Scalp antomy
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
Reading File
Reading File
I now have comprehensive content from multiple authoritative sources. Let me compile the full answer.
Scalp Anatomy
The scalp is the soft tissue covering of the cranial vault. It is a multilayered structure with important clinical implications for surgery, trauma management, and infection.
Extent
The scalp extends:
- Anteriorly: from the supraorbital ridges
- Posteriorly: to the external occipital protuberance / superior nuchal line
- Laterally: down to the zygomatic arch and external acoustic meatus, blending with the temporalis fascia
The Five Layers (Mnemonic: SCALP)
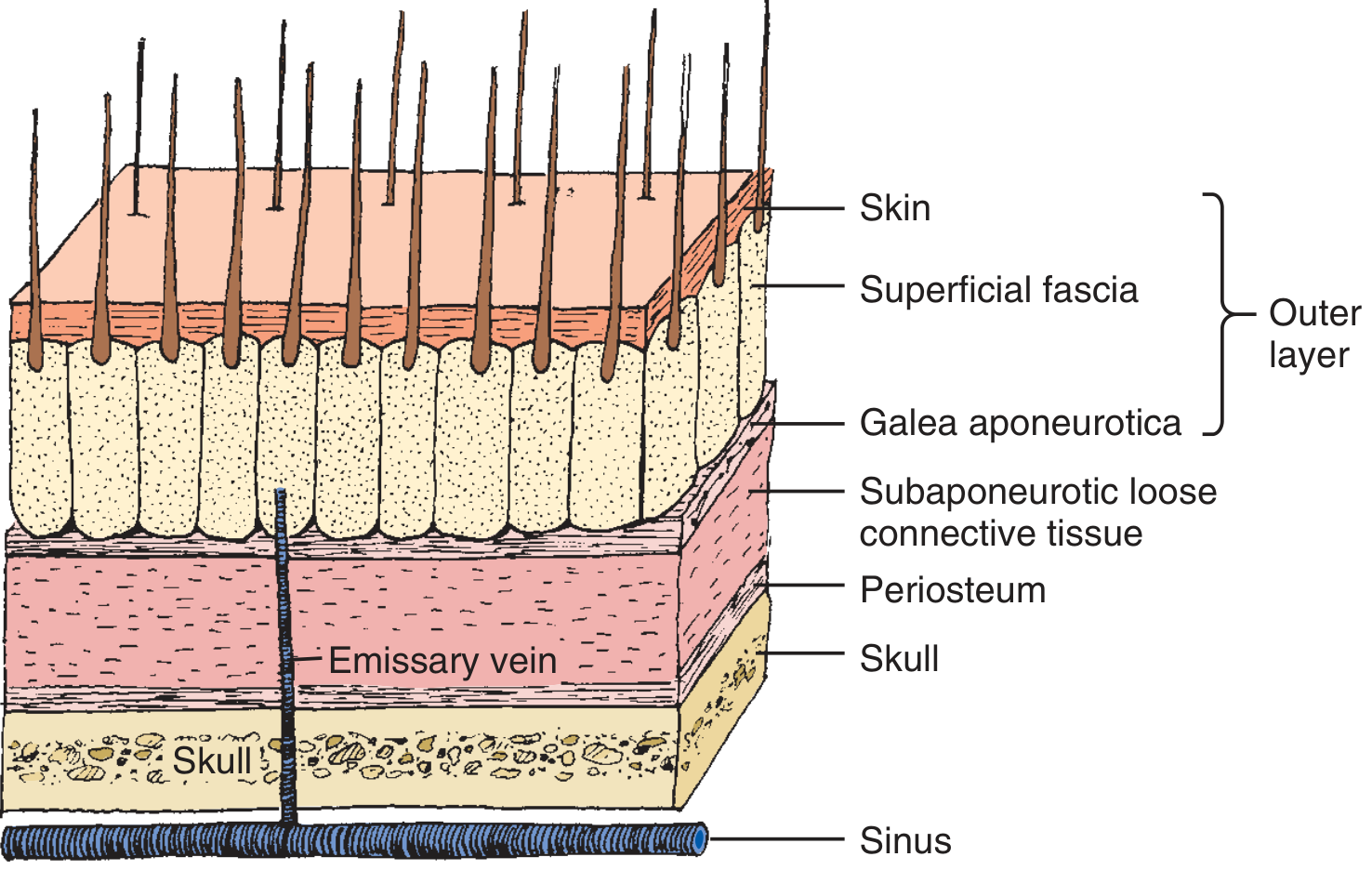
| Layer | Details |
|---|---|
| S - Skin | Thick, hair-bearing; contains sebaceous glands, hair follicles, and sweat glands. The densest hair follicle region of the body. |
| C - Connective tissue (Subcutaneous) | Dense fibro-adipose tissue firmly tethered to both the skin above and the galea below by inelastic fibrous septa. Blood vessels run within this layer - this is the primary source of profuse bleeding in scalp wounds. |
| A - Aponeurosis (Galea aponeurotica) | The epicranial aponeurosis, connecting the frontalis muscle anteriorly and occipitalis posteriorly. Inelastic and tough. Transection of the galea causes wounds to gape open. Clinically, the skin + subcutaneous tissue + galea are treated as a single outer layer. |
| L - Loose areolar tissue (Subaponeurotic) | The "danger space." Contains emissary veins that drain through diploic channels into the intracranial venous sinuses. Allows infection to spread intracranially (osteomyelitis, meningitis, brain abscess). Permits the outer layers to slide freely over the skull - hematomas here spread widely. |
| P - Pericranium (Periosteum) | Tightly adherent to the outer skull surface. Thin and flimsy - cannot be sutured. Continues into sutures of the skull as the endosteum. |
Coronal Section with Deeper Relations
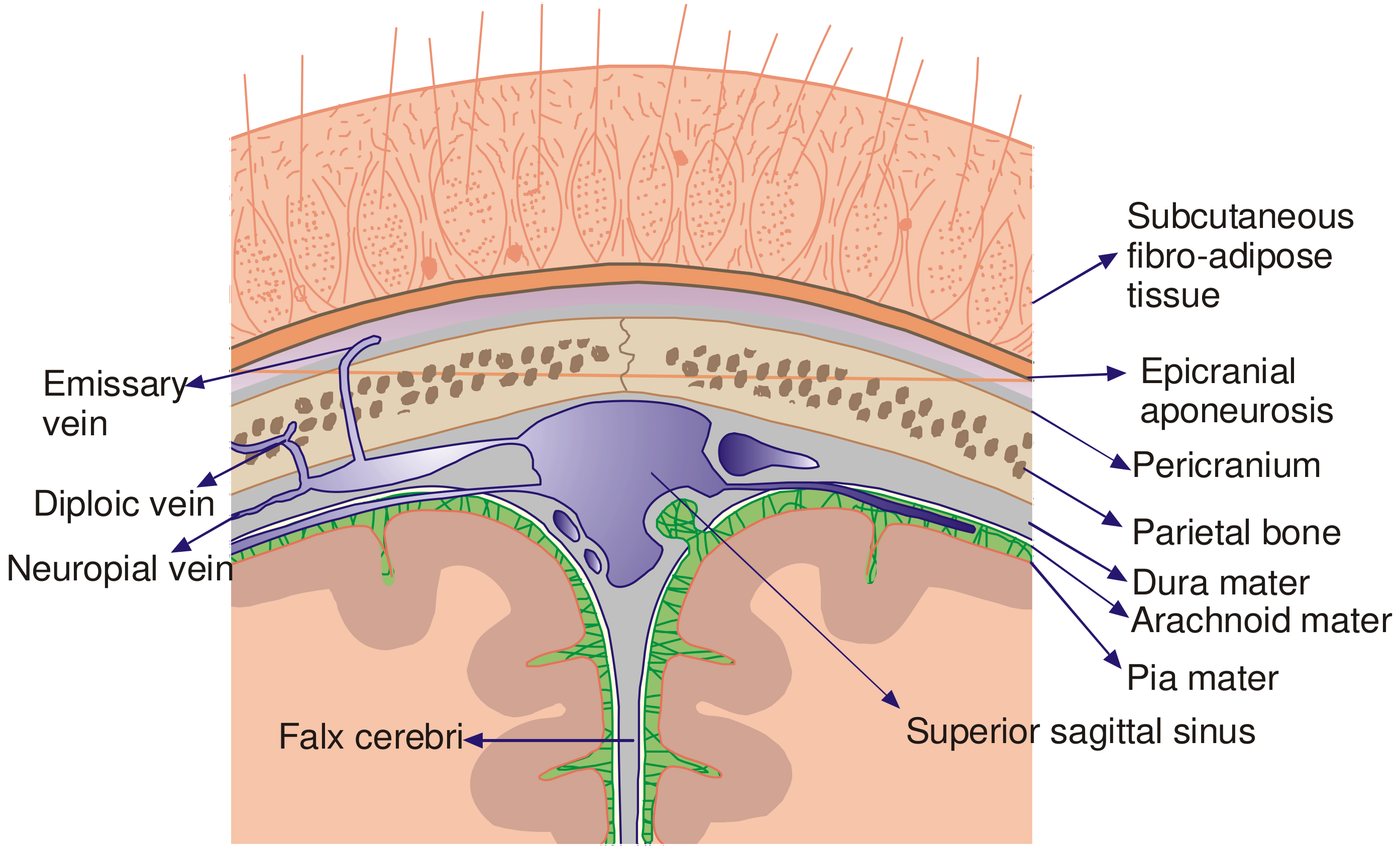
The emissary veins pass through foramina in the skull and connect the subaponeurotic venous plexus with the diploic veins of the skull and then the intracranial venous sinuses (e.g., the superior sagittal sinus).
Blood Supply
The scalp receives a dual arterial supply from both the internal and external carotid systems, creating a rich anastomotic network:
| Artery | Territory | Origin |
|---|---|---|
| Supraorbital artery | Forehead / anterior scalp | Internal carotid (via ophthalmic a.) |
| Supratrochlear artery | Medial forehead | Internal carotid (via ophthalmic a.) |
| Superficial temporal artery | Lateral scalp, temporal region | External carotid (terminal branch) |
| Posterior auricular artery | Posterior scalp above ear | External carotid |
| Occipital artery | Posterior scalp | External carotid |
The vessels run upward from the base of the scalp and lie within the subcutaneous (connective tissue) layer. Because they are tethered by the fibrous septa, cut vessels cannot retract - this is why scalp wounds bleed profusely and persistently. The dense anastomoses mean flaps and grafts have excellent viability even after pedicle ligation of individual branches.
Nerve Supply (Sensory)
| Nerve | Region supplied | Origin |
|---|---|---|
| Supratrochlear nerve | Medial forehead, anterior scalp | V1 (ophthalmic division, CN V) |
| Supraorbital nerve (superficial + deep divisions) | Forehead, vertex of scalp | V1 (ophthalmic division, CN V) |
| Zygomaticotemporal nerve | Anterior temporal region | V2 (maxillary division, CN V) |
| Auriculotemporal nerve | Lateral scalp, temple | V3 (mandibular division, CN V) |
| Lesser occipital nerve | Lateral occipital scalp | C2 (cervical plexus) |
| Greater occipital nerve | Posterior scalp (major supply) | C2 dorsal ramus |
| Third occipital nerve | Lower occipital region | C3 dorsal ramus |
The deep division of the supraorbital nerve runs between the galea and the periosteum, which is important during forehead dissection and flap elevation.
Motor Supply
The scalp musculature (frontalis, occipitalis) is innervated by CN VII (facial nerve):
- Frontalis: temporal branch of facial nerve
- Occipitalis: posterior auricular branch of facial nerve
Clinical Significance
-
Profuse bleeding from lacerations: Vessels in the subcutaneous layer are tethered and cannot retract. Compression and early suturing (rather than vessel ligation) is the preferred hemostasis method.
-
Gaping wounds = galea transection: A non-gaping scalp wound has an intact galea and can be closed superficially. A gaping wound means the galea is cut and must be separately sutured to achieve hemostasis and prevent infection spread.
-
"Dangerous area" / subaponeurotic space: Infections, pus, or hematomas in this loose areolar layer can spread freely across the entire vault (from the orbital margin to the nuchal line). Emissary veins in this layer provide a route for intracranial spread.
-
Temporal lacerations: Heal poorly because the temporalis fascia offers rigid resistance to the galea, making wide mobilization for closure difficult.
-
Scalp avulsions: The loose areolar layer is the plane along which the outer three layers (skin + SQ tissue + galea) peel away from the skull in degloving injuries.
-
Bruise migration: A subgaleal hematoma can track anteriorly into the orbit (giving periorbital bruising) or laterally behind the ear, appearing remote from the actual injury site.
Sources: Roberts and Hedges' Clinical Procedures in Emergency Medicine, p. 813-814 | P.C. Dikshit Textbook of Forensic Medicine and Toxicology, p. 192 | Scott-Brown's Otorhinolaryngology Head & Neck Surgery | Dermatology 2-Volume Set 5e
This is a shared conversation. Sign in to Orris to start your own chat.