Describe the placental barrier and its importance to anesthetist
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
I now have everything needed for a thorough, well-sourced answer. Here it is:
The Placental Barrier and Its Importance to the Anaesthetist
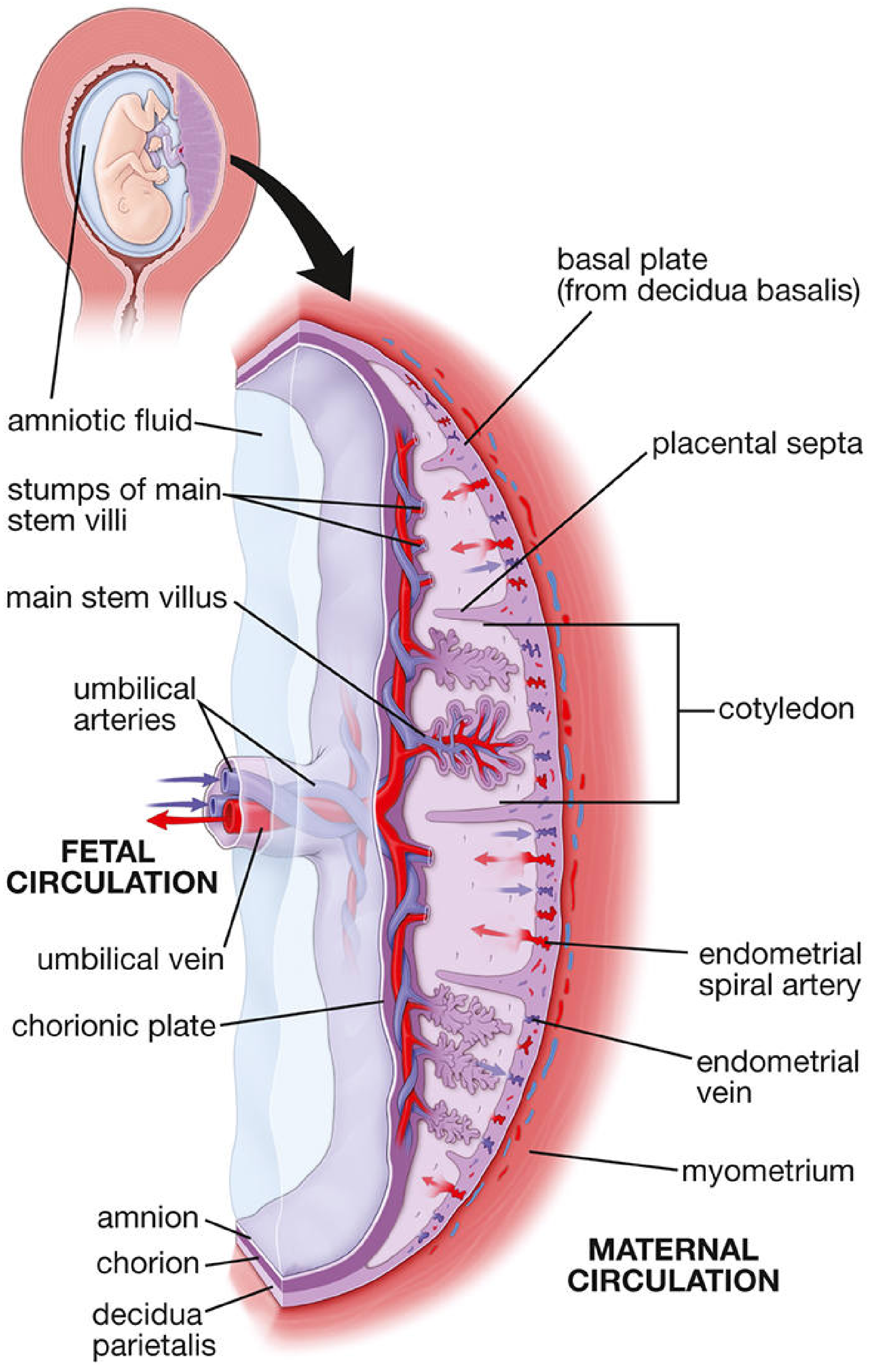
1. Structure of the Placental Barrier
At its thinnest, the placental barrier consists of six layers separating maternal from fetal blood:
- Syncytiotrophoblast - the outermost continuous layer bathed in maternal blood
- Cytotrophoblast - inner layer, thin and discontinuous in the mature placenta
- Trophoblast basal lamina
- Villus connective (mesenchymal) tissue containing Hofbauer cells (fetal macrophages)
- Endothelial basal lamina
- Fetal capillary endothelium
This structure bears a strong functional resemblance to the alveolar-capillary (air-blood) barrier of the lung, facilitating the exchange of O₂ and CO₂ between maternal and fetal circulations. Maternal blood enters the intervillous spaces via 80-100 spiral endometrial arteries, bathing ~150 mL of blood exchanged 3-4 times per minute over the villus surfaces. - Histology: A Text and Atlas (Histology A Text and Atlas With Correlated Cell and Molecular Biology)
2. Mechanisms of Drug Transfer Across the Placenta
Most drugs used in anaesthesia practice cross the placenta by one of four mechanisms:
| Mechanism | Examples |
|---|---|
| Simple (passive) diffusion | Most anaesthetic drugs; follows Fick's Law |
| Facilitated diffusion | Carrier-mediated, down concentration gradient |
| Active transport | ATP-dependent, against gradient |
| Pinocytosis/vesicular transport | Large molecules, immunoglobulins |
Simple diffusion is by far the most common. It follows Fick's Law:
Q/t = K × A × (Cm - Cf) / D
where Q/t = rate of diffusion, K = diffusion constant, A = placental surface area, Cm and Cf = free drug concentrations in maternal and fetal blood, D = membrane thickness. - Barash, Clinical Anaesthesia, 9e
3. Physicochemical Determinants of Placental Transfer
The following drug properties govern how readily a drug crosses:
a) Molecular Weight
- Drugs < 500 Da cross freely - this includes virtually all drugs used in anaesthesia practice
- 500-1000 Da: restricted transfer
-
1000 Da (e.g., heparin): minimal transfer
- Barash, Clinical Anaesthesia, 9e
b) Lipid Solubility
Highly lipophilic drugs diffuse readily across all biological membranes. This is why volatile agents (halothane, isoflurane, sevoflurane), propofol, and benzodiazepines cross easily. A useful rule of thumb: drugs that readily cross the blood-brain barrier also readily cross the placenta. - Miller's Anaesthesia, 10e
c) Degree of Ionization (pKa and pH)
Only the non-ionized form of a drug crosses the placental membrane. The degree of ionization depends on the drug's pKa and blood pH (Henderson-Hasselbalch). Fetal blood is more acidic than maternal blood (fetal pH ~7.32 vs maternal ~7.40).
This gives rise to the clinically critical concept of ion trapping:
- Weakly basic drugs (e.g., local anaesthetics, opioids) cross the placenta as non-ionized molecules
- In the more acidic fetal circulation, they become ionized
- The ionized form cannot diffuse back across the placenta
- The drug accumulates in the fetal circulation, potentially reaching levels higher than maternal blood
- During fetal distress and acidaemia, this effect is greatly amplified - Miller's Anaesthesia, 10e; Barash 9e
d) Protein Binding
Only the free (unbound) fraction of drug is available for placental transfer. The rate of transfer is inversely proportional to protein binding. However, given enough time for maternal-fetal equilibration, even highly protein-bound drugs such as bupivacaine can accumulate significantly in the fetus. - Barash, Clinical Anaesthesia, 9e
e) Uteroplacental Blood Flow
Factors reducing uteroplacental blood flow - aortocaval compression, maternal hypotension, haemorrhage, uterine contractions - reduce drug delivery to the fetus. Conversely, a drug given intravenously during a uterine contraction (when flow is transiently maximal then drops) may deliver less drug to the fetus. - Barash, Clinical Anaesthesia, 9e
4. Specific Drug Classes: Transfer and Fetal Effects
Volatile Inhalational Agents
- Readily cross the placenta due to low molecular weight and high lipophilicity
- Rapid placental transfer: detectable in umbilical vein/artery concentrations within 1 minute
- At < 1 MAC for < 10 minutes, minimal neonatal depression
- Nitrous oxide: can cause neonatal depression if induction-to-delivery interval exceeds 5-10 minutes
- Morgan & Mikhail's Clinical Anaesthesiology, 7e
Intravenous Induction Agents
| Drug | Transfer | Clinical Note |
|---|---|---|
| Propofol | Very high (highly lipophilic) | Rapid redistribution limits fetal effects at induction doses |
| Ketamine | High | < 1.5 mg/kg does not significantly alter uteroplacental flow |
| Thiopental | High | Significant hepatic first-pass in fetus reduces CNS exposure |
| Etomidate | Moderate | Minimal data on uteroplacental circulation |
| Benzodiazepines | High | Midazolam as single anxiolytic dose has no measurable fetal effect |
Opioids
- Most opioids cross readily; fetal effects vary
- Morphine: greatest neonatal respiratory depression
- Meperidine (pethidine): respiratory depression peaks 1-3 h after administration
- Fentanyl: minimal neonatal effect unless IV doses > 1 mcg/kg given immediately before delivery
- Remifentanil: crosses readily; fetal concentrations ~50% maternal; but UA/UV ratio ~30%, indicating rapid neonatal metabolism
- Epidural/intrathecal fentanyl & sufentanil: generally minimal neonatal effects
- Morgan & Mikhail's Clinical Anaesthesiology, 7e
Local Anaesthetics
Three key factors govern placental transfer: (1) pKa, (2) maternal and fetal pH, (3) protein binding
- Bupivacaine & ropivacaine: high protein binding → lower fetal blood levels; however, fetal acidosis still causes ion trapping
- Lidocaine: lower protein binding → higher fetal levels; causes uterine arterial vasoconstriction at high blood concentrations
- Chloroprocaine: least placental transfer of all - rapidly hydrolysed by maternal plasma cholinesterase before it reaches the placenta
- In fetal distress: high concentrations of local anaesthetics can cause neonatal neuromuscular depression, bradycardia, ventricular arrhythmias, acidosis, and severe cardiac depression (especially following inadvertent intravascular injection)
- Morgan & Mikhail's Clinical Anaesthesiology, 7e; Miller's Anaesthesia, 10e
Muscle Relaxants
- Highly ionized + high molecular weight + poor lipid solubility = minimal placental transfer
- Succinylcholine: low MW but highly ionized → does not readily cross at clinical doses
- Non-depolarising agents (vecuronium, rocuronium, etc.): minimal transfer
- Practical consequence: the neonate is NOT paralysed during GA for caesarean section
- Sugammadex: large molecular size and negative charge → not expected to cross in significant amounts (limited data)
- Miller's Anaesthesia, 10e
Anticholinergics
- Atropine & scopolamine: cross the placenta (non-ionized, lipophilic)
- Glycopyrrolate: does NOT cross due to its quaternary ammonium (fully ionized) structure - preferred in obstetric patients
- Morgan & Mikhail's Clinical Anaesthesiology, 7e
Other Adjuncts
- Ephedrine, beta-blockers (labetalol, esmolol), vasodilators, phenothiazines, antihistamines (H1/H2), metoclopramide: all cross the placenta
- Heparin: minimal transfer (large, highly charged molecule) - Miller's Anaesthesia, 10e
- Dexmedetomidine: may cross but is substantially stored within the placenta, reducing fetal transfer - Miller's Anaesthesia, 10e
5. Protective Mechanisms of the Fetal Circulation
Even when drugs cross the placenta, the fetal circulation provides some protection:
- Fetal hepatic first-pass: ~75% of umbilical venous blood passes through the fetal liver first. Significant hepatic uptake of thiopental, lidocaine, and halothane has been demonstrated, metabolising a portion before it reaches the fetal brain
- Progressive dilution: drug in umbilical venous blood is diluted as it mixes with venous drainage from the GI tract, lower limbs, head, and ultimately the lungs
- Uterine contractions: timing of bolus with contractions can reduce drug delivery
During asphyxia and acidosis, however, fetal cardiac output is redistributed to the brain, heart, and placenta - paradoxically increasing drug uptake in these vital organs. - Barash, Clinical Anaesthesia, 9e
6. Clinical Implications for the Anaesthetist - Summary
| Concern | Principle | Clinical Action |
|---|---|---|
| Neonatal respiratory depression | Opioids cross readily | Time opioids carefully; have naloxone ready |
| Ion trapping in fetal acidosis | Acidaemic fetus accumulates basic drugs | Maintain fetal pH; be cautious with local anaesthetics in distressed fetuses |
| GA induction-to-delivery interval | Volatile/IV agents cross rapidly | Aim for < 10 min to limit fetal drug exposure |
| Muscle paralysis risk | NMBs do not cross significantly | Use standard dosing for rapid sequence induction |
| Anticholinergic choice | Glycopyrrolate does not cross | Preferred over atropine for maternal bradycardia during obstetric anaesthesia |
| Aortocaval compression | Reduces uteroplacental flow → increases drug delivery variability | Left uterine displacement in all supine pregnant patients |
| Protein binding & accumulation | Given time, even highly bound drugs accumulate | Avoid prolonged high-dose infusions near delivery |
The fetal-to-maternal drug ratio is measured by the UV/MV ratio (umbilical vein to maternal vein concentrations). Fortunately, current anaesthetic techniques for labour and delivery - particularly neuraxial methods - generally produce minimal fetal effects despite significant placental transfer, as fetal plasma concentrations remain in the nano- to micromolar range. - Morgan & Mikhail's Clinical Anaesthesiology, 7e
Key Sources:
- Barash, Cullen & Stoelting's Clinical Anaesthesia, 9e - Chapter 41: Placental Drug Transfer
- Miller's Anaesthesia, 10e - Chapter: Drug Transfer
- Morgan & Mikhail's Clinical Anaesthesiology, 7e - Chapter 6: Placental Transfer of Anaesthetic Agents
- Histology: A Text and Atlas, 8e - Chapter 23: Placental Barrier Structure
This is a shared conversation. Sign in to Orris to start your own chat.