Ureterocele
Reading File
Finding Sources
Searching PubMed
ureterocele management pediatric
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive content from Campbell-Walsh Wein Urology, Smith & Tanagho's General Urology, and Bailey & Love's Surgery, plus an excellent diagram and recent meta-analysis data. Let me compile the full answer.
Ureterocele
Definition
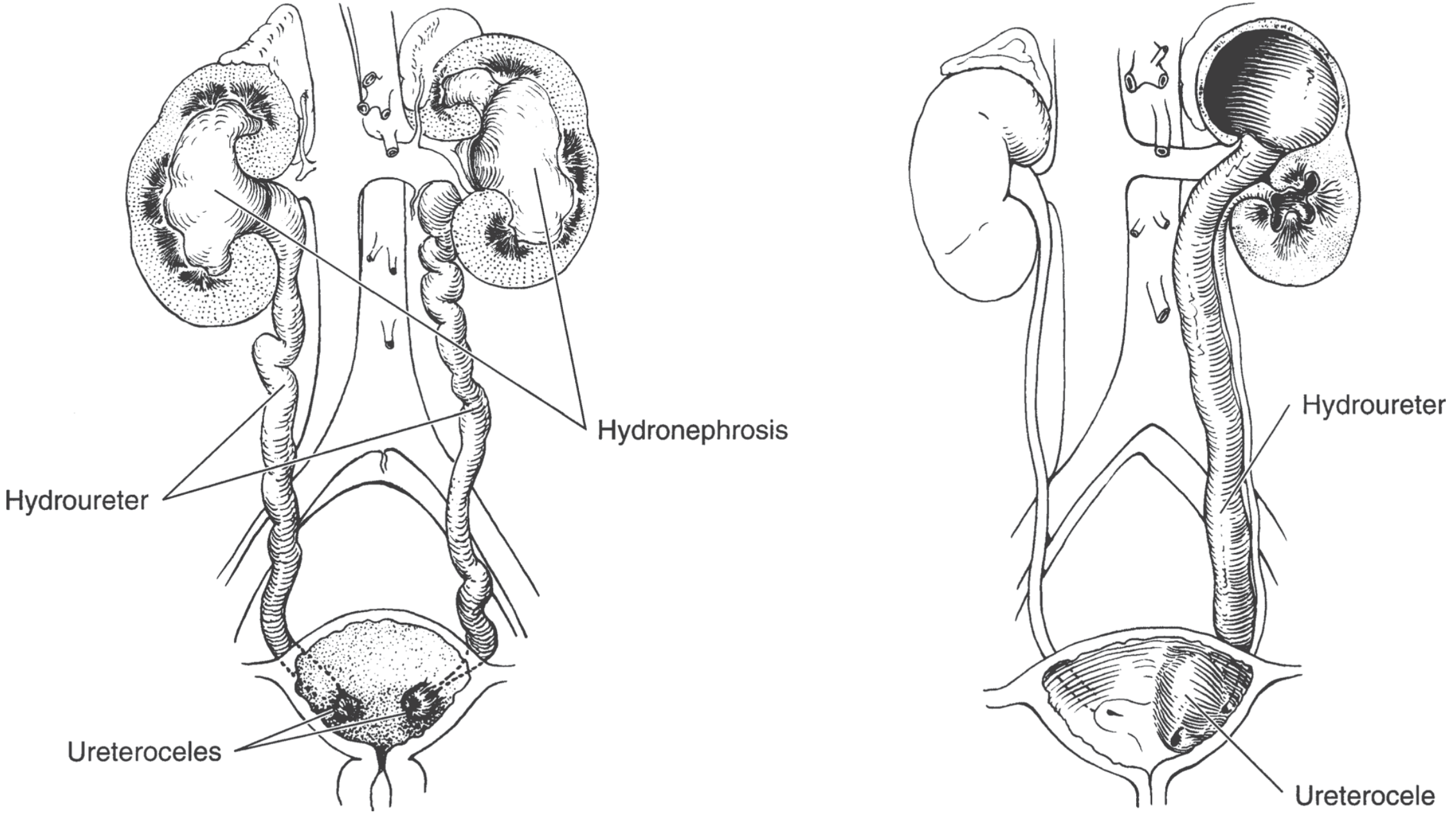
A ureterocele is a cystic dilation (sacculation) of the distal (intramural) portion of the ureter. The expansion forms between the superficial and deep muscle layers of the trigone and may lie entirely within the bladder or extend across the bladder neck into the urethra. - Smith and Tanagho's General Urology, 19th ed.
Epidemiology
| Feature | Detail |
|---|---|
| Sex ratio | 7:1 female predominance (Bailey & Love: 4:1) |
| Bilateral | ~10% of cases |
| Associated with duplex system | Ectopic ureteroceles nearly always involve the upper pole ureter of a duplex kidney |
| Ectopic vs intravesical | Ectopic ureteroceles are 4x more common than intravesical ones |
- Smith and Tanagho's General Urology, 19th ed.
Embryology / Pathogenesis
Ureterocele results from delayed or incomplete canalization of the ureteral bud, leading to early prenatal obstruction and expansion of the ureteral bud prior to its absorption into the urogenital sinus. This is considered a variant of ectopic ureter pathogenesis, involving defective ureterotrigonal connections and associated renal maldevelopment. - Campbell-Walsh-Wein Urology
Classification
The most clinically useful classification separates two types:
1. Intravesical (Orthotopic) Ureterocele
- Entirely within the bladder, above the bladder neck
- More often associated with a single ureter (and more common in boys when single)
- May be non-obstructive ("simple") or cause significant obstruction
2. Ectopic Ureterocele
- Some portion is situated permanently at the bladder neck or urethra
- Orifice may be in the bladder, at the bladder neck, or within the urethra
- Nearly always associated with the upper pole of a duplicated system
Stephens' Subtypes (additional detail)
-
Stenotic - narrow orifice
-
Sphincteric - orifice at the level of the sphincter
-
Sphincterostenotic - both stenotic and sphincteric
-
Blind - no orifice
-
Nonobstructed - open orifice
-
Cecoureterocele - orifice is within the bladder, but the cavity of the ureterocele extends submucosally beyond the bladder neck into the urethra (surgically challenging)
-
Campbell-Walsh-Wein Urology
Pathophysiology / Consequences
Large ureteroceles can:
- Cause significant hydroureteronephrosis (nearly always present)
- Displace adjacent ureteric orifices
- Interfere with the muscular backing of the bladder
- Obstruct the bladder neck (causing bladder outlet obstruction)
- Obstruct the contralateral ureteric orifice
- Lead to upper pole dysplasia in ectopic ureteroceles associated with duplex systems
- Prolapse through the female urethra (rare)
Clinical Presentation
Historically patients presented with:
- Urinary tract infection (most common in childhood)
- Bladder outlet obstruction
- Incontinence
- Rarely, prolapse of the ureterocele through the urethra
Today, most cases are diagnosed on antenatal maternal ultrasound. - Smith and Tanagho's General Urology, 19th ed.
Diagnosis / Imaging
| Investigation | Findings |
|---|---|
| Antenatal / postnatal ultrasound | Hydronephrosis (upper pole), dilated ureter, cystic structure in bladder |
| VCUG (voiding cystourethrogram) | Demonstrates reflux into lower pole ureter, contralateral ureter, or ruptured ureterocele |
| Intravenous urogram (IVU) | Classic "cobra head" sign (filling defect with halo around ureterocele orifice) |
| Renal scan (DMSA / MAG3) | Estimates differential renal function; guides therapy |
The combination of imaging findings is critical for surgical planning. - Smith and Tanagho's General Urology, 19th ed.
Cobra head sign on IVU is pathognomonic - a rounded filling defect surrounded by a radiolucent halo caused by the ureterocele wall.
Treatment
Treatment must be individualized based on:
- Anatomic type (intravesical vs ectopic)
- Associated system (single vs duplex)
- Degree of hydroureteronephrosis
- Residual upper pole renal function
- Patient age
Endoscopic Incision (First-line / Minimally invasive)
- Transurethral incision is recognized as the definitive procedure in many instances
- Preferred especially for intravesical ureteroceles and as the initial approach in neonates
- Risk: may create vesicoureteric reflux post-incision (~50% rate, per meta-analyses)
- A 2024 meta-analysis (PMID 38705762) examined surgical patterns in endoscopic management of pediatric ureteroceles
Open Surgery (when endoscopic approach is insufficient)
Options based on anatomy and function:
| Procedure | Indication |
|---|---|
| Heminephrectomy + ureterectomy | Non-functioning / dysplastic upper pole |
| Ureterocele excision + ureteral reimplantation | Functioning upper pole with significant reflux or obstruction |
| Upper pole ureteral ligation (laparoscopic) | Can be done with minimal morbidity |
| Vesical reconstruction | If bladder anatomy is significantly distorted |
More than one procedure may be required in complex cases. - Smith and Tanagho's General Urology, 19th ed. and Bailey and Love's Surgery, 28th ed.
Key Points Summary
| Feature | Details |
|---|---|
| Definition | Cystic dilation of distal ureter |
| Most common type | Ectopic (4x more common than intravesical) |
| Association | Upper pole of duplex kidney |
| Sex predominance | Female (7:1) |
| Diagnosis | Antenatal USS; postnatal USS + VCUG; cobra head on IVU |
| First-line treatment | Endoscopic transurethral incision |
| Complication of incision | Vesicoureteric reflux |
| Non-functioning upper pole | Heminephrectomy |
Recent evidence (2024-2025): A systematic review and meta-analysis (PMID 38705762) on endoscopic management patterns (2024) and another meta-analysis on voiding dysfunction risk in children with ureteroceles (PMID 40707301) (2025) are the latest high-level evidence on outcomes - no major departures from the above guidelines were identified.
This is a shared conversation. Sign in to Orris to start your own chat.