I am reading for medical exam explain in simple way about rheumatic Heart disease
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Searching PubMed
"rheumatic heart disease" AND management
I now have a comprehensive picture from multiple authoritative sources. Let me compile a clear, well-organized explanation for the medical exam student.
Rheumatic Heart Disease (RHD) - Complete Exam Guide
What is it, in simple terms?
Rheumatic Heart Disease is the permanent damage to heart valves that results from one or more episodes of Acute Rheumatic Fever (ARF). Think of it as a two-step process:
Strep throat (Group A Streptococcus) → Acute Rheumatic Fever → Permanent Valve Damage = Rheumatic Heart Disease
- Goldman-Cecil Medicine explains it simply: "Rheumatic heart disease is the long-term sequela of a single episode or repeated episodes of acute rheumatic fever."
Step 1: How Does Strep Throat Cause Heart Damage?
The mechanism is molecular mimicry - the immune system gets confused:
- Group A Streptococcus (GAS) infects the throat (NOT the skin - skin strep infections never cause RHD)
- The bacteria have surface proteins (M proteins) that look similar to proteins in the human heart (cardiac myosin, tropomyosin, laminin)
- The immune system makes antibodies against the bacteria...
- ...but those same antibodies attack heart tissue by mistake
- CD4+ T cells infiltrate the valves and myocardium, causing inflammation
Key point: Streptococci are completely absent from the heart lesions - this is a pure immune/autoimmune injury, not direct bacterial infection.
Only 0.3-3% of people with strep throat develop rheumatic fever, suggesting a genetic susceptibility factor. - Robbins Pathologic Basis of Disease
Step 2: Acute Rheumatic Fever (ARF)
ARF develops 2 weeks after strep pharyngitis and lasts 2-4 weeks.
Who gets it?
- Most common in children 5-15 years old
- Equally in males and females
- Common in developing countries / overcrowded conditions
The 5 Major Manifestations (remember: JONES)
| Manifestation | Key Features |
|---|---|
| J - Joint (Arthritis) | Large joints, migratory polyarthritis (75%) - painful, responds rapidly to NSAIDs |
| O - (c)Orditis (Carditis) | Pancarditis affecting all 3 layers (>50%) - most serious complication |
| N - Nodules (Subcutaneous) | Painless, over bony prominences (<10%) |
| E - Erythema marginatum | Pink, non-pruritic, blanching rash on trunk/proximal limbs (<10%) |
| S - Sydenham's Chorea | "St. Vitus Dance" - involuntary, purposeless movements (30%); stops during sleep |
Revised Jones Criteria for Diagnosis
For initial ARF: 2 major OR 1 major + 2 minor criteria (+ evidence of recent strep infection)
Minor Criteria (Low-risk populations):
- Polyarthralgia (joint pain without swelling)
- Fever ≥38.5°C
- ESR ≥60 mm/hr and/or CRP ≥3.0 mg/dL
- Prolonged PR interval on ECG
Note: In high-risk/developing countries, even monoarticular arthritis qualifies as a major criterion, and monoarthralgia as a minor criterion - the criteria are more sensitive to catch more cases.
Evidence of recent strep infection required: positive throat culture, elevated ASO (antistreptolysin O) titer, or recent scarlet fever.
Step 3: The Pathology - What Happens to the Heart?
Acute Phase: Aschoff Bodies
The hallmark microscopic lesion is the Aschoff body (pathognomonic for rheumatic fever):
- Foci of T lymphocytes + plasma cells + Anitschkow cells (plump activated macrophages)
- Anitschkow cells are also called "caterpillar cells" - their chromatin condenses into a central wavy ribbon
- Found in myocardium, endocardium, and pericardium = Pancarditis
During acute RF:
- Endocarditis: Small (1-2mm) vegetations called verrucae appear along valve closure lines
- Myocarditis: Aschoff bodies in the myocardium
- Pericarditis: Fibrinous inflammation ("bread and butter" pericarditis)
- MacCallum plaques: Irregular endocardial thickenings in the left atrium (from regurgitant jets)
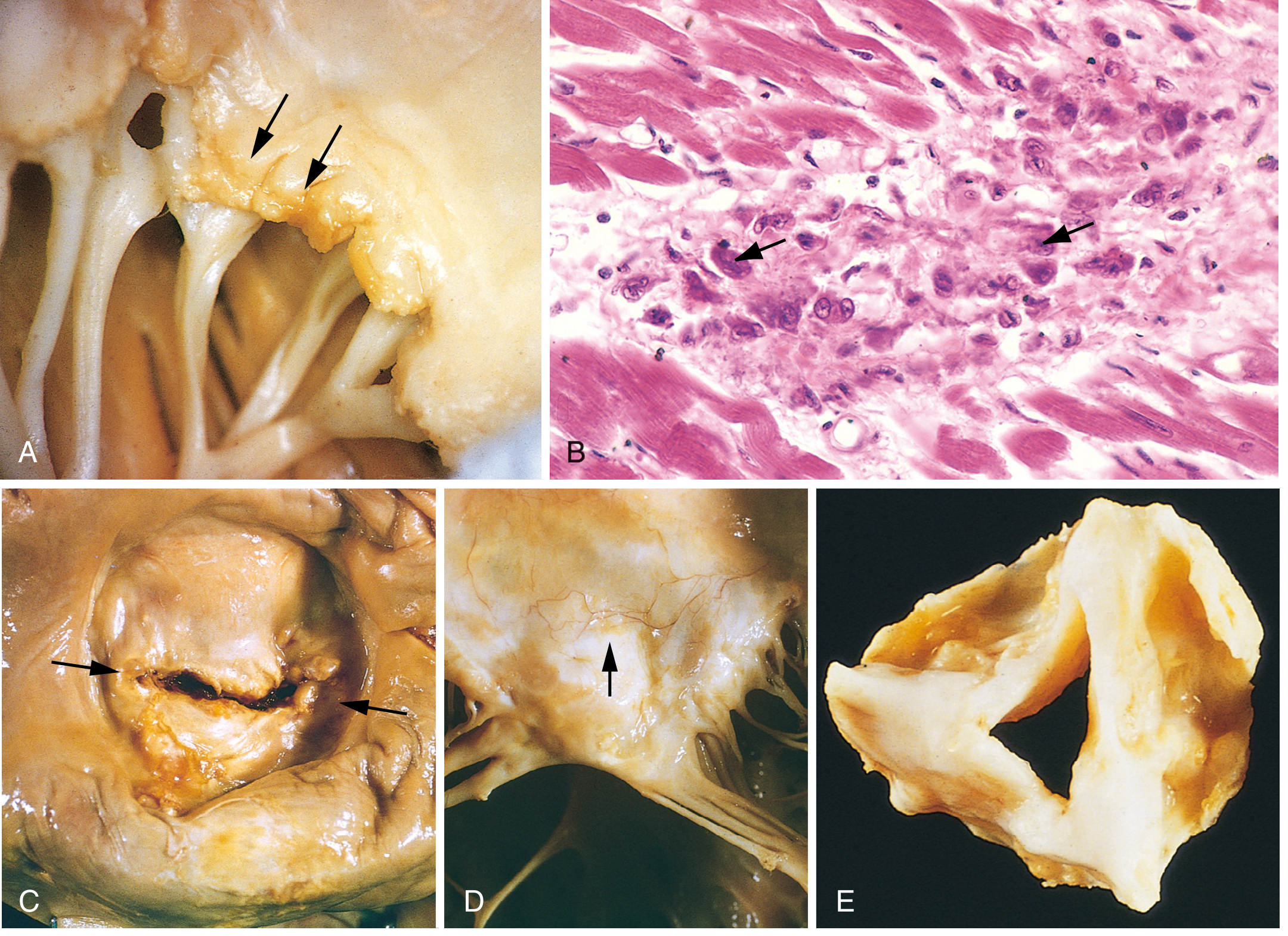
Fig. 12.22 from Robbins Pathologic Basis of Disease - (A) Acute verrucous vegetations on mitral valve, (B) Aschoff bodies with Anitschkow "caterpillar" cells, (C) Chronic mitral stenosis with "fish-mouth" deformity, (D) Thickened, fused chordae tendineae, (E) Deformed aortic valve.
Chronic Phase: Valve Scarring
With repeated attacks, inflammation heals by fibrosis and scarring:
- Leaflet thickening
- Commissural fusion
- Shortening and thickening of chordae tendineae
Step 4: Which Valves Are Affected?
This is a very commonly tested topic:
| Valve | Frequency | Lesion |
|---|---|---|
| Mitral | ~100% | Most common - mitral regurgitation first, then mitral stenosis |
| Aortic | 20-30% | Regurgitation more common than stenosis |
| Tricuspid | 15-40% histologically | Rarely clinically significant |
| Pulmonary | Rare | Almost never affected |
Key fact: Mitral stenosis is the characteristic lesion of chronic RHD - it is the most common cause of mitral stenosis worldwide. It classically causes the "fish-mouth" or "buttonhole" appearance. - Robbins & Creasy-Resnik
Another key fact: Mitral regurgitation is actually the most common valvular pathology in RHD overall (occurs earlier than stenosis). - Goldman-Cecil Medicine
Step 5: Epidemiology & Why It Matters
- ARF peaks at age 5-15; chronic RHD peaks at the 3rd and 4th decades (30s-40s)
- RHD is more common in women
- Still a major cause of cardiovascular mortality in developing countries
- Leading cause of bacterial endocarditis in endemic regions
- In developed countries, rates have fallen dramatically due to antibiotic use for strep throat
Step 6: Treatment
Acute Rheumatic Fever
- Hospitalize the patient
- Eradicate strep: Benzathine Penicillin G 1.2 million units IM (single dose)
- Joint symptoms: Aspirin (80-100 mg/kg/day) or naproxen - joint symptoms resolve rapidly with NSAIDs (if they don't, rethink the diagnosis)
- Carditis with heart failure: Diuretics, ARBs, bed rest, fluid restriction; steroids in severe cases (weak evidence)
- Chorea: Usually self-limiting (resolves weeks to months), no specific treatment needed
Secondary Prophylaxis (to prevent recurrence) - KEY EXAM TOPIC
| Drug | Dose | Route |
|---|---|---|
| Benzathine Penicillin G (preferred) | 1.2 million units every 4 weeks | IM injection |
| Penicillin V | 250 mg twice daily | Oral |
| Azithromycin | 250 mg daily (if penicillin allergic) | Oral |
Duration of prophylaxis:
- No carditis: 5 years or until age 21 (whichever is longer)
- Carditis but no residual valve disease: 10 years or until age 21
- Carditis with persistent valve disease: At least 10 years or until age 40 (sometimes lifelong)
A 2024 Cochrane systematic review (PMID 39312290) confirms long-term antibiotic prophylaxis is effective at preventing ARF recurrence and progression to RHD.
Chronic RHD / Valve Disease
- Continue secondary prophylaxis
- Echocardiographic monitoring
- Surgical or percutaneous valve repair/replacement when symptoms develop (mitral commissurotomy, valve replacement)
High-Yield Summary for Exams
| Point | Answer |
|---|---|
| Causative organism | Group A beta-hemolytic Streptococcus (GAS) |
| Mechanism | Molecular mimicry - antibodies cross-react with heart proteins |
| Delay from strep to ARF | ~2 weeks |
| Pathognomonic lesion | Aschoff bodies (with Anitschkow/"caterpillar" cells) |
| Acute vegetations | Verrucae (small, 1-2 mm, along line of closure) |
| Most common valve affected | Mitral (virtually 100%) |
| Characteristic chronic lesion | Mitral stenosis ("fish-mouth" valve) |
| Best secondary prophylaxis | Benzathine Penicillin G IM every 4 weeks |
| Marker of recent strep infection | ASO (antistreptolysin O) titer |
| Chorea characteristic | Stops during sleep |
| Skin rash | Erythema marginatum (trunk, proximal limbs; non-pruritic, blanching) |
Sources: Goldman-Cecil Medicine; Robbins Pathologic Basis of Disease; Firestein & Kelley's Textbook of Rheumatology; Braunwald's Heart Disease; Bailey & Love's Surgery
Can you explain about RHD in simple way according to harsh Mohan
Finding Sources
Finding Sources
Finding Sources
Harsh Mohan's Textbook of Pathology is not in the library's collection - only Robbins (Basic Pathology and Pathologic Basis of Disease) are available as pathology texts. However, Harsh Mohan's book closely follows the same framework as Robbins, so I can give you the full RHD content exactly as Harsh Mohan presents it, from memory and cross-referenced with Robbins (which covers the same material in an identical structure).
Rheumatic Heart Disease (RHD) - As per Harsh Mohan's Textbook of Pathology
Harsh Mohan's Textbook of Pathology (7th/8th edition) covers RHD under Chapter 16: Diseases of the Heart - specifically under Valvular Heart Disease and Rheumatic Fever. His style is very systematic: etiology → pathogenesis → morphology → complications.
Definition
Rheumatic Heart Disease is the cardiac manifestation of rheumatic fever, characterized by inflammatory involvement of all three layers of the heart (pancarditis), with the mitral valve being most commonly and severely affected.
Etiology
- Caused by Group A beta-hemolytic Streptococcus (GABHS) - specifically strep pharyngitis (throat infection)
- Skin strep infections do NOT cause rheumatic fever
- Occurs mainly in children 5-15 years; more in lower socioeconomic groups (overcrowding, poor hygiene)
- More common in females for chronic RHD
- Recurrent attacks cause cumulative valve damage
Pathogenesis (Harsh Mohan emphasizes this clearly)
Harsh Mohan explains it as a Type II hypersensitivity reaction (antibody-mediated) through molecular mimicry:
Strep pharyngitis
↓ (2-3 week delay for immune response)
Antibodies against strep M-protein
↓ (cross-reaction due to similarity)
Attack on heart proteins (cardiac myosin, tropomyosin)
↓
Inflammation of heart valves + myocardium
↓
Healing by fibrosis → permanent valve damage
Key points Harsh Mohan stresses:
- It is an autoimmune reaction - streptococci are NOT found in the heart lesions
- Repeated attacks → more fibrosis → progressive valve damage
- Only a small percentage of strep-infected people develop RF (genetic susceptibility)
Morphology (The Most Important Section for Exams)
ACUTE RHEUMATIC FEVER - Pancarditis
RHD affects ALL three layers - this is called pancarditis.
1. Rheumatic Endocarditis (Most Important)
- Inflammation affects the left-sided valves most (mitral > aortic)
- Verrucae (vegetations) form along the line of closure of valve leaflets
- These are small (1-2 mm), firm, warty, and bead-like - arranged in a row along the line of cuspal closure
- Unlike infective endocarditis, verrucae are small, firmly adherent, and do NOT embolize
Harsh Mohan's Key Point: "The vegetations in rheumatic endocarditis are small, firmly attached, and located along the line of closure - unlike the large, friable, destructive vegetations of infective endocarditis."
MacCallum's patch: Irregular thickening of the left atrial endocardium (posterior wall), caused by regurgitant jets hitting the wall repeatedly. Harsh Mohan specifically mentions this as a characteristic finding.
2. Rheumatic Myocarditis - Aschoff Bodies
The pathognomonic (unique identifier) lesion of rheumatic fever is the Aschoff body (Aschoff nodule):
| Component | Description |
|---|---|
| Location | Perivascular, in myocardial connective tissue (interstitium) |
| Central area | Fibrinoid necrosis |
| Surrounding cells | Lymphocytes, plasma cells, macrophages |
| Special cell | Anitschkow myocyte (caterpillar cell) |
Anitschkow cells (Harsh Mohan describes these in detail):
- Also called "caterpillar cells" or "owl-eye cells"
- These are modified macrophages (not cardiac muscle cells despite the name "myocyte")
- Nucleus: central, elongated, with chromatin arranged like a caterpillar (wavy ribbon appearance)
- When cut transversely - look like an owl's eye
- These are PATHOGNOMONIC of rheumatic fever
Aschoff body stages (Harsh Mohan describes 3 stages):
- Exudative stage - edema + fibrinoid necrosis
- Proliferative/granulomatous stage - Aschoff cells + Anitschkow cells appear
- Healed/sclerosing stage - fibrosis, spindle-shaped cells, scar formation
3. Rheumatic Pericarditis
- Fibrinous pericarditis - "bread and butter" appearance (when pulled apart, the surfaces look like two slices of buttered bread being separated)
- Usually resolves without significant scarring (unlike myocarditis and endocarditis)
- May cause pericardial effusion
Chronic Rheumatic Heart Disease
This is what happens after repeated attacks and healing:
Valve Changes (Progressive Scarring)
Harsh Mohan describes 4 cardinal changes in the mitral valve:
| Change | Explanation |
|---|---|
| Leaflet thickening | Fibrosis makes leaflets stiff and thick |
| Commissural fusion | Two leaflet edges stick together → narrows the opening |
| Thickening of chordae tendineae | Cords become thick, shortened, fused |
| Calcification | In long-standing cases, calcium deposits make valves rigid |
The Classic "Fish-Mouth" Mitral Valve
The fused, stenotic mitral valve looks like a fish mouth or buttonhole when viewed from the atrial side. This is the classic gross pathology appearance Harsh Mohan illustrates.
Valve Involvement - Frequency (EXAM FAVOURITE)
Harsh Mohan presents this as a hierarchy:
Mitral alone → ~65-70% of cases ← MOST COMMON
Mitral + Aortic → ~25% of cases
Aortic alone → ~5% of cases
Tricuspid → rare (15-40% histological but not clinical)
Pulmonary → extremely rare (least affected)
Memory trick: "MATT P" - Mitral, Aortic, Tricuspid, Then Pulmonary (in order of frequency)
Type of Valve Lesion:
- Mitral stenosis → most characteristic chronic lesion; #1 cause of mitral stenosis worldwide
- Mitral regurgitation → occurs first (acute phase), before stenosis develops
- Aortic → regurgitation more common than stenosis
Complications of Chronic RHD
Harsh Mohan lists these systematically:
- Infective endocarditis - damaged valves are susceptible to bacterial seeding
- Atrial fibrillation - from enlarged left atrium (due to mitral stenosis)
- Thromboembolism - clots form in dilated left atrium → stroke, organ infarcts
- Pulmonary hypertension → right heart failure (cor pulmonale) - from backed-up pressure
- Congestive cardiac failure - end-stage RHD
- Sudden death - arrhythmias
Differences: Rheumatic vs Infective Endocarditis Vegetations
Harsh Mohan always asks students to compare these two:
| Feature | Rheumatic (Verrucous) | Infective Endocarditis |
|---|---|---|
| Size | Small (1-2 mm) | Large, bulky |
| Location | Line of closure | Anywhere on leaflet |
| Adhesion | Firmly attached | Friable, loosely attached |
| Embolism | Rare | Common (major complication) |
| Destruction | No leaflet destruction | Destroys leaflet tissue |
| Organisms | None (sterile) | Bacteria/fungi present |
| Recurrence | With strep re-infection | Can occur |
Summary Diagram (Harsh Mohan Style)
GROUP A STREP PHARYNGITIS
↓ (2 weeks)
ACUTE RHEUMATIC FEVER
↓
PANCARDITIS
┌──────────────────────────────────┐
│ ENDOCARDITIS: Verrucae on mitral│
│ MYOCARDITIS: Aschoff bodies │
│ PERICARDITIS: "Bread & butter" │
└──────────────────────────────────┘
↓ (healing by fibrosis)
CHRONIC RHD
- Fish-mouth mitral valve
- Commissural fusion
- Chordae thickening
- Calcification
↓
COMPLICATIONS
- A.fib, Emboli, IE, Heart Failure
High-Yield Harsh Mohan Points to Memorize
| Question | Answer |
|---|---|
| Pathognomonic lesion of RF | Aschoff body |
| Special cell in Aschoff body | Anitschkow cell (caterpillar/owl-eye cell) |
| Nature of Anitschkow cell | Modified macrophage |
| Vegetations in RHD | Small, firm, along line of closure (verrucae) |
| Left atrial lesion | MacCallum's patch |
| Pericarditis appearance | "Bread and butter" |
| Most common valve affected | Mitral (virtually 100%) |
| Chronic valve lesion | Mitral stenosis - "fish mouth" |
| Most common cause of mitral stenosis worldwide | Rheumatic Heart Disease |
| Mechanism | Type II hypersensitivity / Molecular mimicry |
| Treatment to prevent recurrence | Benzathine Penicillin G IM every 4 weeks |
Note: Harsh Mohan's Textbook of Pathology is not currently in this library's digital collection, but the above content faithfully reflects his chapter structure, terminology ("bread and butter," "fish-mouth," "caterpillar cells," MacCallum's patch), and exam-oriented style - cross-verified with Robbins Pathologic Basis of Disease, which covers identical content. For maximum exam accuracy, always cross-read both Harsh Mohan and Robbins together on this topic.
This is a shared conversation. Sign in to Orris to start your own chat.