Hydrocele
Reading File
Finding Sources
Searching PubMed
hydrocele
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have excellent material for a comprehensive answer. Let me compile it.
Hydrocele
A hydrocele is an abnormal collection of serous fluid within a part of the processus vaginalis - most commonly the tunica vaginalis surrounding the testis, and occasionally along the spermatic cord.
Epidemiology
- Affects approximately 1% of adult men
- More than 80% of newborn boys have a patent processus vaginalis at birth
- Most close spontaneously within 18 months of age
- Primary (idiopathic) hydroceles are most common; secondary hydroceles typically occur in men >40 years
Embryology & Pathophysiology
The processus vaginalis is a diverticulum of the peritoneal cavity that descends with the testes into the scrotum via the inguinal canal around the 28th week of gestation, with gradual closure through infancy and childhood.
Fluid accumulates due to excessive production and/or defective absorption by the tunica vaginalis, often from disruption of lymphatic drainage.
Classification
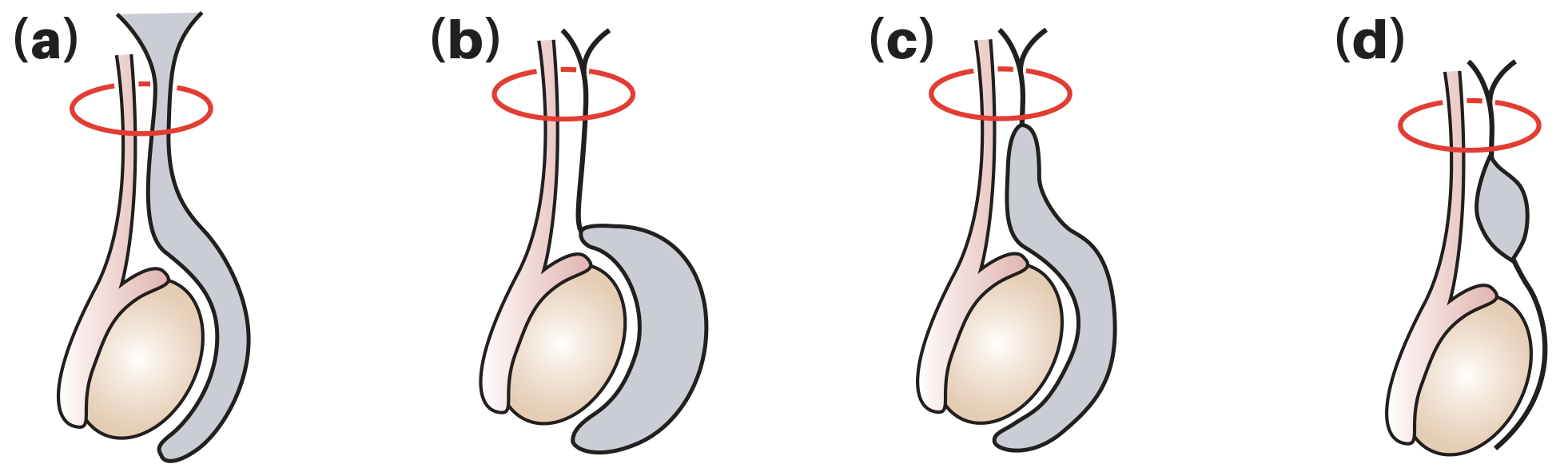
Bailey & Love's, Fig. 86.8: Types of hydrocele
| Type | Description |
|---|---|
| (a) Vaginal (primary/non-communicating) | Processus vaginalis is closed; fluid accumulates within tunica vaginalis due to imbalance in production/absorption. Most common type globally. |
| (b) Infantile hydrocele | Distal processus closes correctly but mid-portion remains patent; proximal end is open, communicating with tunica vaginalis. |
| (c) Congenital (communicating) | Patent processus vaginalis allows free flow of peritoneal fluid into the scrotum; associated with indirect inguinal hernias. |
| (d) Hydrocele of the cord | Both proximal and distal ends of processus close but mid-portion remains patent, forming a cyst along the spermatic cord. |
Abdominoscrotal hydrocele is a rare variant (1.25% of all hydroceles), bilateral in ~30% of cases, where a non-communicating scrotal mass extends upward into the abdomen.
Etiology
Primary (idiopathic): No underlying cause found. Most common in adults.
Secondary: Occurs at any age, may present acutely. Causes include:
- Epididymo-orchitis / infection (including filariasis - major cause globally)
- Testicular torsion
- Trauma
- Testicular neoplasm
- Radiotherapy
Important: If a tumour is suspected, do NOT aspirate the hydrocele - risk of malignant needle-track implantation.
Post-varicocelectomy hydrocele: Complication in 3-33% (average ~7%) of non-microscopic varicocelectomy, caused by lymphatic obstruction. Microsurgical technique almost eliminates this risk.
Filarial hydrocele: Accounts for up to 80% of hydroceles in tropical countries (endemic Wuchereria bancrofti). Follows repeated filarial epididymo-orchitis. May contain chylous fluid (chylocele) from ruptured lymphatic varices.
Clinical Features
Examination should be performed in both upright and supine positions. Ask three key questions:
- Can you get above the swelling? - A hydrocele allows palpation of a normal spermatic cord above it (unlike an inguino-scrotal hernia)
- Are the testis and epididymis palpable? - A hydrocele encloses both structures, making them impalpable
- Does it transilluminate? - Hydroceles are typically brilliantly translucent
Presentation:
- Usually painless scrotal swelling - may reach large size before presentation
- Smooth, fluctuant, tense swelling
- An acute hydrocele in a young man warrants suspicion for testicular tumour
- Congenital hydrocele may be intermittent (fluid drains back to peritoneum when lying flat)
- Hydrocele of the cord - smooth oval swelling above the testis near the cord; moves downward when testis is pulled (differentiates from inguinal hernia)
- Hydrocele of the canal of Nuck - female equivalent; cyst along the round ligament, at least partially within the inguinal canal
Investigations
- Scrotal ultrasound - investigation of choice; valuable when testis/epididymis is impalpable, and to exclude underlying testicular pathology (especially malignancy)
- Fluid analysis if aspirated (protein concentration helps distinguish causes)
Treatment
Conservative
- Small, asymptomatic hydroceles require no treatment
- Congenital hydroceles in infants - watchful waiting; most resolve spontaneously by 18 months
Surgical (main treatment for symptomatic acquired hydroceles)
Three established surgical techniques:
| Procedure | Principle | Indication |
|---|---|---|
| Lord's operation (plication) | Sac is gathered and sutured with multiple radial stitches without excision | Thin-walled sac; minimal dissection, reduced haematoma risk |
| Jaboulay's procedure (eversion) | Sac is everted and sutured behind the epididymis (bottleneck suture) | Moderate-thickness sac; most widely used |
| Excision | Sac is excised and edges oversewn | Thick-walled or recurrent hydrocele; highest haematoma risk |
- Congenital hydroceles are treated by herniotomy (ligation of patent processus vaginalis) through an inguinal incision
- In infants, surgery is deferred unless the hydrocele persists beyond 2 years or enlarges
Aspiration
- Simple but fluid always reaccumulates within days to weeks
- Reserved for men unfit for surgery (can be done under local anaesthetic)
- Risk of haematocele formation
- Sclerotherapy (e.g., tetracycline injection) may be added - effective but painful
Filarial/Chylocele
- Acute: rest and aspiration
- Chronic: excision of the sac
Differential Diagnosis of Scrotal Swelling
| Feature | Hydrocele | Epididymal cyst | Varicocele | Inguinoscrotal hernia | Testicular tumour |
|---|---|---|---|---|---|
| Can get above | Yes | Yes | Yes | No | Yes |
| Transillumination | Bright | Bright | No | No | No |
| Relation to testis | Surrounds testis | Separate from testis | Above/behind testis | Separate | Part of testis |
Key Points
- Hydroceles surround the testis and transilluminate brightly
- Ultrasound is essential when testis/epididymis is impalpable
- Testicular malignancy is an uncommon but important secondary cause - exclude by ultrasound
- Surgery is the mainstay of treatment for symptomatic cases
- Never aspirate if malignancy is suspected
- In tropical regions, filariasis (W. bancrofti) is the dominant cause
Sources: Bailey and Love's Short Practice of Surgery, 28th Ed., Ch. 86; Campbell-Walsh-Wein Urology, Ch. 37, 44; Mulholland & Greenfield's Surgery, 7th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.