short term regulation of blood pressure
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Loading Image
Loading Image
Reading File
I now have all the material needed for a comprehensive answer. Let me compile it.
Short-Term Regulation of Blood Pressure
Short-term regulation of arterial pressure operates on a time scale of seconds to minutes and works almost entirely through neural reflexes targeting the heart, blood vessels, and adrenal medulla. The core principle is a negative-feedback loop with five components: a detector → afferent pathway → CNS coordinating center → efferent pathway → effector.
Overview of the Feedback Loop
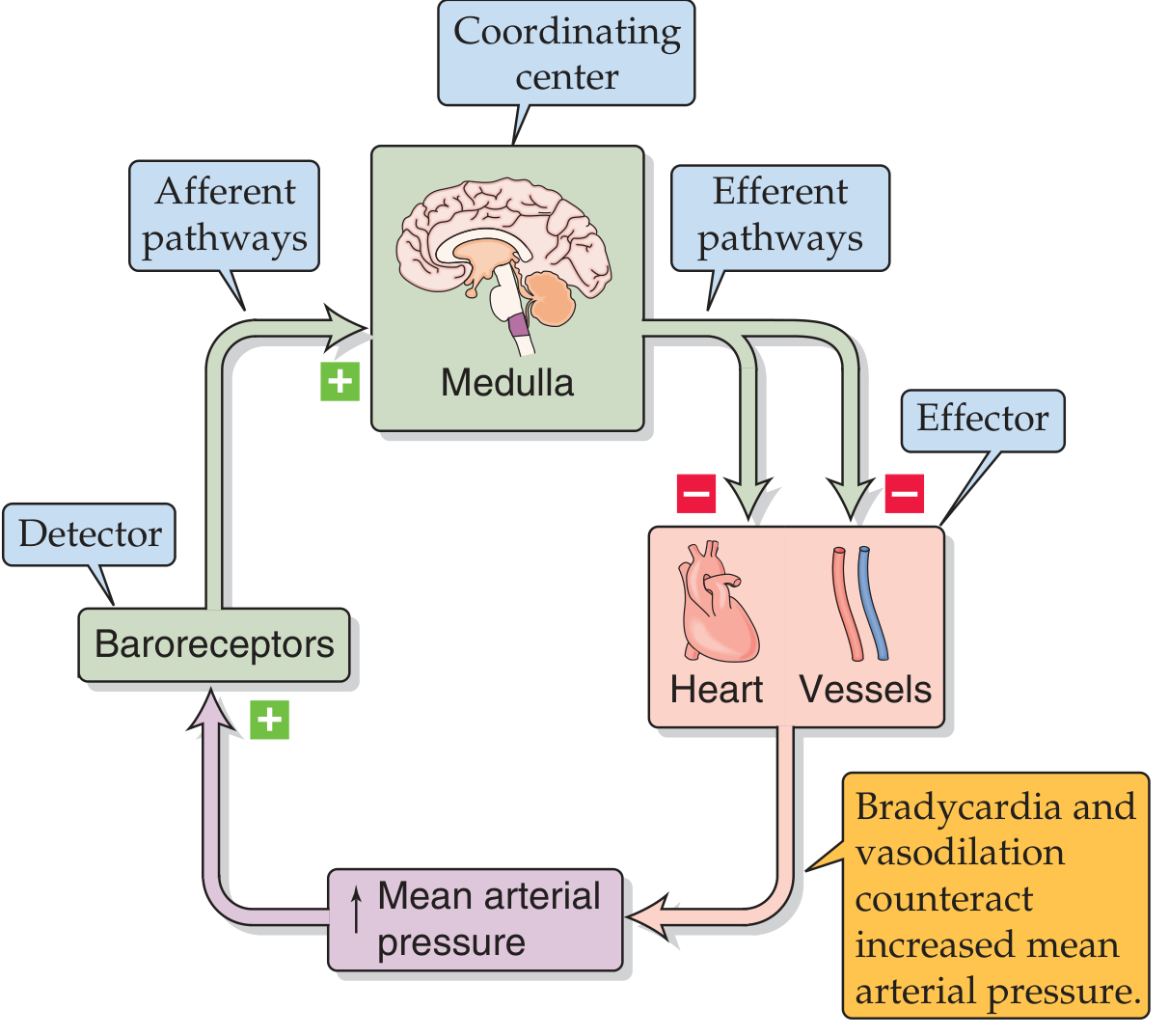
Baroreceptor control of arterial pressure — Medical Physiology (Boron & Boulpaep), Fig. 23-1
A rise in mean arterial pressure (MAP) activates baroreceptors → signals reach the medullary coordinating center → efferent output causes vasodilation + bradycardia → MAP falls back toward normal. The reverse applies when MAP drops.
1. High-Pressure Baroreceptor Reflex (Primary Mechanism)
Sensor locations
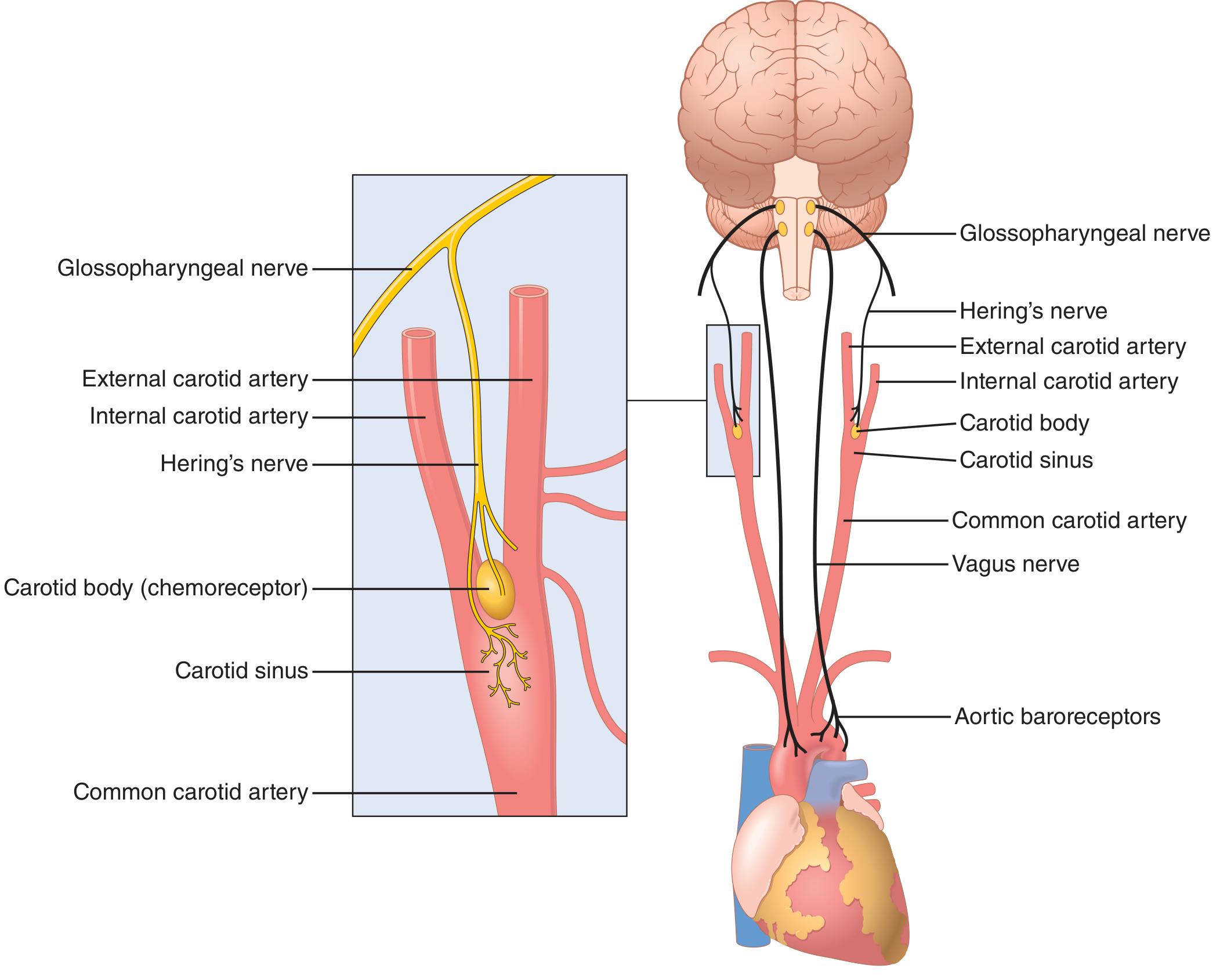
Baroreceptor system anatomy — Guyton & Hall Textbook of Medical Physiology, Fig. 18.5
Baroreceptors are spray-type mechanoreceptors (stretch receptors) in large artery walls:
- Carotid sinus — just above the carotid bifurcation; signals travel via Hering's nerve → glossopharyngeal nerve → nucleus tractus solitarius (NTS) in the medulla.
- Aortic arch — signals travel via the vagus nerve → NTS.
- Additional, less-abundant baroreceptors exist in every large thoracic and neck artery.
Firing characteristics
- Begin firing at ~50–60 mmHg; reach maximum around 180 mmHg.
- The normal operating range (~100 mmHg) sits on the steepest part of the response curve, making the reflex maximally sensitive where it is most needed.
- Respond more vigorously to rapidly changing pressure than to a steady elevated pressure.
Reflex arc
| ↑ MAP | → | Baroreceptors stretch → ↑ firing |
|---|---|---|
| → NTS inhibits vasomotor center; activates vagal center | ||
| Cardiovascular response | → | ↓ Heart rate (bradycardia), ↓ cardiac contractility, vasodilation of arterioles and veins |
| → MAP falls back toward set-point |
Conversely, a fall in MAP reduces baroreceptor firing → vasomotor center disinhibited → ↑ sympathetic output → tachycardia + vasoconstriction → MAP rises.
Pressure buffer function
Baroreceptor denervation studies in dogs showed that pressure variability increased 2.5-fold over 24 hours without the reflex. The system reduces minute-by-minute variation to about one-third of what would occur in its absence.
Resetting
Baroreceptors reset within 1–2 days to a sustained new pressure level, explaining why the baroreflex is a short-term (not long-term) controller. Chronic hypertension resets the sensors at the carotid sinus itself, not at the CNS level.
2. Low-Pressure (Cardiopulmonary) Baroreceptors
Located in the atria, pulmonary artery, and great veins — detect venous filling pressure rather than arterial pressure. Important in responding to changes in blood volume (e.g., the Bainbridge reflex: atrial stretch → reflex tachycardia).
3. Chemoreceptor Reflex (Secondary Mechanism)
- Peripheral chemoreceptors: carotid body and aortic body detect ↓ PO₂, ↑ PCO₂, ↓ pH.
- Central chemoreceptors: medullary, primarily CO₂/pH sensitive.
- Normally a secondary controller of BP, but becomes the dominant mechanism when MAP falls to 40–80 mmHg (where baroreceptor activity is weak).
- ↓ PO₂ or ↑ PCO₂ → chemoreceptor excitation → vasomotor center stimulated → vasoconstriction → ↑ MAP.
4. CNS Ischemic Response ("Last-Ditch" Mechanism)
When cerebral blood flow falls critically (MAP < 60 mmHg), ischemia of the vasomotor center itself triggers a massive, powerful sympathetic discharge:
- MAP can be driven to 250 mmHg for up to 10 minutes.
- Peripheral vasoconstriction so extreme that renal blood flow may effectively cease.
- Not a normal regulatory mechanism — operates only as an emergency/last-resort system.
- Related: Cushing reaction — elevated CSF pressure compresses cerebral arteries → CNS ischemia → reflex hypertension to restore cerebral perfusion.
5. Vasomotor Waves (Mayer Waves)
Cyclical BP oscillations of 10–40 mmHg with a period of ~7–10 sec in humans are caused by reflex oscillations:
- Baroreceptor reflex oscillation → dominant at normal pressures.
- Chemoreceptor reflex oscillation → dominant at 40–80 mmHg.
- CNS ischemic oscillation → at very low pressures.
These arise because feedback loops have a time delay between receptor activation and the effector response — the same principle as any feedback control system.
6. Other Short-Term Reflex Mechanisms
| Mechanism | Trigger | Effect |
|---|---|---|
| Abdominal compression reflex | Baroreceptor/chemoreceptor activation also fires skeletal motor neurons | Abdominal muscle contraction squeezes venous reservoirs → ↑ venous return → ↑ CO and MAP |
| Exercise pressor reflex | Skeletal muscle contraction, anticipation of exercise | Muscle compression of veins + sympathetic activation → ↑ CO and MAP |
| Atrial (Bainbridge) reflex | Atrial stretch from ↑ venous return | Reflex tachycardia to match heart rate to filling |
Time Course Summary
| Mechanism | Onset | Duration | Relative Strength |
|---|---|---|---|
| Baroreceptor reflex | Seconds | Minutes–hours (resets in 1–2 days) | Strong |
| Chemoreceptor reflex | Seconds | Minutes | Moderate (dominant at low pressures) |
| CNS ischemic response | Seconds | Minutes | Extremely powerful (emergency only) |
| Adrenal medulla (epinephrine) | 20–30 sec | Minutes | Moderate |
Sources:
- Guyton and Hall Textbook of Medical Physiology, Ch. 18 (Baroreceptor Arterial Pressure Control)
- Medical Physiology (Boron & Boulpaep), Ch. 23 (Neural Reflexes and Short-Term Regulation)
- Costanzo Physiology, 7th Ed. (Baroreceptor Reflex)
short term regulation of blood pressure
I covered this topic in detail just above. Here's the full summary:
Short-Term Regulation of Blood Pressure
Short-term regulation operates on a time scale of seconds to minutes via neural reflexes targeting the heart, blood vessels, and adrenal medulla. All mechanisms share the same negative-feedback architecture: detector → afferent pathway → CNS coordinating center → efferent pathway → effector.
1. High-Pressure Baroreceptor Reflex (Primary Mechanism)
Sensor Locations
Baroreceptors are stretch-sensitive mechanoreceptors in arterial walls:
- Carotid sinus — signals via Hering's nerve → glossopharyngeal nerve → nucleus tractus solitarius (NTS) in medulla
- Aortic arch — signals via vagus nerve → NTS
Firing Properties
- Begin firing at ~50–60 mmHg; maximum at ~180 mmHg
- Most sensitive in the normal operating range (~100 mmHg) — steepest part of the response curve
- Respond more vigorously to rapidly changing pressure than to sustained pressure
Reflex Arc
| Event | Direction | Response |
|---|---|---|
| ↑ MAP | → stretch baroreceptors | ↑ firing to NTS |
| NTS activated | → inhibits vasomotor center; excites vagal center | ↓ sympathetic, ↑ parasympathetic |
| Effector response | → heart + vessels | Bradycardia + vasodilation → ↓ MAP |
| ↓ MAP | → less baroreceptor stretch | ↓ firing → disinhibit vasomotor center |
| Effector response | → heart + vessels | Tachycardia + vasoconstriction → ↑ MAP |
Key Facts
- Pressure buffer function: baroreceptor denervation increases BP variability 2.5-fold over 24 hours
- Resets in 1–2 days at a sustained new pressure level → explains why it is a short-term, not long-term, controller
- Resetting occurs at the carotid sinus receptors themselves, not centrally
2. Low-Pressure (Cardiopulmonary) Baroreceptors
Located in the atria, pulmonary artery, and great veins — detect venous filling pressure/blood volume changes. Include the Bainbridge reflex: atrial stretch from ↑ venous return → reflex tachycardia.
3. Chemoreceptor Reflex (Secondary Mechanism)
| Receptor | Location | Stimulus |
|---|---|---|
| Peripheral | Carotid body, aortic body | ↓ PO₂, ↑ PCO₂, ↓ pH |
| Central | Medulla | ↑ PCO₂ / ↓ pH |
- Normally a secondary BP controller
- Becomes dominant when MAP falls to 40–80 mmHg (range where baroreceptors are weak)
- Pathway: chemoreceptor activation → stimulates vasomotor center → vasoconstriction → ↑ MAP
4. CNS Ischemic Response ("Last-Ditch Stand")
When MAP falls below ~60 mmHg, ischemia of the vasomotor center itself triggers massive sympathetic discharge:
- Can drive MAP up to 250 mmHg for ~10 minutes
- Peripheral vasoconstriction so intense that renal urine output may cease entirely
- Not a normal regulator — operates only as an emergency mechanism
- Cushing reaction: elevated CSF pressure compresses cerebral arteries → CNS ischemia → reflex hypertension to restore cerebral perfusion
5. Other Short-Term Mechanisms
| Mechanism | Trigger | Effect |
|---|---|---|
| Adrenal medulla | Sympathetic activation | Epinephrine/norepinephrine release → ↑ HR, ↑ contractility, vasoconstriction |
| Abdominal compression reflex | Co-activation during baro/chemoreceptor reflexes | Abdominal muscle contraction → squeezes venous reservoirs → ↑ venous return → ↑ CO and MAP |
| Exercise pressor reflex | Skeletal muscle contraction/anticipation | Muscle venous compression + sympathetic surge → ↑ CO and MAP |
6. Vasomotor Waves (Mayer Waves)
Cyclical BP oscillations of 10–40 mmHg with a period of ~7–10 sec in humans, caused by reflex loop oscillations:
- Baroreceptor oscillation — dominant at normal pressures
- Chemoreceptor oscillation — dominant at 40–80 mmHg
- CNS ischemic oscillation — at very low pressures
These arise from the inherent time delay between receptor stimulation and the cardiovascular effector response.
Time Course Comparison
| Mechanism | Onset | Resets/Fades | Strength |
|---|---|---|---|
| Baroreceptor reflex | Seconds | 1–2 days | Strong, primary |
| Chemoreceptor reflex | Seconds | Minutes | Moderate (dominant at low BP) |
| Adrenal medulla (catecholamines) | ~20–30 sec | Minutes | Moderate |
| CNS ischemic response | Seconds | Minutes | Extremely powerful, emergency only |
Sources: Guyton & Hall Textbook of Medical Physiology, Ch. 18 · Medical Physiology (Boron & Boulpaep), Ch. 23 · Costanzo Physiology, 7th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.