Give me details about respiratory system of human body
Reading File
Finding Sources
Finding Sources
Searching the Web
human respiratory system anatomy physiology overview
Reading File
Reading File
Finding Sources
Finding Sources
Loading Image
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
I now have comprehensive content from authoritative textbooks. Let me compile the full detailed response.
The Human Respiratory System
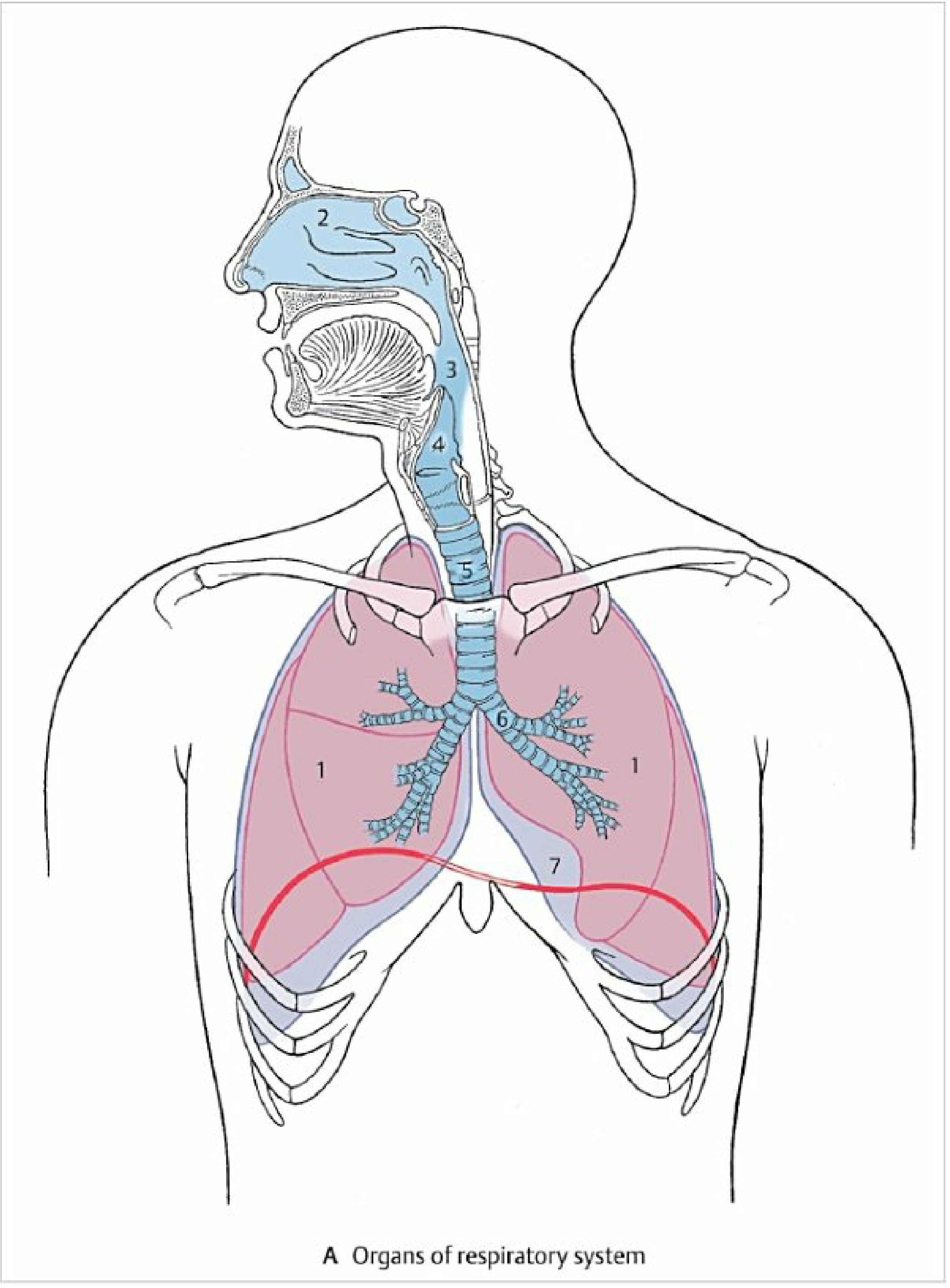
Organs of the respiratory system showing the conducting pathway from nasal cavity (2), pharynx (3), larynx (4), trachea (5), bronchial tree (6), lungs (1), and diaphragm (7) - Color Atlas of Human Anatomy, Vol. 2
Overview
The primary task of the respiratory system is "external respiration": extracting oxygen (O₂) from air and releasing carbon dioxide (CO₂) from the blood. It consists of two main components:
- Surfaces for gas exchange - the combined surface area of all pulmonary alveoli (~200 m²)
- Conducting airways - passages that transport air to those surfaces
Along the way, inhaled air is filtered, humidified, and warmed before reaching the gas-exchange region. The respiratory system also supports vocalization (via the larynx), olfactory perception (via the nasal epithelium), and immune defense.
- Color Atlas of Human Anatomy, Vol. 2, Internal Organs
Anatomical Division
The respiratory system is clinically divided into upper and lower airways:
| Division | Structures |
|---|---|
| Upper airways | Nasal cavities, paranasal sinuses, pharynx (and larynx above the vocal cords) |
| Lower airways | Larynx below the vocal cords, trachea, bronchial tree, alveoli |
1. Upper Respiratory Tract
Nasal Cavity & Paranasal Sinuses
- The airway begins at the nasal cavity, lined with pseudostratified ciliated columnar epithelium (respiratory epithelium) with goblet cells that secrete mucus
- Paranasal sinuses are pneumatized (air-filled) spaces within cranial bones (frontal, sphenoid, ethmoid, maxillary) that open into the nasal cavity
- Functions: filter large particles, warm and humidify air, olfaction
Pharynx
- A muscular tube behind the nasal and oral cavities
- Divided into nasopharynx (above), oropharynx (middle), and laryngopharynx (below)
- The respiratory and alimentary (food) passages intersect here - the epiglottis guards the airway during swallowing
Larynx
- Located in the neck; contains the vocal folds (cords) supported by the thyroid and cricoid cartilages
- Produces voice during phonation
- The epiglottis flaps down to protect the airway during swallowing
- Below the vocal cords, the larynx becomes part of the lower airway
2. Lower Respiratory Tract
Trachea
- A rigid tube ~10-12 cm long, reinforced by 16-20 C-shaped cartilaginous rings (open posteriorly, where the esophagus lies)
- Lined with ciliated pseudostratified columnar epithelium and mucus-secreting goblet cells
- Divides at the carina (at the level of the sternal angle, T4/T5) into the right and left main bronchi
Bronchial Tree
The trachea branches in a progressively bifurcating pattern - 23 generations total:
| Generation | Structure |
|---|---|
| 0 | Trachea |
| 1 | Right and left main (primary) bronchi |
| 2-4 | Lobar and segmental bronchi |
| 5-16 | Smaller bronchi → bronchioles → terminal bronchioles |
| 17-23 | Respiratory bronchioles → alveolar ducts → alveolar sacs |
The walls of conducting airways contain smooth muscle with dual autonomic innervation:
-
Sympathetic (β₂ receptors): relaxation → bronchodilation (e.g., salbutamol/albuterol works here)
-
Parasympathetic (muscarinic receptors): contraction → bronchoconstriction
-
Costanzo Physiology, 7th Edition
Lungs
- Two lungs housed in the thorax within separate pleural cavities, each lined by a serous pleural membrane
- Right lung: 3 lobes (upper, middle, lower) separated by horizontal and oblique fissures
- Left lung: 2 lobes (upper, lower) separated by the oblique fissure; the cardiac notch and lingula accommodate the heart
- The mediastinum lies between the two lungs and contains the heart, great vessels, trachea, esophagus, and lymph nodes
- Each lung's hilum is where the main bronchus, pulmonary artery, and pulmonary veins enter/exit
3. The Respiratory Zone (Gas Exchange Units)
The respiratory zone includes structures lined with alveoli:
- Respiratory bronchioles (transitional - have both cilia and some alveoli)
- Alveolar ducts (completely lined with alveoli, no cilia)
- Alveolar sacs and alveoli
Key alveolar facts:
- ~300 million alveoli per lung
- Each alveolus is ~200 micrometers in diameter
- Combined surface area ~200 m² for gas exchange
- Walls are extremely thin to allow rapid diffusion
Alveolar cell types:
| Cell | Function |
|---|---|
| Type I pneumocytes | Thin squamous cells; main surface for gas exchange |
| Type II pneumocytes | Synthesize pulmonary surfactant (reduces surface tension, prevents alveolar collapse); have regenerative capacity for both cell types |
| Alveolar macrophages | Phagocytose dust, debris, and pathogens; migrate to bronchioles for clearance via cilia |
- Costanzo Physiology, 7th Edition
4. Lung Volumes and Capacities
| Volume/Capacity | Abbreviation | Typical Value | Description |
|---|---|---|---|
| Tidal Volume | TV | 500 mL | Air breathed in/out per normal breath |
| Inspiratory Reserve Volume | IRV | 3,000 mL | Extra air that can be inhaled after normal inspiration |
| Expiratory Reserve Volume | ERV | 1,200 mL | Extra air that can be forced out after normal expiration |
| Residual Volume | RV | 1,200 mL | Air remaining in lungs after maximal expiration (cannot be exhaled) |
| Total Lung Capacity | TLC | ~5,900 mL | All volumes combined |
| Vital Capacity | VC | ~4,700 mL | TV + IRV + ERV (maximum breathable range) |
| Functional Residual Capacity | FRC | ~2,400 mL | ERV + RV (volume at rest after normal expiration) |
| Inspiratory Capacity | IC | ~3,500 mL | TV + IRV |
Dead space - the ~150 mL conducting airway volume does NOT participate in gas exchange (anatomic dead space). Of a 500 mL tidal volume, only ~350 mL actually reaches the alveoli.
- Goldman-Cecil Medicine; Costanzo Physiology
5. Mechanics of Breathing
Inspiration (Active process)
- The diaphragm (primary muscle, innervated by phrenic nerve C3-C5) contracts and flattens downward
- External intercostal muscles elevate the rib cage, expanding thoracic volume
- As thoracic volume increases, intrapleural pressure becomes more negative → lungs expand → alveolar pressure drops below atmospheric → air flows in
Expiration (Passive at rest)
- Elastic recoil of the lung tissue and chest wall drives air out
- Forced expiration uses internal intercostal muscles and abdominal muscles
Compliance
- Lungs resist stretching - their compliance (ease of stretching) is inversely related to their elastance (elastic recoil)
- Surfactant from Type II pneumocytes reduces surface tension in alveoli, dramatically increasing compliance and preventing alveolar collapse on expiration
- Costanzo Physiology, 7th Edition
6. Gas Exchange
Gas exchange occurs by passive diffusion across the alveolar-capillary membrane, driven by partial pressure gradients:
| Gas | Alveolar air | Pulmonary capillary (venous) | Direction of diffusion |
|---|---|---|---|
| O₂ | ~100 mmHg | ~40 mmHg | Alveolus → Blood |
| CO₂ | ~40 mmHg | ~46 mmHg | Blood → Alveolus |
Alveolar gas equation (predicts alveolar PO₂):
PAO₂ = PIO₂ - PACO₂/R (R = respiratory quotient ~0.8)
Ventilation/Perfusion (V/Q) matching is critical - alveoli must be both ventilated AND perfused. Mismatches (ventilated but not perfused = dead space; perfused but not ventilated = shunt) impair gas exchange. Normal V/Q ratio ≈ 0.8.
- Costanzo Physiology, 7th Edition; Murray & Nadel's Textbook of Respiratory Medicine
7. Oxygen and CO₂ Transport in Blood
Oxygen Transport
- ~98.5% bound to hemoglobin (Hb) as oxyhemoglobin (HbO₂) - each Hb carries 4 O₂ molecules
- ~1.5% dissolved in plasma
- The oxyhemoglobin dissociation curve (S-shaped) describes the relationship between PO₂ and Hb saturation
Factors shifting the curve right (decreased O₂ affinity → more O₂ unloaded to tissues):
- Increased temperature, CO₂, H⁺ (lower pH), 2,3-DPG
CO₂ Transport
- ~70% as bicarbonate (HCO₃⁻) in plasma (via carbonic anhydrase in RBCs)
- ~20-23% bound to hemoglobin as carbaminohemoglobin
- ~7% dissolved in plasma
8. Control of Breathing
Breathing is regulated by an automatic neural system with two control centers:
| Center | Location | Function |
|---|---|---|
| Automatic control | Medulla oblongata + pons | Generates rhythmic breathing; responds to blood chemistry |
| Voluntary control | Cerebral cortex | Allows conscious override (talking, breath-holding, etc.) |
The Rhythm Generator
- The pre-Bötzinger complex (pre-BÖTC) in the medulla contains pacemaker cells that discharge rhythmically to drive respiration
- Motor output travels via:
- Phrenic nerve (C3-C5) → diaphragm
- Thoracic spinal nerves → intercostal muscles
Chemoreceptors (Feedback control)
| Type | Location | Stimulus |
|---|---|---|
| Central chemoreceptors | Medulla (near ventral surface) | ↑ CO₂ / ↓ pH of CSF - primary drive to breathe |
| Peripheral chemoreceptors | Carotid & aortic bodies | ↓ PO₂, ↑ PCO₂, ↓ pH in arterial blood |
Key principle: CO₂ (via its effect on CSF pH) is the dominant chemical stimulus for breathing. Hypoxia is a secondary, weaker stimulus except at high altitudes or in chronic lung disease.
- Ganong's Review of Medical Physiology, 26th Edition
9. Additional Functions of the Respiratory System
Beyond gas exchange, the respiratory system serves:
- Vocalization - the larynx and adjacent structures produce sound
- Olfaction - olfactory receptors in the nasal epithelium detect smell
- Immune defense - mucociliary clearance, alveolar macrophages, IgA secretion in airways
- Acid-base regulation - altering ventilation rate rapidly changes blood CO₂ and therefore blood pH
- Thermoregulation - minor heat loss via exhaled air
Summary
The human respiratory system is a highly organized network spanning from the nasal cavity to ~300 million microscopic alveoli. Its conducting airways (nose → trachea → bronchioles) filter and condition air, while the respiratory zone (alveolar surfaces covering ~200 m²) performs the critical exchange of O₂ and CO₂. Breathing is driven by the diaphragm and intercostal muscles under tight neural control from the medullary pre-Bötzinger complex, with continuous chemical feedback from central and peripheral chemoreceptors responding primarily to CO₂ levels in the blood.
Sources: Costanzo Physiology, 7th Edition | Color Atlas of Human Anatomy, Vol. 2 | The Developing Human - Clinically Oriented Embryology | Ganong's Review of Medical Physiology, 26th Edition | Goldman-Cecil Medicine | Murray & Nadel's Textbook of Respiratory Medicine
This is a shared conversation. Sign in to Orris to start your own chat.