°C - 37.5°C). This remains stable within ±0.6°C in health.
- Skin (shell) temperature: fluctuates freely with the environment, and is important for heat exchange.
The average normal oral temperature is 98.0-98.6°F (37°C); rectal temperature is ~1°F higher.
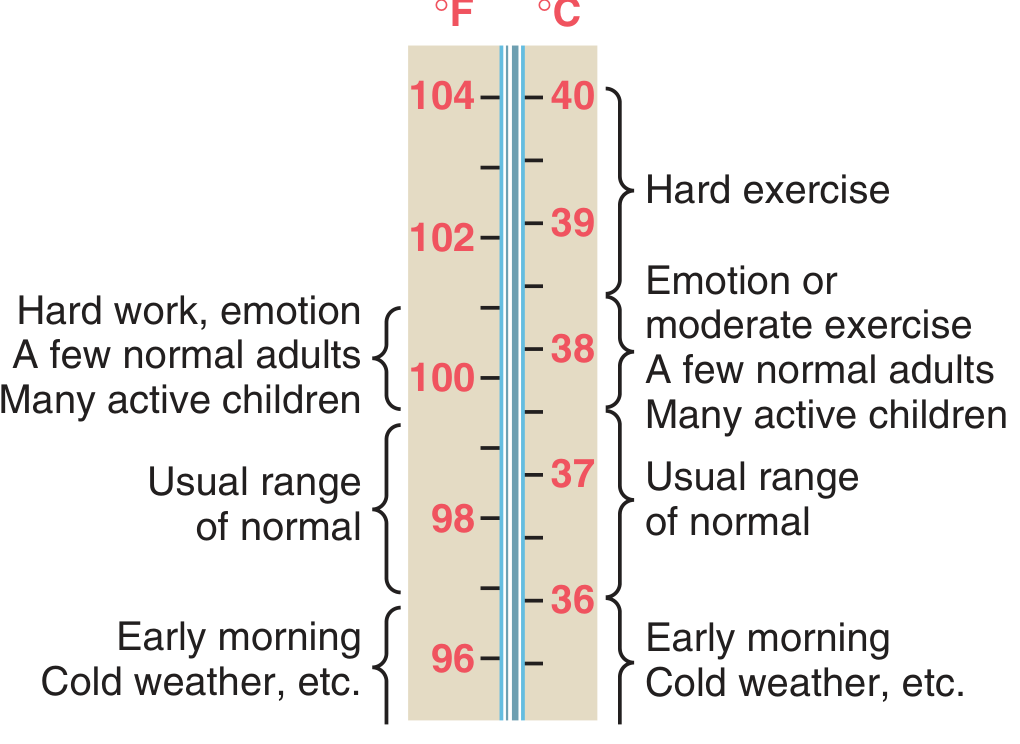
Figure: Estimated normal range of body core temperatures under various conditions - Guyton & Hall, p. 897
Core temperature can transiently rise to 101-104°F during strenuous exercise or fall below 96°F in extreme cold.
Factors Affecting Body Temperature
Heat production in the body depends on:
- Basal metabolic rate (BMR) of all cells
- Muscle activity - exercise and shivering are major sources
- Thyroid hormones (thyroxine) - increase cellular metabolism
- Epinephrine/norepinephrine and sympathetic stimulation
- Cell temperature - higher temperature accelerates chemical reactions
- Thermogenic (specific dynamic) effect of food - digestion generates heat
Other factors affecting body temperature include: time of day (lowest at 6 AM, highest at 6 PM - diurnal variation), age (higher in children, lower in elderly), exercise, emotions, and environmental temperature.
Temperature Regulating Mechanisms
The body maintains thermal balance by balancing heat production vs. heat loss:
"When the rate of heat production in the body is greater than the rate at which heat is being lost, heat builds up in the body, and the body temperature rises. Conversely, when heat loss is greater than heat production, body temperature decreases." - Guyton & Hall
The Hypothalamic Thermostat:
- The anterior hypothalamus is the body's thermoregulatory center (the "thermostat")
- It receives input from:
- Peripheral thermoreceptors in the skin (warm & cold receptors)
- Central thermoreceptors in the anterior hypothalamus itself monitoring blood/core temperature
- The hypothalamus compares sensed temperature against a set-point (~37°C) and activates corrective responses
Heat-Generating Mechanisms (when core temperature falls below set-point):
- Shivering - rapid involuntary muscle contractions generate heat
- Vasoconstriction of skin blood vessels (sympathetic tone increase) - reduces heat loss from skin
- Increased metabolic rate via thyroid hormones
- Piloerection (goosebumps) - traps insulating air layer
Heat-Dissipating Mechanisms (when core temperature rises above set-point):
- Sweating - evaporation is the most powerful heat loss mechanism
- Vasodilation of skin vessels (reduced sympathetic tone) - brings warm blood to skin surface for radiation, conduction, convection
- Increased respiration (minor effect in humans; major in panting animals)
Routes of Heat Loss:
| Method | Mechanism |
|---|---|
| Radiation | Infrared waves from skin (~60% at rest) |
| Conduction | Direct contact with cooler objects |
| Convection | Air currents carry heat away |
| Evaporation | Sweat evaporation (~22% at rest, dominant during exercise) |
Applied Aspects
Fever:
- Defined as core temperature above normal due to resetting of the hypothalamic set-point upward by pyrogens
- Pyrogens (e.g., bacterial lipopolysaccharide endotoxins) stimulate macrophages to release cytokines, especially Interleukin-1 (IL-1), which is also called endogenous pyrogen
- IL-1 acts on the anterior hypothalamus to increase local prostaglandin synthesis, which raises the set-point
- The body then activates heat-generating mechanisms (shivering, vasoconstriction) until the new, higher set-point is reached - this is the "chills" phase
- Aspirin reduces fever by inhibiting cyclooxygenase (COX), blocking prostaglandin synthesis - this lowers the set-point back to normal, triggering heat-loss mechanisms (sweating, vasodilation) - Costanzo Physiology 7th Ed., p. (block2)
Hypothermia:
- Core temperature below 35°C
- At <32°C: loss of shivering (heat production fails), cardiac arrhythmias risk
- At <20°C: potentially fatal
- Causes: exposure to extreme cold, immersion in cold water, anesthesia
Heat Stroke:
- Occurs when core temperature rises to levels causing tissue damage, due to failure of heat-dissipating mechanisms
- If sweating fails, heat cannot be released and temperature rises uncontrolled
- Medical emergency requiring rapid cooling
Malignant Hyperthermia:
- A rare but life-threatening condition triggered by certain inhalation anesthetics in susceptible individuals
- Causes massive increase in skeletal muscle metabolic rate, extreme heat production that overwhelms dissipating mechanisms
Cold Injuries:
- Frostnip - mild, reversible freezing of superficial skin
- Frostbite - ice crystal formation in tissues causing cell damage and vascular injury
Chapter 103: Physiology of Exercise
Grading of Exercise
Exercise intensity is classified using MET (Metabolic Equivalent of Task) values or VO₂max percentage:
- Light exercise: <3 METs (e.g., slow walking)
- Moderate exercise: 3-6 METs (e.g., brisk walking, cycling)
- Vigorous/Hard exercise: >6 METs (e.g., running, sports)
The motor unit is the fundamental functional unit - it consists of one motor neuron and all muscle fibers it innervates. Motor units are recruited progressively:
- Type I (slow-twitch) fibers - recruited first, high oxidative capacity, fatigue-resistant - used for sustained activities
- Type IIa (fast-twitch oxidative) - intermediate
- Type IIx (fast-twitch glycolytic) - recruited last, powerful but fatigue quickly
"Physical exercise is often the greatest stress that the body encounters in the course of daily life... the body must make rapid, integrated adjustments at the level of cells and organ systems." - Medical Physiology (Boron & Boulpaep)
Skeletal muscle converts only ~25% of stored chemical energy into mechanical work; the remaining ~75% appears as heat - which is why exercise raises body temperature and demands active thermoregulation.
Cardio-respiratory Adaptation to Exercise
Immediate (Acute) Cardiovascular Responses:
- Heart rate (HR) increases - due to withdrawal of vagal tone and increased sympathetic activity
- Stroke volume increases - due to increased venous return (Frank-Starling mechanism) and sympathetic stimulation of the heart
- Cardiac output (CO = HR × SV) can increase from 5 L/min at rest to 20-25 L/min during maximal exercise
- Blood pressure rises - systolic increases more than diastolic
- Vasodilation in active muscles (due to local metabolites: CO₂, H⁺, adenosine, K⁺) and vasoconstriction in visceral organs - blood is redirected to muscles
Immediate Respiratory Responses:
- Respiratory rate and tidal volume both increase
- Minute ventilation can rise from 5-6 L/min at rest to >100 L/min during maximal exercise
- Increased ventilation matches increased CO₂ production and O₂ demand
- Ventilatory threshold (anaerobic threshold): point at which lactic acid accumulates faster than it can be cleared; ventilation rises disproportionately to clear excess CO₂ from lactate buffering
Long-term (Chronic) Adaptations with Training:
| Parameter | Trained Effect |
|---|---|
| Resting HR | Decreases (athlete's bradycardia - HR may be 40-50 bpm) |
| Heart size | Cardiac hypertrophy (especially left ventricle) |
| Stroke volume | Increases at rest and during exercise |
| VO₂max | Increases (best measure of cardiovascular fitness) |
| Muscle capillary density | Increases |
| Mitochondria in muscle | Increase in number and size |
| Oxidative enzyme activity | Increases in skeletal muscle |
Physiological Effects of Physical Training
Systematic physical training produces beneficial adaptations across multiple systems:
- Musculoskeletal: increased muscle strength, bone density, joint flexibility
- Cardiovascular: lower resting HR, larger stroke volume, reduced cardiovascular disease risk
- Metabolic: improved insulin sensitivity, better glucose and lipid metabolism, increased fat oxidation
- Respiratory: improved efficiency, larger vital capacity
- Psychological: reduced anxiety and depression, improved mood (endorphin release)
Exercise under Heat and Cold
Exercise in Heat:
- Competing demands between muscles (needing blood flow) and skin (needing blood flow for cooling) create cardiovascular strain
- Core temperature rises faster; risk of heat exhaustion and heat stroke
- Fluid replacement (hydration) and acclimatization are essential
- Acclimatization over 7-14 days increases plasma volume, improves sweating efficiency and earlier onset of sweating
Exercise in Cold:
- Shivering increases heat production
- Vasoconstriction protects core temperature but peripheral extremities are at risk of cold injury
- Wet cold and wind greatly increase heat loss
Consequences of Sedentary Lifestyle
Physical inactivity is now recognized as a major independent risk factor for chronic disease. Key consequences include:
- Cardiovascular disease: sedentary lifestyle is associated with increased inflammation, insulin resistance, decreased wall shear stress, and heightened vascular disease risk
- Obesity and metabolic syndrome: reduced caloric expenditure, impaired glucose metabolism
- Osteoporosis: reduced mechanical loading leads to bone loss
- Muscle atrophy (disuse atrophy)
- Depression and anxiety
- Increased all-cause mortality
Regular physical activity of moderate intensity (at least 150 minutes/week) is recommended by WHO for adults.
Chapter 104: Physiology of Yoga
General Introduction
Yoga is a holistic discipline originating in ancient India that integrates physical postures (asanas), breathing techniques (pranayama), and meditative practices (dhyana). From a physiological standpoint, yoga produces measurable effects on the autonomic nervous system, cardiovascular system, musculoskeletal system, endocrine system, and mental health.
Types of Yogic Exercises
| Type | Description |
|---|---|
| Asanas (postures) | Static or dynamic body positions improving flexibility, balance, and strength |
| Pranayama (breathing) | Controlled breathing patterns affecting autonomic and respiratory function |
| Dhyana (meditation) | Mental focus and mindfulness, reduces stress hormone levels |
| Shatkarmas | Cleansing techniques (e.g., Kapalbhati for respiratory tract) |
Major categories of asanas:
- Relaxative (e.g., Shavasana)
- Meditative (e.g., Padmasana)
- Cultural/corrective - for posture and organ function
Health Benefits of Yoga Practice
Cardiovascular:
- Reduces resting heart rate and blood pressure
- Improves heart rate variability (reflects improved parasympathetic tone)
- Lowers cholesterol and triglycerides
Respiratory:
- Pranayama improves lung volumes - vital capacity (VC) and tidal volume increase
- Improves respiratory muscle strength and efficiency
Musculoskeletal:
- Increases flexibility and range of joint motion
- Strengthens postural muscles and core stability
- Helps prevent and manage low back pain
Endocrine/Metabolic:
- Reduces cortisol (stress hormone) levels
- Improves insulin sensitivity; beneficial in Type 2 diabetes
- Balances thyroid function
Neurological/Psychological:
- Stimulates parasympathetic nervous system (rest-and-digest), countering chronic sympathetic over-activation
- Reduces anxiety, depression, and perceived stress
- Improves sleep quality
- Increases GABA levels in the brain (anti-anxiety)
Yoga in Health and Disease
- Hypertension: yoga's parasympathomimetic effect reduces sympathetic drive and lowers BP
- Diabetes mellitus: improves glycemic control and insulin sensitivity
- Asthma and COPD: pranayama improves breathing efficiency
- Depression/anxiety: meditative practices reduce cortisol, increase serotonin
- Obesity: combined effect of physical activity + stress reduction + improved eating behaviors
- Osteoporosis: weight-bearing asanas stimulate bone formation
- Arthritis: gentle movement improves joint lubrication and reduces stiffness
Yoga vs. Conventional Exercises
| Parameter | Yoga | Conventional Exercise |
|---|---|---|
| Primary focus | Mind-body integration | Physical performance |
| Intensity | Low-moderate | Variable (low to very high) |
| Caloric expenditure | Moderate | Higher |
| Cardiovascular training | Moderate | High (aerobics/HIIT) |
| Flexibility | Excellent | Moderate (unless stretched) |
| Stress/autonomic effects | Strong parasympathetic shift | Sympathetic activation during; parasympathetic after |
| Injury risk | Low | Higher (especially high-intensity) |
| Suitability | All ages, chronic illness | Primarily healthy/active populations |
The two are complementary rather than mutually exclusive. Yoga excels in stress management and flexibility; conventional aerobic exercise excels in cardiovascular fitness and caloric expenditure.
Chapter 105: Physiology of Infancy and Aging
Physiology of Infancy
Infancy spans birth to 1 year of age and is a period of rapid physiological adaptation and development.
At birth (transition from fetal to neonatal life):
- Circulatory transition: The foramen ovale and ductus arteriosus close (functional closure within hours, anatomical within weeks), converting from parallel fetal circulation to adult serial circulation
- Respiratory onset: First breath is triggered by hypoxia, hypercarbia, cold stimulation, and tactile stimulation at birth
- Thermoregulation: Neonates are poikilothermic - they lose heat rapidly due to high surface area:body mass ratio and thin subcutaneous fat. Brown adipose tissue (BAT) - unique to neonates - provides non-shivering thermogenesis via uncoupling of oxidative phosphorylation
Key physiological features of infants vs. adults:
| Parameter | Infant | Adult |
|---|---|---|
| Heart rate | 120-160 bpm | 60-100 bpm |
| Respiratory rate | 40-60 breaths/min | 12-18 breaths/min |
| Blood pressure | 60-90/30-60 mmHg | 120/80 mmHg |
| Hemoglobin type | Fetal HbF (higher O₂ affinity) shifts to HbA | Adult HbA |
| Renal function | Immature - poor concentrating ability | Fully mature |
| Immune system | Passive immunity from maternal IgG; active immunity developing | Fully active |
Neonatal brain: Rapidly growing; myelination of nerve fibers continues until early adulthood. The blood-brain barrier is less complete in neonates, making them more susceptible to certain drugs and toxins.
Growth: Infants double their birth weight by 5-6 months and triple it by 1 year. Growth hormone and thyroid hormone are critical regulators.
Aging and Free Radicals and Antioxidants
The Free Radical Theory of Aging:
The most widely accepted cellular theory of aging proposes that reactive oxygen species (ROS) - also called free radicals - accumulate over a lifetime and progressively damage cellular components:
Sources of Free Radicals (ROS):
- Normal byproduct of mitochondrial oxidative phosphorylation (electron leakage)
- Inflammatory reactions
- UV radiation, ionizing radiation
- Environmental toxins, cigarette smoke
- Ischemia-reperfusion injury
Damage Caused by ROS:
- DNA damage: strand breaks, base modifications - leads to mutations and cancer
- Lipid peroxidation: damage to cell membranes
- Protein oxidation: inactivates enzymes
- Mitochondrial damage: creates a vicious cycle of more ROS production
Antioxidant Defense Systems:
The body combats oxidative damage through:
| Antioxidant | Type | Mechanism |
|---|---|---|
| Superoxide dismutase (SOD) | Enzyme | Converts O₂•⁻ to H₂O₂ |
| Catalase | Enzyme | Converts H₂O₂ to H₂O + O₂ |
| Glutathione peroxidase | Enzyme | Neutralizes H₂O₂ and lipid peroxides |
| Vitamin E (tocopherol) | Dietary | Scavenges lipid radicals in membranes |
| Vitamin C (ascorbate) | Dietary | Water-soluble radical scavenger |
| Beta-carotene | Dietary | Quenches singlet oxygen |
| Alpha-lipoic acid | Dietary | Potent antioxidant in dermis; may reduce both intrinsic and extrinsic aging from free radical damage |
Aging Changes Across Systems:
- Cardiovascular: Reduced cardiac output, arterial stiffening (atherosclerosis), hypertension
- Respiratory: Reduced vital capacity, decreased elastic recoil of lungs
- Renal: Reduced GFR (decreases ~1% per year after age 40), reduced tubular function
- Nervous system: Neuronal loss, reduced neurotransmitter levels, slowed conduction velocities, memory decline
- Musculoskeletal: Sarcopenia (muscle wasting), osteoporosis, joint degeneration
- Immune system: Immunosenescence - reduced T-cell function, increased autoimmunity and infection susceptibility
- Hormonal: Menopause (women), andropause (men), reduced growth hormone and IGF-1
Brain Death
Definition: Brain death is the irreversible cessation of all brain functions, including the brainstem, while the heart may continue to beat with ventilatory support. It is legally and medically accepted as the definition of death in most countries.
Criteria for Brain Death (must fulfill all):
- Coma - completely unresponsive to all external stimuli
- Absence of all brainstem reflexes:
- No pupillary light reflex (pupils fixed and dilated)
- No corneal reflex
- No oculovestibular (caloric) reflex
- No gag or cough reflex
- No oculocephalic reflex (doll's eye absent)
- Apnea test positive - no spontaneous breathing even when PaCO₂ rises to ≥60 mmHg, confirming complete loss of respiratory drive
- Irreversibility confirmed - known cause, reversible causes ruled out (hypothermia, drug intoxication, metabolic disturbances excluded)
Confirmatory tests (when clinical tests are inconclusive):
- EEG - shows electrocerebral silence (flat trace)
- Cerebral angiography - no intracranial blood flow
- Transcranial Doppler - absent cerebral blood flow
- Radionuclide scan (SPECT) - no cerebral perfusion
Persistent Vegetative State (PVS) vs. Brain Death:
- In PVS, the brainstem functions are preserved (breathing, reflexes intact), but higher cortical functions are lost
- Brain death is complete and irreversible loss including brainstem - PVS is not brain death
Clinical Significance:
- Brain death declaration allows discontinuation of mechanical ventilation
- It is the medical and legal prerequisite for organ donation
- Two independent physicians must certify brain death
Quick Revision Summary for Exams
| Chapter | Key Concept | Remember |
|---|---|---|
| 102 - Thermoregulation | Anterior hypothalamus is the thermostat | Pyrogen → IL-1 → PGs → raise set-point → fever |
| 103 - Exercise | CO can rise 4-5x during exercise | VO₂max = best index of cardiorespiratory fitness |
| 104 - Yoga | Parasympathetic activator | Yoga + conventional exercise = complementary |
| 105 - Aging | Free radical theory | Antioxidant enzymes: SOD, Catalase, Glutathione peroxidase |
| 105 - Brain death | Irreversible loss of all brain + brainstem function | Apnea test is key clinical test |
Sources: Guyton and Hall Textbook of Medical Physiology, Costanzo Physiology 7th Ed., Medical Physiology (Boron & Boulpaep)
This is a shared conversation. Sign in to Orris to start your own chat.