Vitamin A by satynarayan
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I now have comprehensive information from Lippincott Biochemistry, Harper's Biochemistry, and Robbins Pathology. Note that Satynarayan's biochemistry textbook is not in the library, but the content below is from equivalent authoritative biochemistry textbooks covering all the same topics that Satynarayan covers. Let me now compile the complete answer.
Vitamin A (Retinol)
Note: Satynarayan's Biochemistry is not in the library database, but the following is a complete, exam-oriented coverage of Vitamin A drawn from Lippincott Illustrated Reviews: Biochemistry (8th ed), Harper's Illustrated Biochemistry (32nd ed), and Robbins & Kumar Basic Pathology - all covering identical content.
1. Nature and Classification
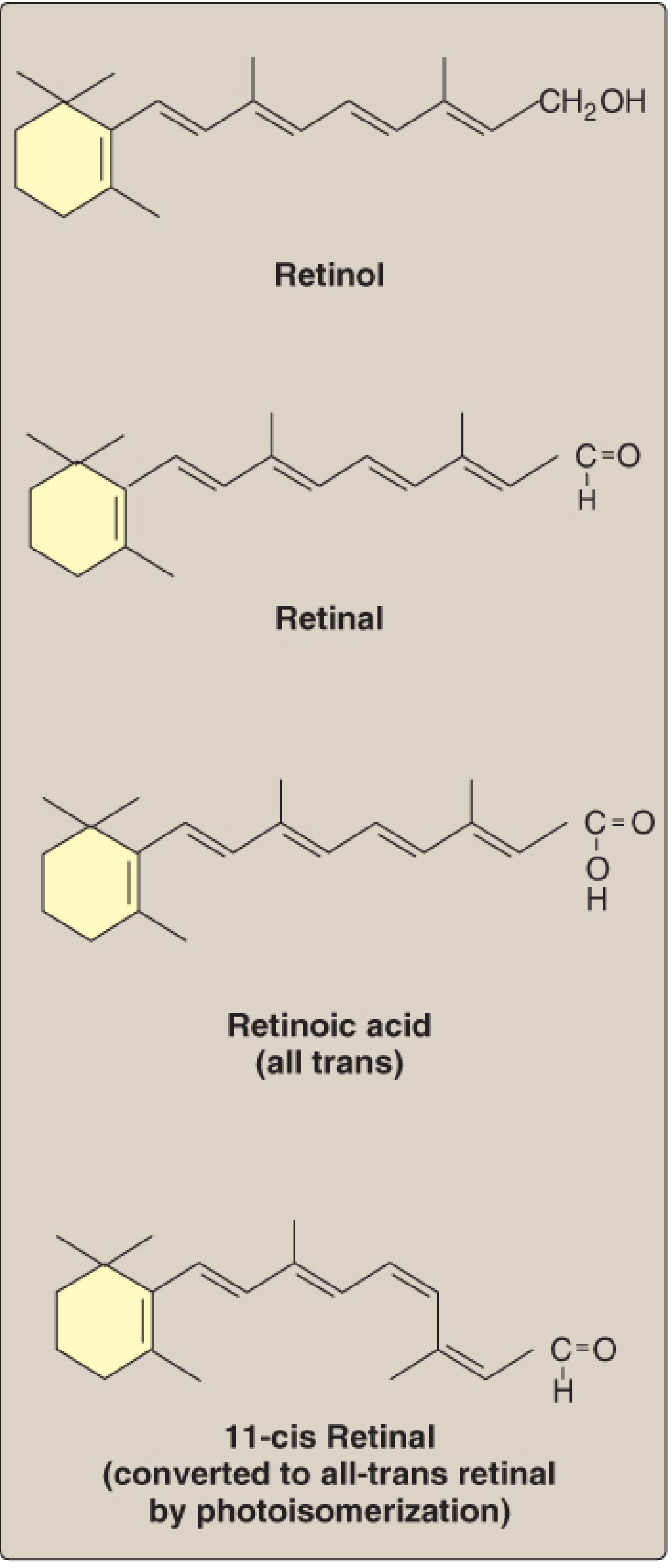
Vitamin A is a fat-soluble vitamin. The term "retinoids" encompasses all natural and synthetic compounds with vitamin A activity. Two groups of compounds have Vitamin A activity:
Group 1 - Preformed Vitamin A (Retinoids) - found only in animal-origin foods:
- Retinol - the primary alcohol form; the transport and storage form (as retinyl ester)
- Retinal (Retinaldehyde) - the aldehyde derived by oxidation of retinol; retinol and retinal are freely interconvertible
- Retinoic acid - the acid derived from further oxidation of retinal; cannot be reduced back to retinal or retinol
Group 2 - Provitamin A (Carotenoids) - found in plant foods:
- β-carotene is the most important; it is symmetrically cleaved in the intestinal mucosa by carotene dioxygenase to yield 2 molecules of retinal
- In practice, conversion is inefficient: 6 μg β-carotene = 1 μg retinol (vitamin A activity is only ~1/12 that of retinol)
- α-carotene, γ-carotene, and cryptoxanthin are also provitamin A carotenoids
Structures of the Retinoids
2. Units and RDA
| Measure | Equivalent |
|---|---|
| 1 IU of Vitamin A | = 0.3 μg retinol |
| 1 μg retinol | = 3.33 IU |
| 1 RAE (Retinol Activity Equivalent) | = 1 μg retinol = 12 μg β-carotene = 24 μg other provitamin A carotenoids |
| RDA (adult males) | 900 RAE/day |
| RDA (adult females) | 700 RAE/day |
3. Dietary Sources
- Animal sources (preformed vitamin A): Liver, fish liver oil, eggs, milk, butter - highest in liver and fish oils
- Plant sources (provitamin A): Yellow/orange vegetables (carrots, sweet potato, squash), dark leafy greens (spinach), yellow fruits
- Carotenoids contribute approximately 30% of dietary vitamin A
4. Absorption and Transport
Digestion and Intestinal Absorption
- Dietary retinyl esters are hydrolyzed by pancreatic enzymes in the intestinal lumen to release retinol + free fatty acids
- β-carotene is cleaved to retinal by carotene dioxygenase in the intestinal mucosa; retinal is reduced to retinol
- Within enterocytes, retinol is re-esterified with long-chain fatty acids to form retinyl esters
- Retinyl esters are packaged into chylomicrons and secreted via lymph into the bloodstream
- Absorption requires bile, pancreatic enzymes, and antioxidants (being fat-soluble)
Transport to Liver and Storage
- Chylomicron remnants (carrying retinyl esters) are taken up by the liver via the apolipoprotein E receptor
- Over 90% of the body's vitamin A is stored in the liver, predominantly as retinyl esters in perisinusoidal stellate (Ito) cells
- Liver reserves are sufficient for at least 6 months in healthy individuals
Release from Liver to Peripheral Tissues
- Retinol is released from the liver bound to Retinol-Binding Protein (RBP), which complexes with transthyretin (TTR) - forming a ternary complex
- This complex binds to cell-surface RBP receptors on peripheral tissues, allowing retinol to enter
- After uptake, RBP is recycled back into the blood
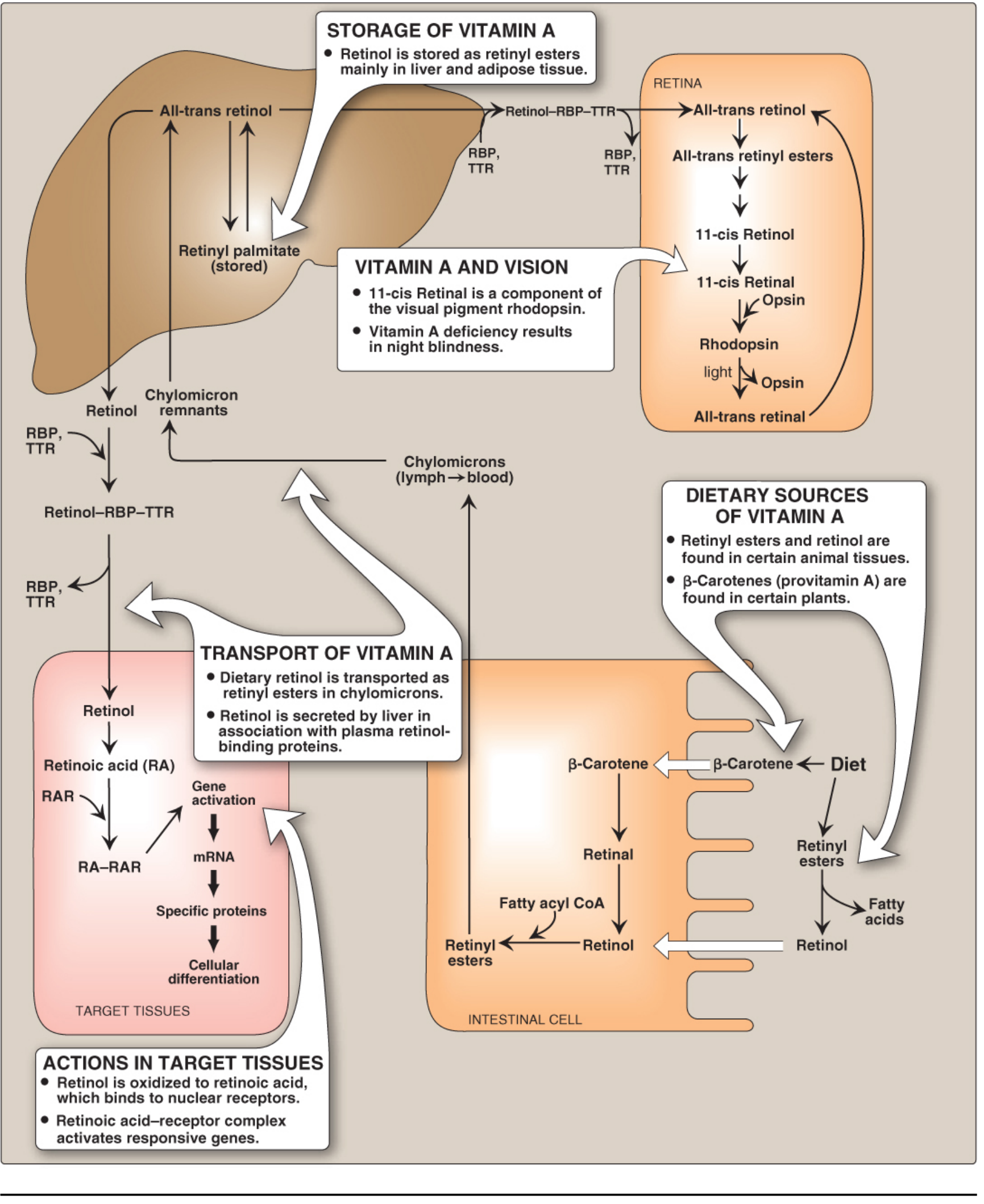
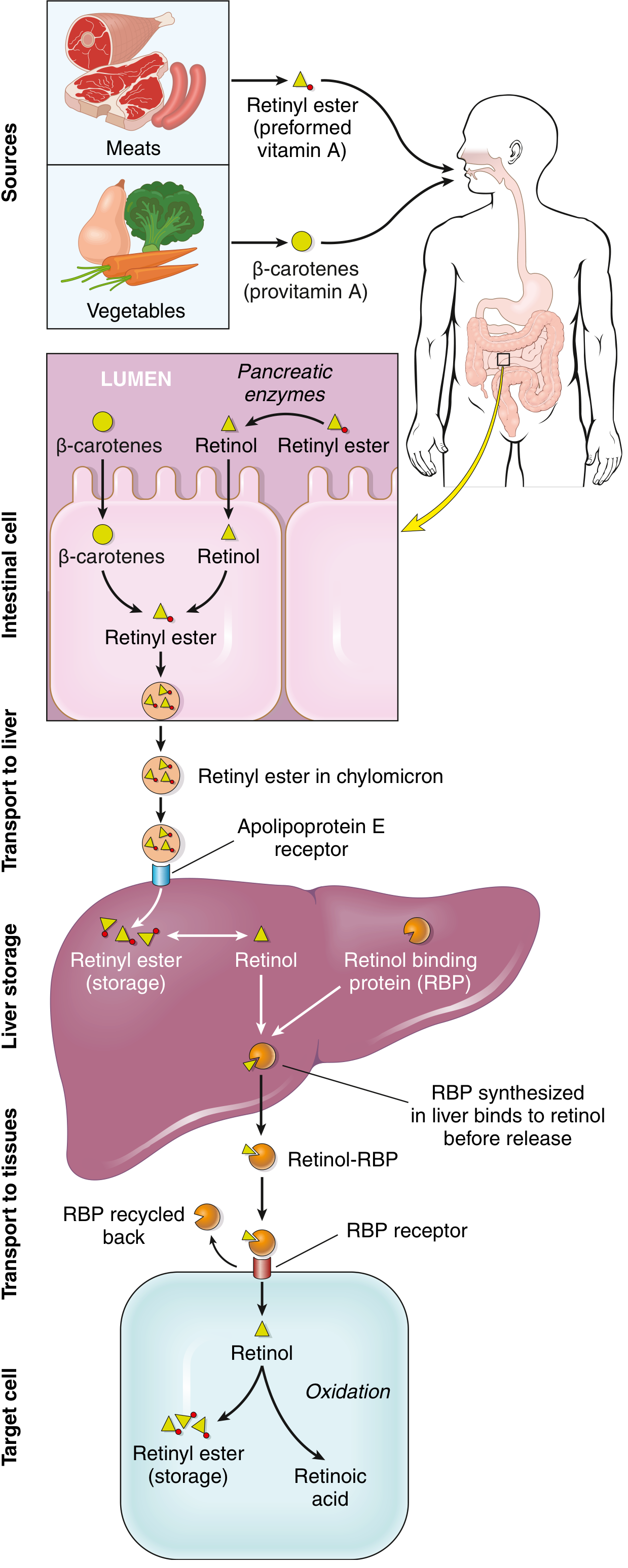
5. Mechanism of Action
- In target tissues, retinol is oxidized to retinoic acid (RA)
- Retinoic acid binds with high affinity to nuclear receptors called Retinoic Acid Receptors (RARs)
- The RA-RAR complex forms a heterodimer with Retinoic X Receptor (RXR)
- RAR/RXR heterodimers bind to Retinoic Acid Response Elements (RAREs) on DNA
- This activates or represses transcription of specific genes - controlling production of proteins that mediate physiologic functions (e.g., keratin gene expression in epithelial cells)
- The RAR superfamily includes receptors for steroid hormones, thyroid hormones, and vitamin D - all functioning similarly
- 9-cis retinoic acid activates RXR, which can also heterodimerize with PPARs (peroxisome proliferator-activated receptors) and vitamin D receptors, mediating metabolic effects
6. Functions of Vitamin A
A. Vision (Visual Cycle)
- Rhodopsin (in rod cells) = 11-cis retinal + opsin protein; most sensitive to dim light
- Iodopsins (3 types in cone cells) = retinal + different opsins, each sensitive to a specific color (red, green, blue)
- Phototransduction: Light isomerizes 11-cis retinal → all-trans retinal, causing conformational change in opsin, activating G protein transducin → triggers nerve impulse → transmitted via optic nerve to brain
- Regeneration: All-trans retinal is reduced to all-trans retinol → esterified → isomerized to 11-cis retinol → oxidized back to 11-cis retinal → recombines with opsin to reform rhodopsin
B. Epithelial Cell Differentiation and Growth
- Vitamin A maintains the differentiation of mucus-secreting columnar epithelium
- In deficiency: normal epithelium undergoes squamous metaplasia (keratinizing metaplasia)
- Retinoids regulate expression of genes encoding growth factor receptors, tumor suppressors, and secreted proteins
- Controls cell growth, differentiation, and cell-cycle regulation
C. Metabolic Effects (via RXR-PPAR heterodimers)
- Retinoids inhibit adipogenesis and stimulate lipid breakdown
- Regulate fatty acid oxidation, adipogenesis, and lipoprotein metabolism
D. Immune Function
- Vitamin A supplementation reduces morbidity from diarrhea by ~15% and mortality by ~30%
- Promotes regeneration of damaged epithelium
- Required for optimal immune function (mechanism not fully elucidated)
E. Reproduction and Growth
- Essential for normal reproduction and fetal development
- Deficiency causes impaired spermatogenesis and fetal resorption
7. Deficiency - Hypovitaminosis A
Causes
- Dietary deficiency (most common worldwide - seen in developing countries)
- Fat malabsorption syndromes: celiac disease, Crohn's disease, colitis
- Bariatric surgery, chronic use of mineral oil laxatives
- Prolonged protein deficiency (RBP is a protein - needed for transport)
Clinical Features
Ocular manifestations (most significant):
| Stage | Manifestation |
|---|---|
| Early | Night blindness (nyctalopia) - earliest sign; impaired dark adaptation |
| Progressive | Xerosis conjunctivae - dryness of conjunctiva (squamous metaplasia replaces lacrimal/mucus epithelium) |
| Progressive | Bitot's spots - buildup of keratin debris as small, foamy, opaque plaques on conjunctiva |
| Advanced | Corneal xerosis and ulceration |
| Severe | Keratomalacia - softening and destruction of the cornea |
| End-stage | Blindness - due to opaque scar tissue formation |
Over 500,000 children worldwide are blinded each year by xerophthalmia from Vitamin A deficiency.
Other manifestations:
- Respiratory tract: Squamous metaplasia of mucociliary epithelium → predisposes to secondary pulmonary infections
- Urinary tract: Squamous metaplasia → desquamation of keratin debris → renal and bladder stones
- Skin: Follicular hyperkeratosis (phrynoderma/toad skin) - hyperkeratinization and plugging of adnexal gland ducts, producing follicular/papular dermatosis
- Growth: Retarded growth and development in children
- Reproductive: Impaired spermatogenesis, infertility
8. Toxicity - Hypervitaminosis A
Both acute and chronic excess can cause toxicity. Beta-carotene excess does NOT cause vitamin A toxicity (it is not efficiently converted).
Acute Toxicity
- Nausea, vomiting, headache
- Blurred vision, vertigo
- Increased intracranial pressure (pseudotumor cerebri)
- Historically described after eating polar bear liver (very high in preformed vitamin A)
Chronic Toxicity
- Dry, scaly skin; hair loss (alopecia); cheilitis
- Hepatotoxicity - liver damage
- Hypercalcemia
- Bone and joint pain; periosteal thickening (cortical hyperostosis)
- Headache from raised intracranial pressure
- Desquamation
Teratogenicity (Critical!)
- Retinoic acid and its synthetic derivatives are potent teratogens
- Excess vitamin A during pregnancy causes retinoid embryopathy: craniofacial defects, heart malformations, CNS defects, thymic aplasia
- Isotretinoin (13-cis retinoic acid) is absolutely contraindicated in pregnancy
- β-carotene does NOT cause teratogenicity
9. Clinical/Therapeutic Uses
| Condition | Agent Used | Route |
|---|---|---|
| Vitamin A deficiency / xerophthalmia | Retinol / retinyl esters | Oral |
| Mild acne, skin aging | Tretinoin (all-trans retinoic acid) | Topical |
| Severe cystic acne (unresponsive to other therapy) | Isotretinoin (13-cis retinoic acid) | Oral |
| Acute promyelocytic leukemia (APL) | Tretinoin (ATRA) | Oral |
| Psoriasis | Acitretin (synthetic retinoid) | Oral |
10. Summary Table
| Feature | Detail |
|---|---|
| Vitamin type | Fat-soluble |
| Active forms | Retinol (transport/storage), Retinal (vision), Retinoic acid (gene regulation) |
| Provitamin | β-carotene (plants) |
| Storage site | Liver (Ito/stellate cells); >90% of body stores |
| Transport protein | RBP (retinol-binding protein) + transthyretin |
| Mechanism | Nuclear receptors (RAR/RXR) → gene transcription |
| Key function | Vision, epithelial differentiation, growth, immunity |
| Earliest deficiency sign | Night blindness (nyctalopia) |
| Severe deficiency | Xerophthalmia → keratomalacia → blindness |
| Skin deficiency sign | Follicular hyperkeratosis (phrynoderma) |
| Toxicity (chronic) | Liver damage, bone pain, alopecia, teratogenicity |
| RDA | 900 RAE (men), 700 RAE (women) |
Sources: Lippincott Illustrated Reviews: Biochemistry 8th ed, p. 1073-1083 | Harper's Illustrated Biochemistry 32nd ed, Ch. 44 | Robbins & Kumar Basic Pathology, p. 292-294
Vitamin D
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
I have all the material needed for a complete, well-illustrated answer. Here it is:
Vitamin D
Content drawn from Lippincott Illustrated Reviews: Biochemistry (8th ed), Harper's Illustrated Biochemistry (32nd ed), and Robbins & Kumar Basic Pathology - the standard biochemistry/pathology references covering the same syllabus as Satynarayan.
1. Nature - "Vitamin D is Really a Hormone"
Vitamin D is a fat-soluble vitamin with hormone-like properties. It is not strictly a vitamin because it can be synthesized endogenously in the skin - under most conditions this is the major source. A dietary requirement only exists when sunlight exposure is inadequate. Its active form, calcitriol (1,25-dihydroxycholecalciferol), acts through nuclear receptors to regulate gene expression, making it functionally a steroid hormone.
2. Forms of Vitamin D
Two dietary forms exist, differing only in a side-chain double bond and methyl group:
| Form | Name | Source |
|---|---|---|
| Vitamin D₂ | Ergocalciferol | Plants (from ergosterol) |
| Vitamin D₃ | Cholecalciferol | Animal tissues; skin synthesis |
Both forms undergo identical hydroxylation steps to become active.
Structure - Sources Diagram
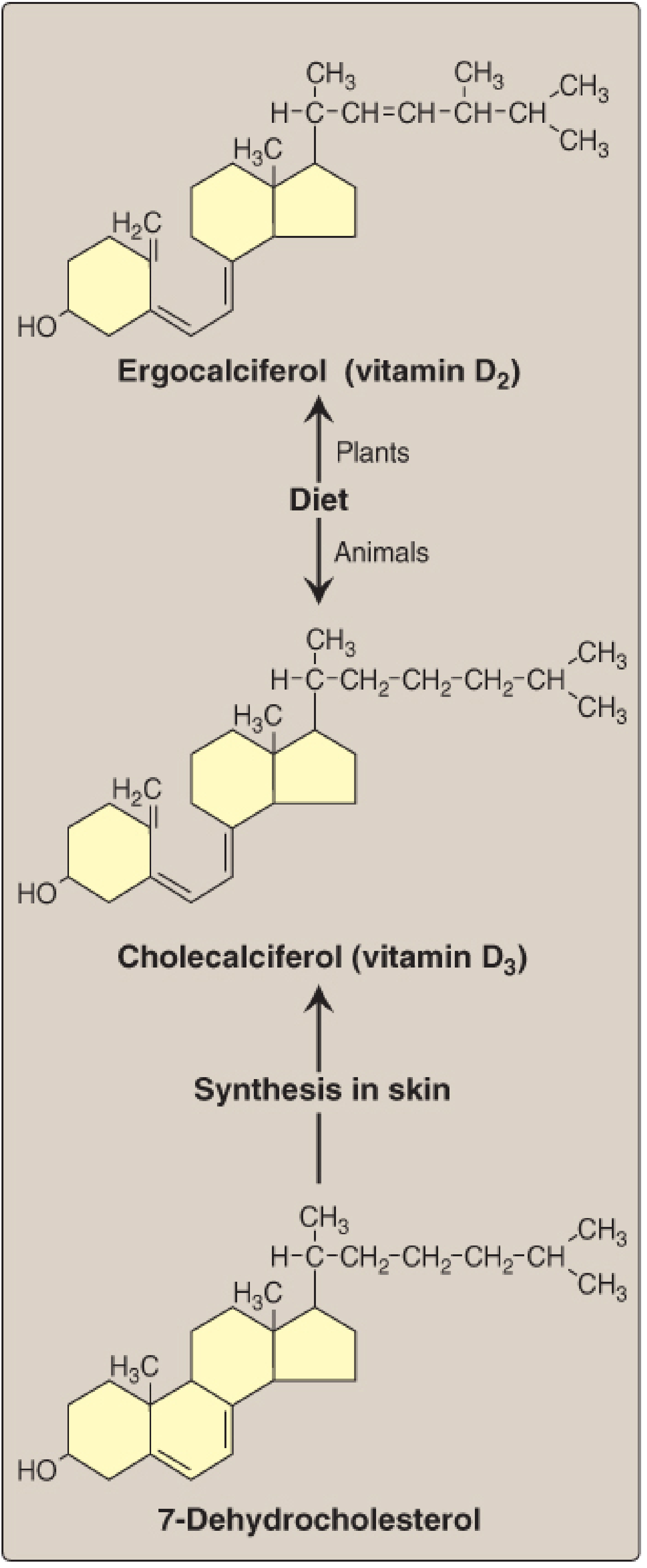
3. Sources
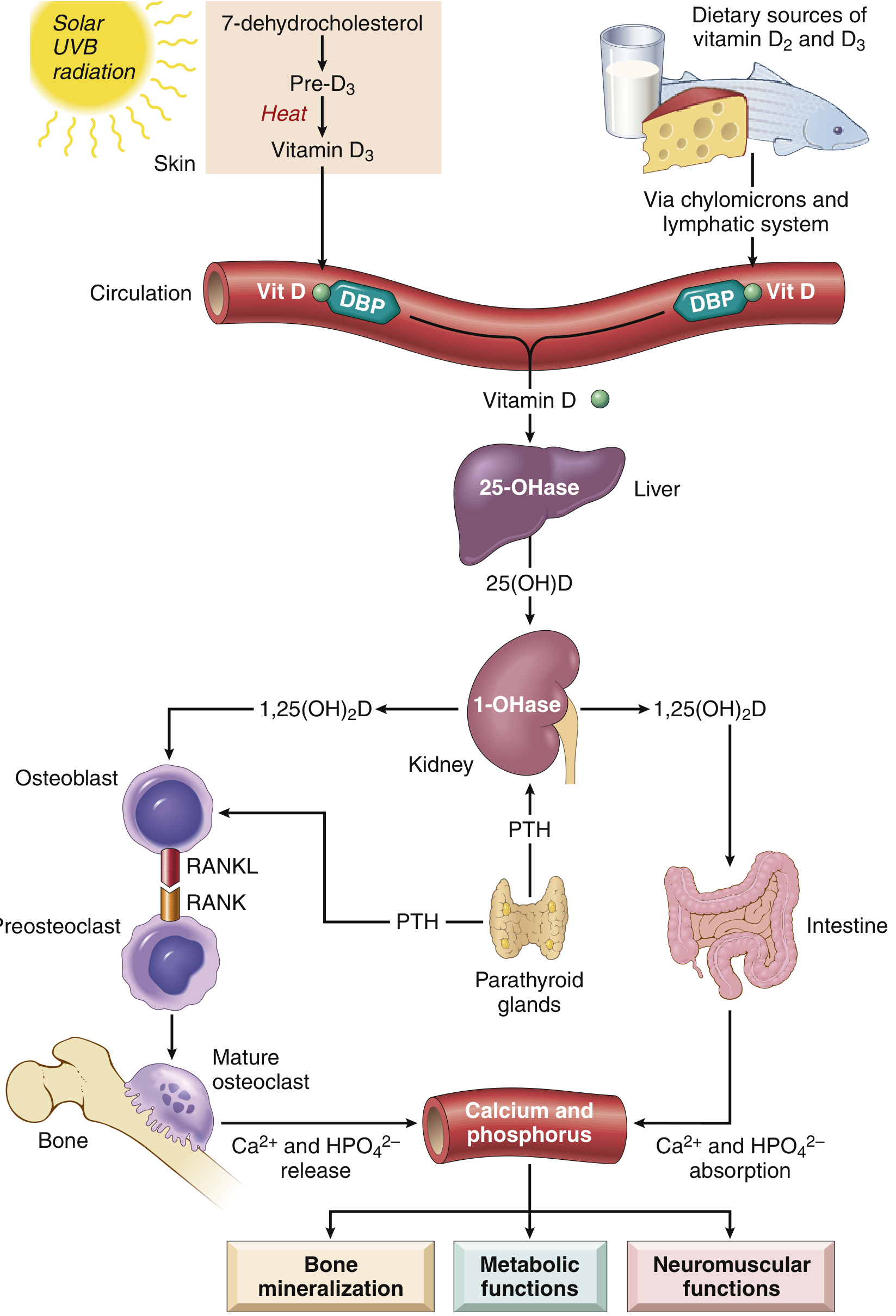
- Endogenous (skin) - ~90% of total: UV light (solar UVB) acts on 7-dehydrocholesterol (an intermediate in cholesterol synthesis that accumulates in skin) → previtamin D (non-enzymatic) → cholecalciferol (D₃) via thermal isomerization
- Dietary:
- Fatty fish (salmon, tuna, mackerel), fish liver oils
- Liver, egg yolk
- Fortified milk (naturally a poor source)
- Plants provide ergosterol/D₂
Key point: In temperate climates, plasma vitamin D is highest at end of summer, lowest at end of winter. Beyond ~40° north or south latitude, there is very little adequate-wavelength UV radiation in winter. Individuals with dark skin produce less vitamin D because melanin absorbs UV light.
4. Metabolism - Two Sequential Hydroxylations
This is the most exam-important pathway:
Step 1 - In the LIVER:
- Cholecalciferol → 25-Hydroxycholecalciferol (Calcidiol / 25-OH-D₃)
- Enzyme: 25-hydroxylase (a cytochrome P450 enzyme)
- Calcidiol is the main circulating/storage form of vitamin D
- Transported in blood bound to vitamin D-binding protein (α₁-globulin / DBP)
Step 2 - In the KIDNEY:
- 25-OH-D₃ → 1,25-Dihydroxycholecalciferol (Calcitriol / 1,25-(OH)₂-D₃)
- Enzyme: 25-hydroxycholecalciferol 1α-hydroxylase (also a cytochrome P450)
- Calcitriol is the biologically active form (most potent metabolite)
- Alternatively: 25-OH-D₃ → 24,25-dihydroxyvitamin D via 24-hydroxylase → this is the inactive/inactivation pathway
Vitamin D Metabolism - Full Diagram (Robbins)
Vitamin D Metabolism + Actions - Lippincott Diagram
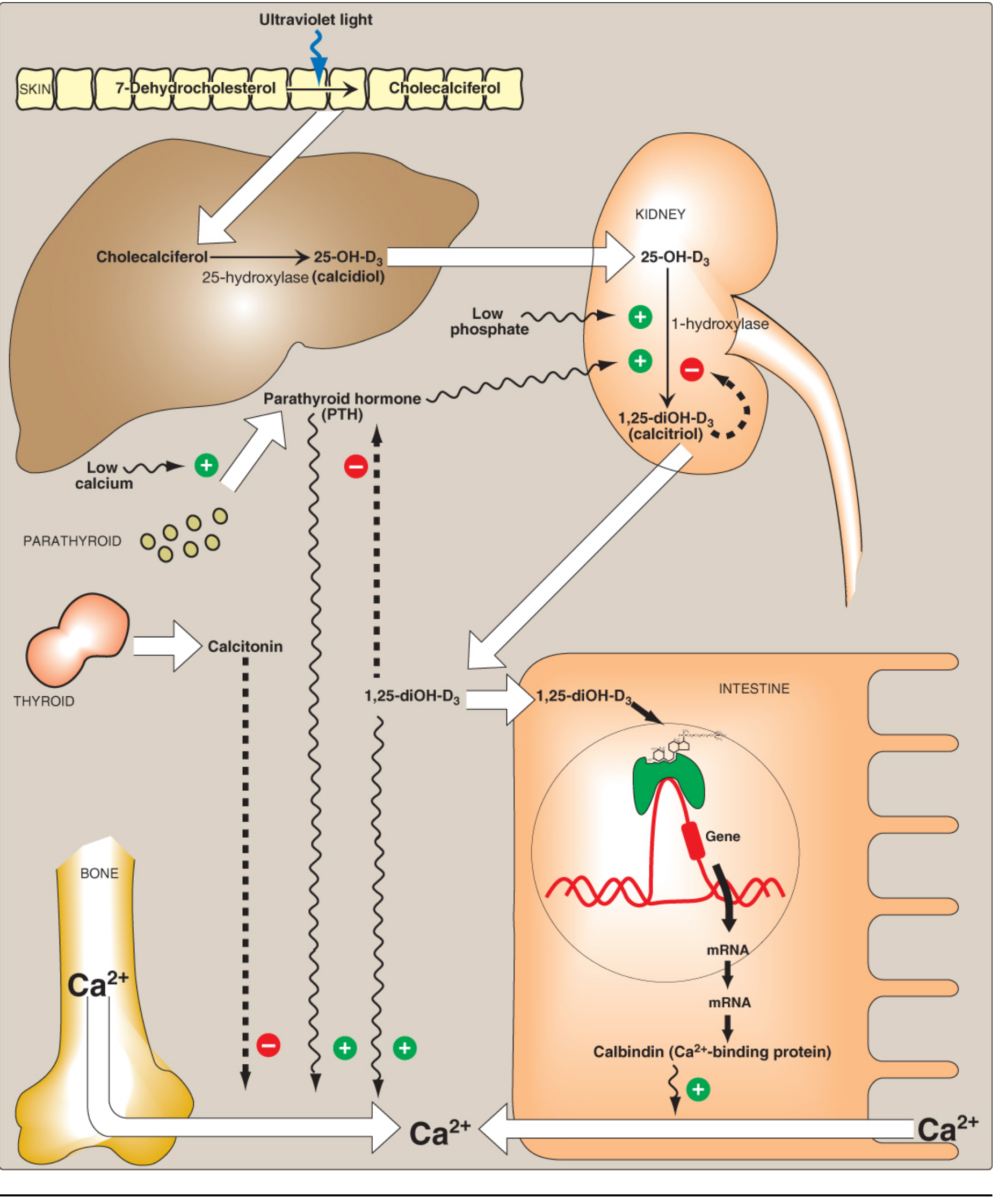
5. Regulation of Calcitriol Synthesis
The renal 1α-hydroxylase is the key regulated enzyme:
| Stimulus | Effect on 1α-hydroxylase | Result |
|---|---|---|
| ↓ Serum Ca²⁺ | ↑ (via PTH) | ↑ Calcitriol |
| ↓ Serum PO₄³⁻ (hypophosphatemia) | ↑ (directly) | ↑ Calcitriol |
| ↑ PTH | ↑ | ↑ Calcitriol |
| ↑ 1,25-(OH)₂-D₃ (calcitriol itself) | ↓ (negative feedback) | ↓ Calcitriol; also induces 24-hydroxylase |
| ↑ Serum Ca²⁺ | ↓ PTH → ↓ 1α-hydroxylase | ↓ Calcitriol |
Note: Calcitriol also inhibits transcription of the PTH gene - completing a negative feedback loop.
6. Mechanism of Action
- Calcitriol (1,25-(OH)₂-D) is a steroid hormone analog
- It binds to the intracellular Vitamin D Receptor (VDR), a nuclear receptor
- The calcitriol-VDR complex heterodimerizes with RXR (Retinoid X Receptor)
- This complex binds to Vitamin D Response Elements (VDREs) on DNA
- Selectively stimulates or represses gene transcription
- VDRs are present in most nucleated cells of the body - explaining vitamin D's wide-ranging effects beyond bone
7. Functions of Vitamin D (Calcitriol)
The overall function is to maintain adequate serum levels of calcium and phosphorus.
A. Intestine (Primary action)
- Calcitriol enters intestinal epithelial cells → binds VDR → activates genes encoding calbindin (calcium-binding protein), calcium channels, and transport proteins
- Results in increased absorption of dietary Ca²⁺ and PO₄³⁻
B. Kidney
- Stimulates calcium reabsorption in the distal renal tubules (upregulates membrane Ca pump, epithelial calcium channels, calbindin)
- PTH and calcitriol work together to prevent renal Ca²⁺ loss
- PTH (but not calcitriol) increases phosphate excretion
C. Bone
Two distinct effects depending on serum calcium status:
- Hypocalcemic states: Together with PTH, stimulates bone resorption (demineralization) to release Ca²⁺ and PO₄³⁻ into blood
- Normocalcemic states: Required for mineralization of osteoid matrix and epiphyseal cartilage during bone formation
- RANK/RANKL pathway: Calcitriol upregulates expression of RANK ligand (RANKL) on osteoblasts → activates RANK receptors on osteoclast precursors → increases osteoclast differentiation and bone resorption
D. Parathyroid
- Increased 1,25-(OH)₂-D decreases transcription of the PTH gene (negative feedback)
E. Other Non-Classical Functions
- Regulates cell proliferation and differentiation in many tissues
- May reduce risk of insulin resistance, obesity, and metabolic syndrome
- Evidence suggests a role in cancer prevention
- Immune system modulation
8. Dietary Requirement and RDA
| Group | RDA |
|---|---|
| Ages 1-70 years | 15 μg/day (600 IU/day) |
| >70 years | 20 μg/day (800 IU/day) |
| Tolerable Upper Limit (≥9 yrs) | 100 μg/day (4,000 IU/day) |
- Conversion: 1 μg vitamin D = 40 IU
- Breast milk is a poor source of vitamin D → supplementation recommended for breastfed infants
- Preformed vitamin D is a dietary requirement only in those with limited sunlight
9. Deficiency States
Causes
- Insufficient sun exposure (northern latitudes, skin covered by clothing, dark skin tone)
- Dietary deficiency of calcium and/or vitamin D
- Fat malabsorption (steatorrhea): celiac disease, Crohn's, biliary obstruction
- Chronic kidney disease - impaired 1α-hydroxylase → decreased calcitriol
- Liver disease - impaired 25-hydroxylation
- Loss-of-function mutations in VDR → hereditary vitamin D-deficient rickets
Pathophysiology of Deficiency
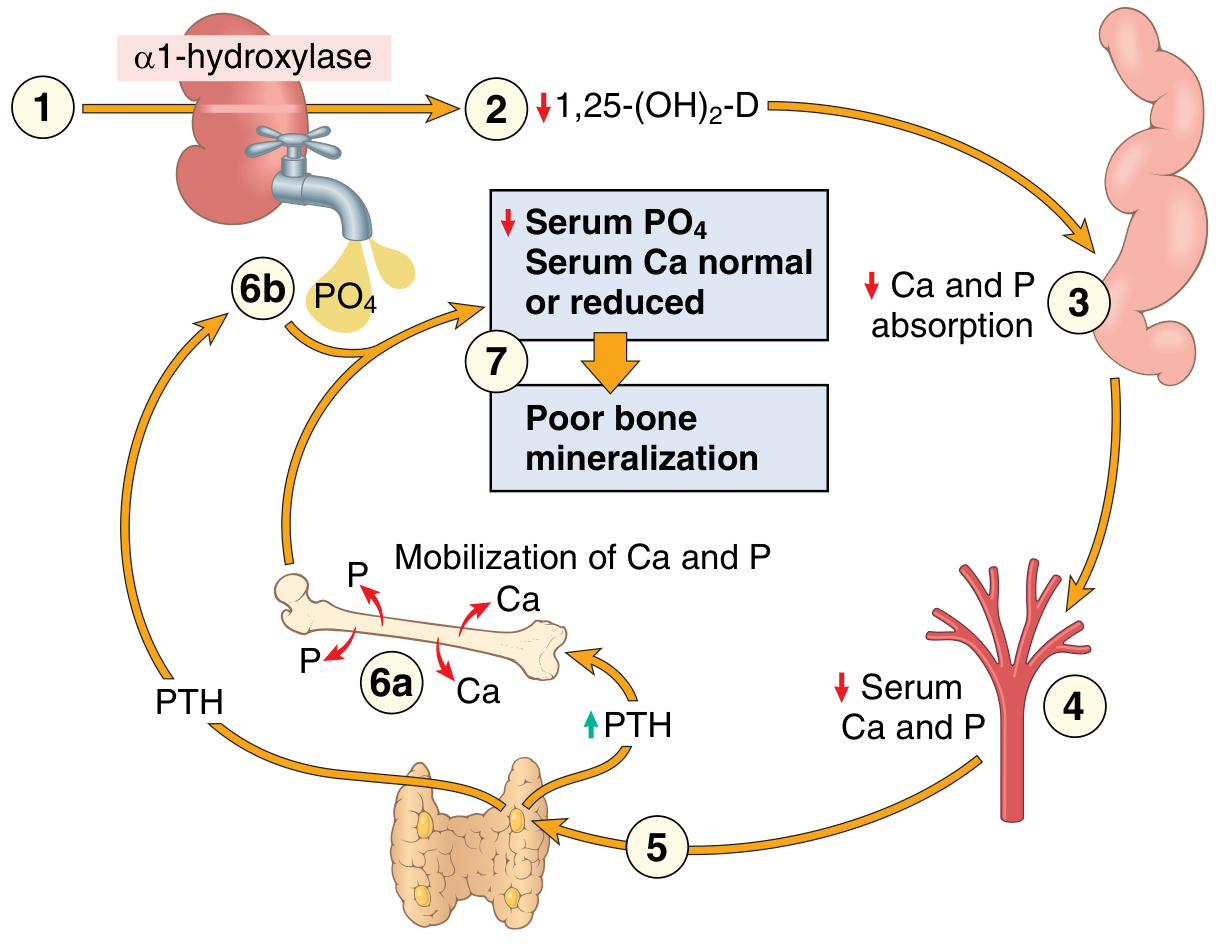
A. Rickets (Children - epiphyses not yet closed)
The basic derangement is excess unmineralized bone matrix (osteoid).
Pathological sequence:
- Hypocalcemia → inadequate provisional calcification of epiphyseal cartilage
- Cartilage cells fail to mature and disintegrate → overgrowth of epiphyseal cartilage
- Persistence of distorted, irregular cartilage masses projecting into marrow cavity
- Osteoid deposited on inadequately mineralized cartilaginous remnants
- Enlargement and lateral expansion of the osteochondral junction
Clinical features of Rickets:
| Feature | Description |
|---|---|
| Craniotabes | Softening of skull bones |
| Frontal bossing | Prominent frontal bones |
| Rachitic rosary | Beading at costochondral junctions (enlarged, irregular) |
| Harrison's sulcus | Groove along diaphragm insertion on ribs |
| Pigeon chest / Pectus carinatum | Protrusion of sternum |
| Bow legs (genu varum) / Knock knees (genu valgum) | Weight-bearing deformity of long bones |
| Epiphyseal enlargement | Especially at wrists and ankles |
| Delayed dentition | |
| Hypocalcemic tetany | Muscle spasms (if Ca²⁺ very low) |
| Pot-belly | Hypotonic abdominal muscles |
B. Osteomalacia (Adults)
- Demineralization of pre-existing bone (epiphyses already closed)
- Bone matrix (osteoid) is laid down but remains unmineralized
- Results in: bone pain, tenderness, muscle weakness
- Pseudofractures (Looser zones): Ribbon-like zones of decalcification perpendicular to bone surface - pathognomonic
- Increased susceptibility to fractures
- Milder forms are common in elderly and lead to hip fractures
C. Hypocalcemic Tetany
- Drop in ionized Ca²⁺ → continuous excitation of muscle
- Rare (PTH usually compensates by mobilizing bone Ca²⁺)
D. Secondary Hyperparathyroidism
- Vitamin D deficiency → hypocalcemia → sustained PTH elevation
- PTH mobilizes Ca²⁺ from bone (bone resorption) → serum Ca²⁺ near-normalized
- But hypophosphatemia persists (PTH promotes phosphaturia)
- Result: impaired mineralization or high bone turnover
10. Toxicity - Hypervitaminosis D
- Only from supplements (excess skin synthesis is converted to inactive forms)
- High doses (100,000 IU for weeks/months) cause:
- Loss of appetite, nausea, vomiting, thirst, weakness
- Hypercalcemia (from increased intestinal absorption + bone resorption)
- Metastatic calcification - deposition of calcium salts in soft tissues (kidneys, blood vessels, heart, lungs)
- Polyuria, polydipsia (nephrocalcinosis)
Key contrast with Vitamin A: Vitamin D toxicity is NOT teratogenic. Also, β-carotene excess doesn't cause Vitamin A toxicity, and excess skin-synthesized vitamin D is safely inactivated.
11. Clinical/Therapeutic Uses
| Condition | Treatment |
|---|---|
| Nutritional rickets/osteomalacia | Vitamin D₂ or D₃ supplementation + calcium |
| Renal osteodystrophy | Active vitamin D (calcitriol) + phosphate-lowering therapy |
| Hypoparathyroidism | Vitamin D + calcium supplementation |
| Osteoporosis | Vitamin D + calcium (adjunctive) |
| Hereditary rickets type I (1α-hydroxylase defect) | Calcitriol (active vitamin D) |
| Hereditary rickets type II (VDR defect) | High-dose calcitriol + calcium |
| Psoriasis | Vitamin D analogs (e.g., calcipotriol) - topical |
12. Summary Table
| Feature | Detail |
|---|---|
| Type | Fat-soluble; steroid hormone |
| Forms | D₂ (ergocalciferol - plants), D₃ (cholecalciferol - animals/skin) |
| Precursor in skin | 7-Dehydrocholesterol |
| Reaction in skin | UV light → previtamin D → cholecalciferol (non-enzymatic) |
| First hydroxylation | Liver: 25-hydroxylase → calcidiol (25-OH-D₃) - main serum/storage form |
| Second hydroxylation | Kidney: 1α-hydroxylase → calcitriol (1,25-(OH)₂-D₃) - active form |
| Inactivation | Kidney: 24-hydroxylase → 24,25-(OH)₂-D (inactive) |
| Transport protein | Vitamin D-binding protein (α₁-globulin / DBP) |
| Mechanism | Nuclear VDR → heterodimerizes with RXR → VDRE → gene transcription |
| Main function | ↑ intestinal Ca²⁺/PO₄ absorption; ↑ renal Ca²⁺ reabsorption; bone mineralization |
| Deficiency - children | Rickets (rachitic rosary, bow legs, craniotabes) |
| Deficiency - adults | Osteomalacia (bone pain, pseudofractures/Looser zones) |
| Toxicity | Hypercalcemia, metastatic calcification |
| RDA (1-70 yrs) | 15 μg/day (600 IU); >70 yrs: 20 μg/day (800 IU) |
| 1 μg = | 40 IU |
Sources: Lippincott Illustrated Reviews: Biochemistry 8th ed, pp. 1085-1093 | Harper's Illustrated Biochemistry 32nd ed, Ch. 44 | Robbins & Kumar Basic Pathology, pp. 294-298
Vitamin C
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
All content and images are ready. Here is the complete Vitamin C notes:
Vitamin C (Ascorbic Acid)
Drawn from Lippincott Illustrated Reviews: Biochemistry (8th ed), Harper's Illustrated Biochemistry (32nd ed), Robbins & Kumar Basic Pathology, and Robbins, Cotran & Kumar Pathologic Basis of Disease - covering the same syllabus as Satynarayan's Biochemistry.
1. Nature and Key Facts
- Vitamin C is a water-soluble vitamin - the only water-soluble vitamin with antioxidant properties
- Chemical name: L-Ascorbic acid (reduced/active form) and Dehydroascorbic acid (oxidized form); both have vitamin activity
- It is a 6-carbon compound, structurally related to glucose (derived from the uronic acid pathway of glucose metabolism in animals that can synthesize it)
- Humans CANNOT synthesize vitamin C - the enzyme gulonolactone oxidase (required for the final step of ascorbate synthesis from glucose) is absent in humans, other primates, and guinea pigs
- Therefore, humans are entirely dependent on dietary intake
- Identified and synthesized in 1932
Structure of Ascorbic Acid
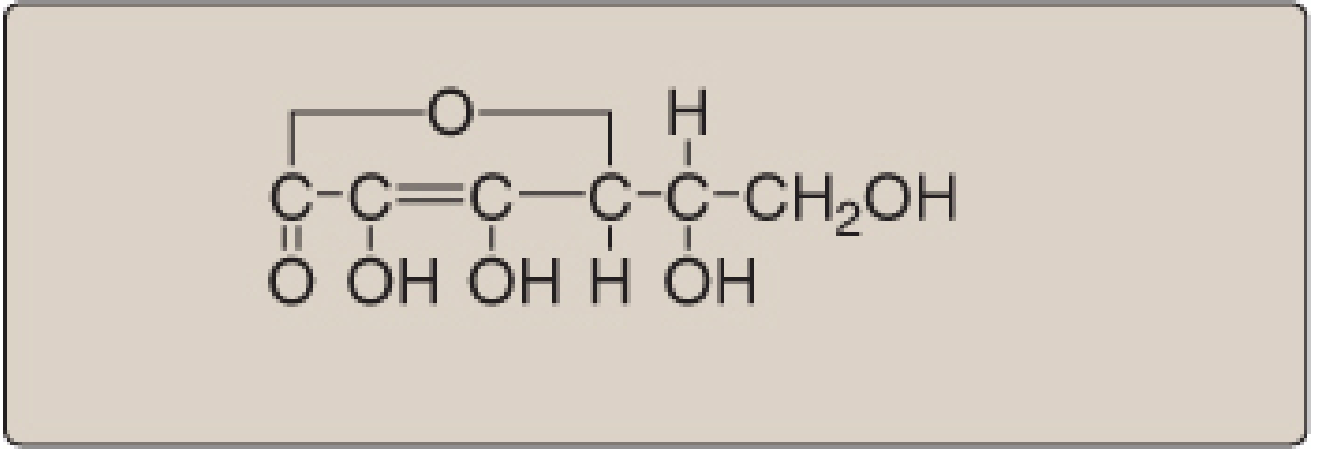
Redox Chemistry: Ascorbate ↔ Dehydroascorbate
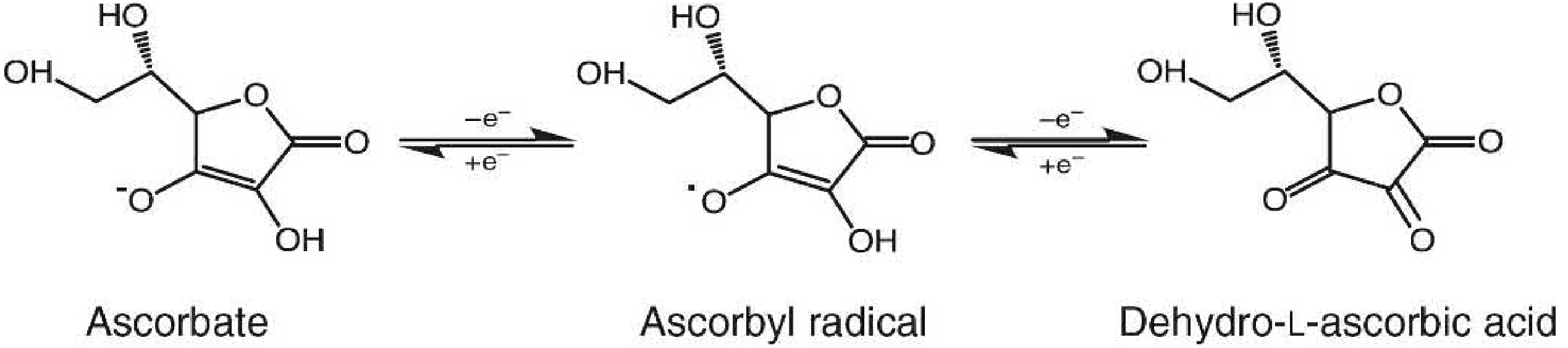
Ascorbic acid donates single electrons in two steps:
Ascorbate → Ascorbyl radical → Dehydroascorbic acid
This reversible redox behavior underlies all its biochemical roles.
2. Dietary Sources
Rich sources (fruits and vegetables):
- Citrus fruits (lemon, lime, orange, grapefruit)
- Guava, amla (Indian gooseberry - richest source)
- Kiwi, strawberries, papaya
- Bell peppers (capsicum), tomatoes
- Broccoli, cabbage, spinach, green leafy vegetables
Animal sources:
- Liver, fish (modest amounts)
- Milk (small amounts)
Historical note: British Royal Navy sailors were called "limeys" because from the late 18th century, the Navy provided lime and lemon juice to sailors to prevent scurvy during long sea voyages.
Important notes on stability:
- Vitamin C is the most labile (easily destroyed) of all vitamins
- Destroyed by heat, oxidation, alkali, and prolonged storage
- Cooking in an open vessel destroys vitamin C (use of baking soda / alkali is particularly destructive)
3. RDA
| Group | RDA |
|---|---|
| Adult males | 90 mg/day |
| Adult females | 75 mg/day |
| Smokers | +35 mg/day extra (increased oxidative stress) |
| Tolerable Upper Limit | 2,000 mg/day |
- At intakes above ~100 mg/day, the body's capacity to metabolize vitamin C is saturated and any excess is excreted in urine
4. Biochemical Functions
Vitamin C is a reducing agent (antioxidant) and acts as a coenzyme in hydroxylation reactions by keeping metal cofactors in their reduced state.
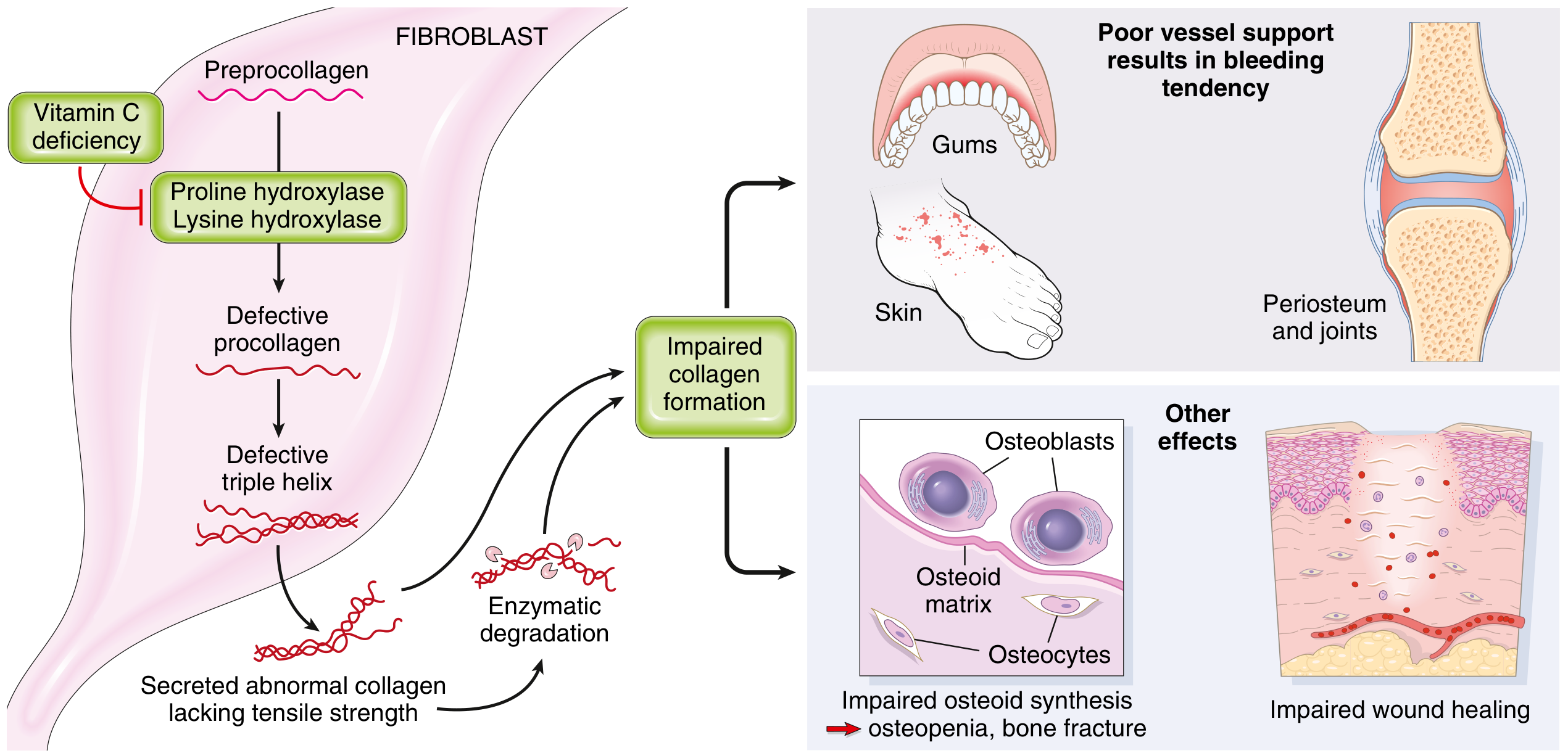
A. Collagen Synthesis (Most Important Function)
Vitamin C activates prolyl hydroxylase and lysyl hydroxylase - enzymes that catalyze the post-translational hydroxylation of proline and lysine residues in procollagen:
- Prolyl hydroxylase: hydroxylates proline → hydroxyproline (required for hydrogen bonding and stabilization of the triple helix)
- Lysyl hydroxylase: hydroxylates lysine → hydroxylysine (required for cross-linking of collagen fibrils)
Mechanism: These enzymes contain Fe²⁺ (ferrous iron) in their active site. During each hydroxylation reaction, Fe²⁺ is oxidized to Fe³⁺ (ferric). Vitamin C reduces Fe³⁺ back to Fe²⁺, keeping the enzyme active. Without vitamin C, the enzymes become inactive.
Consequence of deficiency:
- Inadequately hydroxylated procollagen cannot acquire a stable triple helical configuration
- Defective procollagen is poorly secreted from fibroblasts
- Secreted molecules lack tensile strength, are more soluble, and are degraded enzymatically
- Collagen (which has the highest hydroxyproline content of any protein) is most affected - especially in blood vessels → hemorrhagic tendency
- Vitamin C also directly stimulates collagen polypeptide synthesis, independent of hydroxylation
B. Catecholamine Synthesis
- Dopamine β-hydroxylase (copper-containing enzyme) converts dopamine → norepinephrine in the adrenal medulla and CNS
- During this reaction, Cu⁺ is oxidized to Cu²⁺
- Vitamin C reduces Cu²⁺ back to Cu⁺, reactivating the enzyme
- Consequence of deficiency: impaired catecholamine synthesis → psychological changes (fatigue, depression) seen in scurvy
C. Peptide Hormone Amidation
- Peptidylglycine hydroxylase (copper enzyme) creates carboxy-terminal amides on peptide hormones (e.g., oxytocin, ADH, gastrin, CRH)
- Vitamin C keeps this enzyme's copper in the reduced Cu⁺ state
- Required for full biological activity of several hormones
D. Carnitine Synthesis
- Two hydroxylation enzymes in carnitine synthesis require vitamin C:
- Trimethyllysine hydroxylase
- γ-Butyrobetaine hydroxylase
- Carnitine is needed for transport of long-chain fatty acids into mitochondria for β-oxidation
- Deficiency → fatigue and muscle weakness (partly explained by impaired fatty acid oxidation)
E. Iron Absorption (Non-Enzymatic)
- Dietary non-heme iron is in the ferric (Fe³⁺) form, which is poorly absorbed
- Vitamin C in the intestinal lumen reduces Fe³⁺ → Fe²⁺ (ferrous), which is readily absorbed by intestinal transporters
- Vitamin C should therefore be taken with iron supplements to maximize iron absorption
- This is clinically used in iron deficiency anemia treatment
F. Antioxidant Functions
- Vitamin C is a powerful water-soluble antioxidant - it scavenges free radicals (superoxide, hydroxyl radical, peroxyl radical, hypochlorite, NO₂) directly
- Regenerates vitamin E: Vitamin E (fat-soluble, in membranes) is oxidized to a tocopheryl radical after neutralizing a free radical. Water-soluble vitamin C in extracellular fluid donates electrons to regenerate the functional reduced form of vitamin E. This vitamin C-vitamin E recycling is a key antioxidant mechanism.
- Also reacts with singlet oxygen and hydrogen peroxide
F. Collagen-Related Functions Summary
Vitamin C is required for:
- Synthesis of collagen (type I, II, III, IV)
- Synthesis of osteocalcin (via proline hydroxylase)
- Synthesis of C1q complement component (proline hydroxylase)
- Synthesis of protein C (coagulation - aspartate β-hydroxylase)
5. Deficiency - SCURVY
Scurvy is the disease of vitamin C deficiency. It develops after 1-3 months of severely deficient diet.
Pathophysiology
The central defect is failure to hydroxylate procollagen → defective collagen → poor support for connective tissue, blood vessels, bone, and wound healing.
At-Risk Groups
- Infants maintained on evaporated milk formulas without supplementation
- Elderly persons living alone with poor diets
- Alcoholics (erratic, inadequate eating patterns)
- Patients on peritoneal or hemodialysis
- Food faddists and those on severely restricted diets
Clinical Features of Scurvy
Gums and teeth (most characteristic):
- Swollen, spongy, bleeding gums (gingivitis)
- Gums become red, hemorrhagic, and infected
- Loose teeth (loss of periodontal ligament collagen support)

Skin and soft tissue:
- Perifollicular hemorrhages - petechial hemorrhages around hair follicles (earliest skin sign)
- Corkscrew hairs - coiled, fragmented hair shafts
- Ecchymoses (bruising) from fragile capillaries
- Poor wound healing
Bones and joints:
- Subperiosteal hemorrhages - extremely painful; limbs held in "frog-leg" position (pseudoparalysis in infants)
- Scorbutic rosary - widening and cupping at costochondral junctions (periosteal hemorrhage; different from rachitic rosary which is due to cartilage overgrowth)
- Osteopenia - impaired osteoid synthesis by osteoblasts
- Bone fractures
- Hemarthroses (bleeding into joints)
Systemic:
- Fatigue and weakness (earliest symptom; from impaired carnitine synthesis and catecholamine production)
- Microcytic anemia - from decreased iron absorption + bleeding
- Psychological changes - depression, irritability (impaired catecholamine synthesis)
- Impaired wound healing
Key Distinguishing Points: Scurvy vs Rickets
| Feature | Scurvy (Vitamin C) | Rickets (Vitamin D) |
|---|---|---|
| Rosary type | Scorbutic rosary (subperiosteal hemorrhage) | Rachitic rosary (cartilage overgrowth) |
| Bone lesion | Subperiosteal hemorrhage, impaired osteoid | Excess unmineralized osteoid |
| Gums | Bleeding, spongy | Normal |
| Serum Ca/P | Normal | Abnormal |
| Tenderness | Extreme (hemorrhage) | Less severe |
6. Toxicity - Hypervitaminosis C
Unlike fat-soluble vitamins, vitamin C toxicity is uncommon due to:
- Limited intestinal absorption at high doses
- Rapid urinary excretion of excess
Adverse effects of megadoses:
- Oxalate kidney stones - ascorbic acid is catabolized to oxalate; excess oxalate → calcium oxalate stones
- Iron overload - excessive iron absorption in susceptible individuals
- Hemolytic anemia - in individuals with G6PD deficiency (important exam point)
- Uricosuria - may precipitate gout in susceptible individuals
- Rebound scurvy - if high-dose supplementation is abruptly stopped (body adapts to rapid catabolism)
- "Pro-oxidant" effect at very high doses in the presence of free metal ions
Vitamin C and the common cold: Despite popular belief, controlled clinical trials have not shown that megadoses of vitamin C prevent the common cold. High intake may slightly reduce duration/severity, possibly due to a mild antihistamine action. Similarly, trials have not shown protection against cancer, cardiovascular disease, cataracts, or macular degeneration.
7. Summary of All Enzymatic Roles
| Enzyme | Metal | Reaction | Deficiency Effect |
|---|---|---|---|
| Prolyl hydroxylase | Fe | Proline → Hydroxyproline | Defective collagen |
| Lysyl hydroxylase | Fe | Lysine → Hydroxylysine | Poor collagen cross-linking |
| Dopamine β-hydroxylase | Cu | Dopamine → Norepinephrine | Fatigue, depression |
| Peptidylglycine hydroxylase | Cu | Peptide amidation | Inactive peptide hormones |
| Trimethyllysine hydroxylase | Fe | Carnitine synthesis | Muscle weakness |
| γ-Butyrobetaine hydroxylase | Fe | Carnitine synthesis | Muscle weakness |
| Aspartate β-hydroxylase | Fe | Protein C maturation | Coagulation defect |
8. Summary Table
| Feature | Detail |
|---|---|
| Type | Water-soluble vitamin |
| Chemical name | L-Ascorbic acid (active/reduced form) |
| Humans can synthesize? | No - lacks gulonolactone oxidase |
| Active forms | Ascorbic acid AND dehydroascorbic acid (both active) |
| Mechanism | Keeps Fe²⁺ and Cu⁺ in reduced state in hydroxylases; direct antioxidant |
| Key function | Collagen synthesis (hydroxylation of Pro and Lys) |
| Other functions | Catecholamine synthesis, carnitine synthesis, iron absorption, antioxidant (regenerates Vit E) |
| Deficiency disease | Scurvy |
| Earliest symptom | Fatigue and weakness |
| Gum sign | Bleeding, spongy gums; loose teeth |
| Skin sign | Perifollicular hemorrhages, corkscrew hairs |
| Bone sign | Subperiosteal hemorrhages, scorbutic rosary |
| Anemia type | Microcytic (↓ iron absorption) |
| Toxicity | Oxalate stones, iron overload, hemolysis in G6PD deficiency |
| RDA | 90 mg/day (men), 75 mg/day (women) |
| Richest food source | Amla (Indian gooseberry), guava, citrus fruits |
| Most unstable vitamin | Yes - destroyed by heat, alkali, oxidation |
Sources: Lippincott Illustrated Reviews: Biochemistry 8th ed, p. 1057-1059 | Harper's Illustrated Biochemistry 32nd ed, Ch. 44 | Robbins & Kumar Basic Pathology, pp. 297-298 | Robbins, Cotran & Kumar Pathologic Basis of Disease, pp. 419-421
Vitamin k and vitamin E
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
All content and diagrams collected. Here are the complete notes:
PART 1: Vitamin K
Fat-soluble vitamin. Sources: Lippincott Illustrated Reviews: Biochemistry (8th ed), Harper's Illustrated Biochemistry (32nd ed).
1. Discovery
Vitamin K was discovered while investigating a hemorrhagic (bleeding) disorder in:
- Chickens fed a fat-free diet (missing vitamin K)
- Cattle fed sweet clover feed (contained dicumarol, an antagonist of vitamin K)
The name "K" comes from the German word "Koagulation" (coagulation).
2. Forms of Vitamin K
All forms share a naphthoquinone ring as the basic structure.
Structures of Vitamin K vitamers
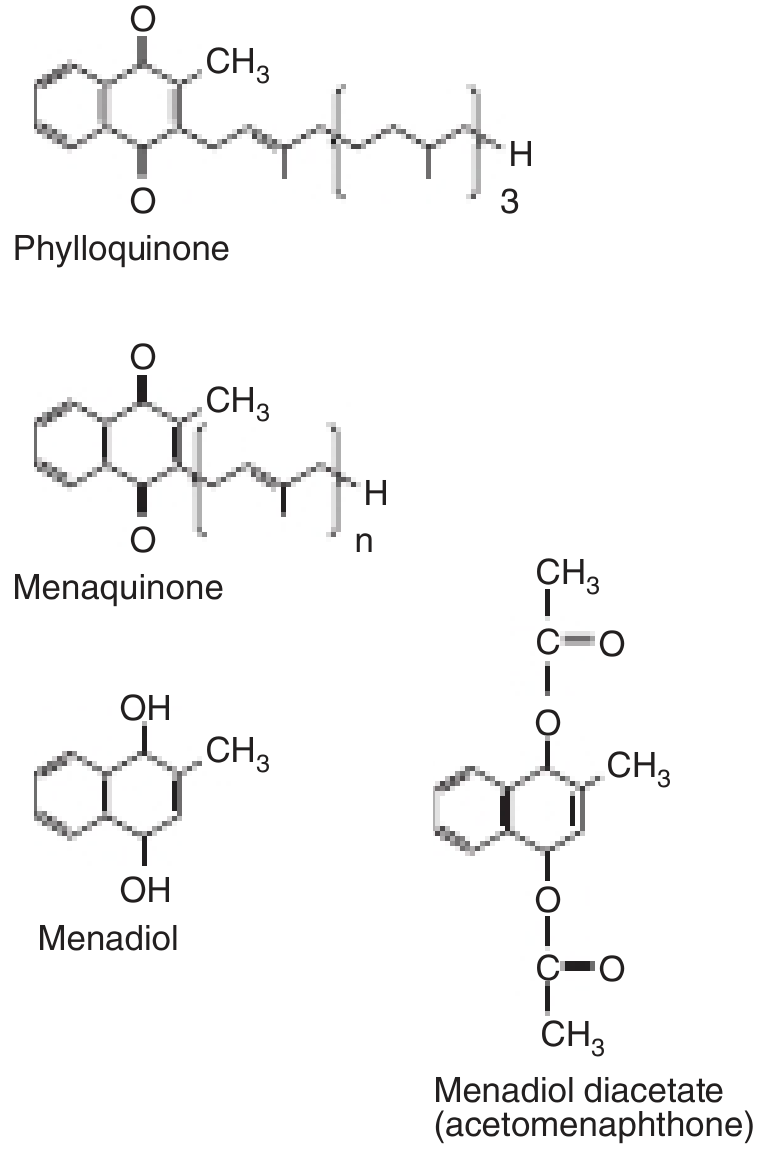
| Form | Name | Source |
|---|---|---|
| Vitamin K₁ | Phylloquinone | Green plants; major dietary source |
| Vitamin K₂ | Menaquinone | Synthesized by intestinal bacteria (gut flora); varying side-chain lengths |
| Vitamin K₃ | Menadione / Menadiol | Synthetic form; converted to K₂ in the liver |
- Dietary vitamin K is packaged into chylomicrons and absorbed with fat
- Requires bile and pancreatic enzymes for absorption (fat-soluble)
3. Dietary Sources and RDA
Sources: Green leafy vegetables (cabbage, kale, spinach), egg yolk, liver, vegetable oils
| Group | Adequate Intake (AI) |
|---|---|
| Adult males | 120 μg/day |
| Adult females | 90 μg/day |
No Tolerable Upper Limit (UL) has been set for natural forms of vitamin K.
4. Biochemical Function - The γ-Carboxyglutamate (Gla) Reaction
The principal role of vitamin K is as a coenzyme for γ-glutamyl carboxylase, the enzyme that catalyzes the post-translational carboxylation of glutamate (Glu) residues → γ-carboxyglutamate (Gla) residues in specific proteins.
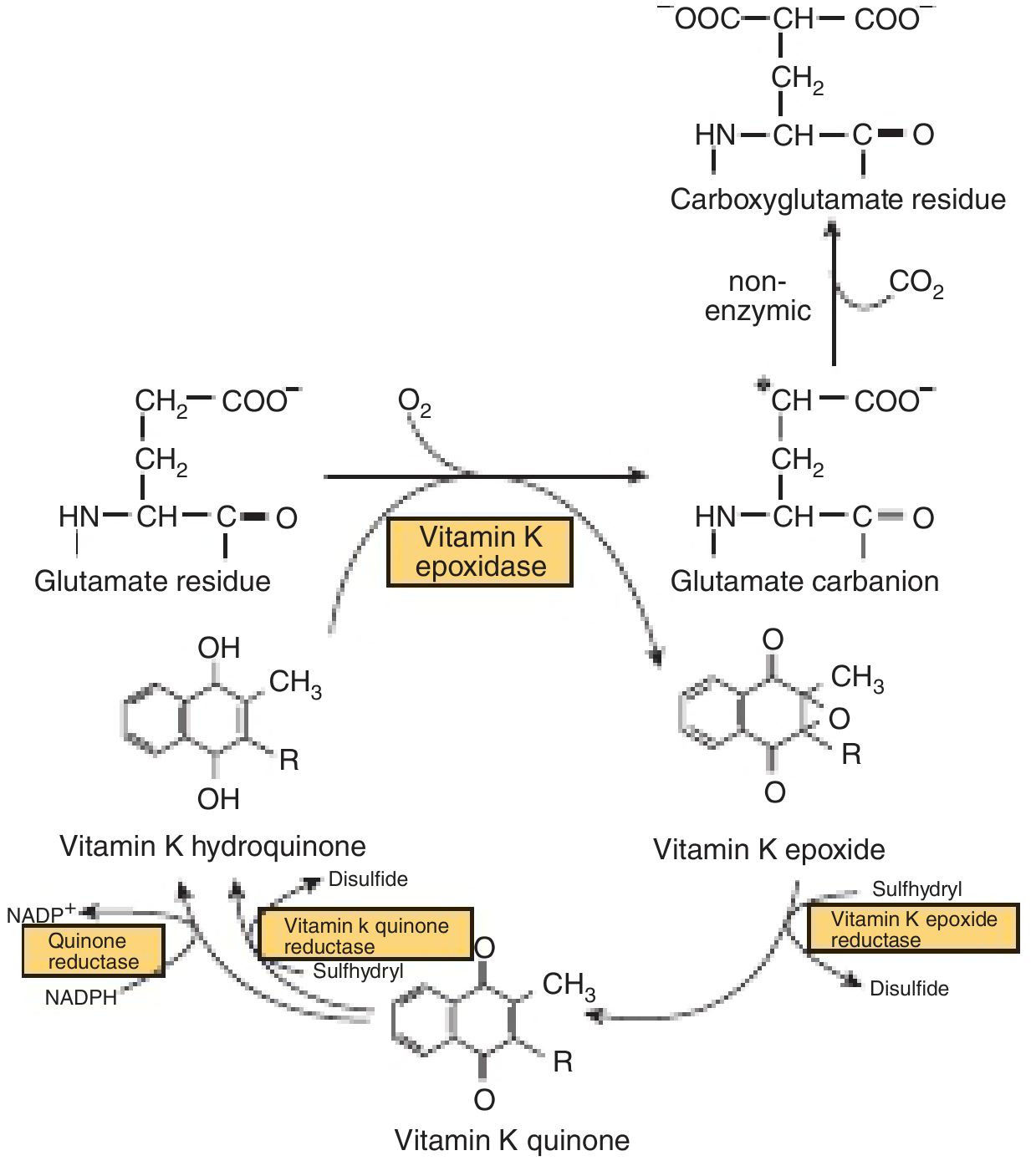
The Vitamin K Cycle and Carboxylation Mechanism
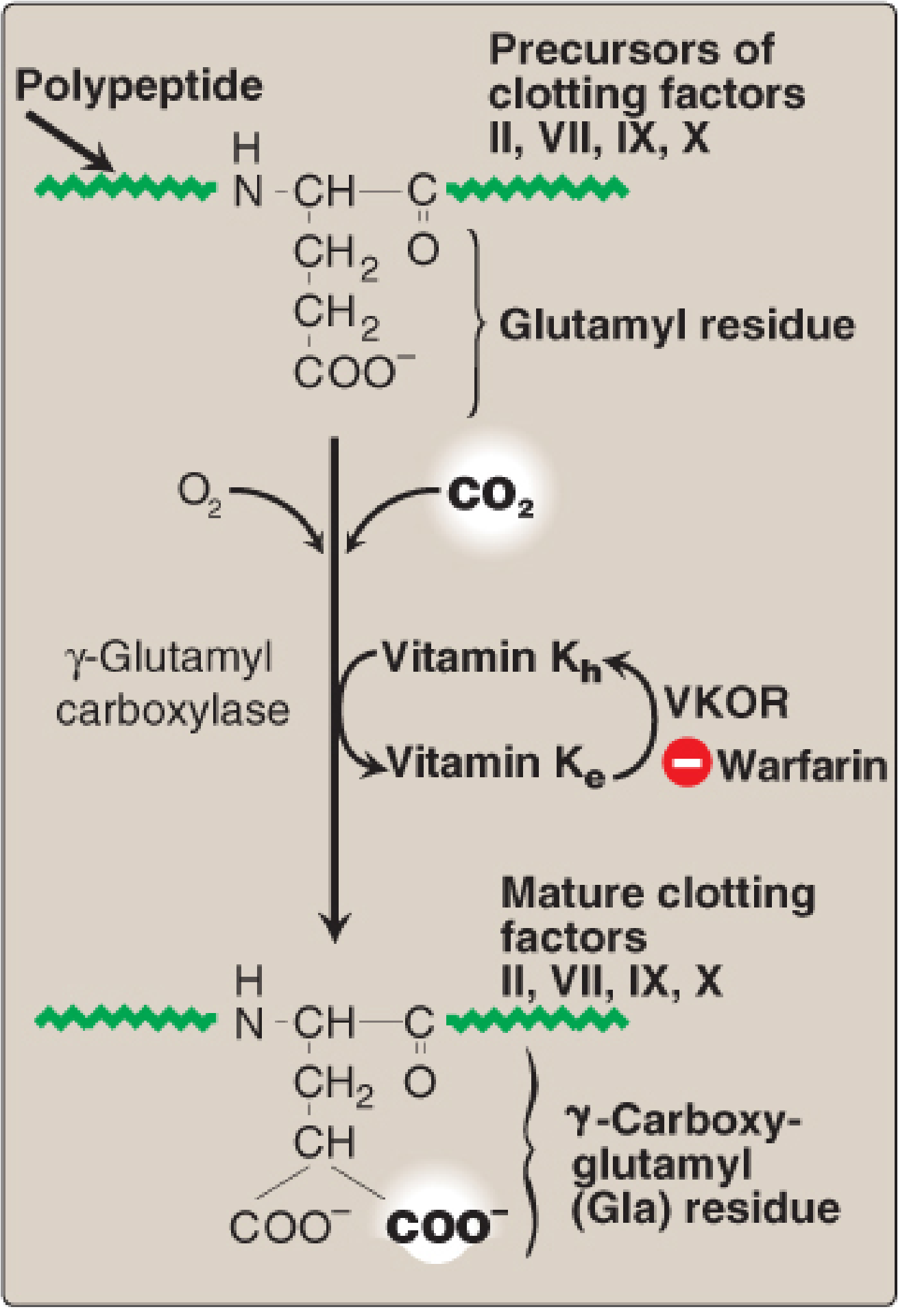
Step-by-step mechanism (Harper's):
- Vitamin K hydroquinone (active form) is oxidized to vitamin K epoxide by vitamin K epoxidase (γ-glutamyl carboxylase)
- This activates a glutamate residue in the protein substrate to a carbanion intermediate
- The carbanion reacts non-enzymically with CO₂ to form γ-carboxyglutamate (Gla)
- Vitamin K epoxide is then reduced back to the quinone form by Vitamin K Epoxide Reductase (VKOR) - this step is warfarin-sensitive
- Quinone is reduced to active hydroquinone by either the same warfarin-sensitive VKOR or a warfarin-insensitive quinone reductase
Requirements: γ-glutamyl carboxylase, O₂, CO₂, vitamin K hydroquinone
5. Why Are Gla Residues Important? - Membrane Binding via Calcium
Diagram - Prothrombin Activation at Membrane
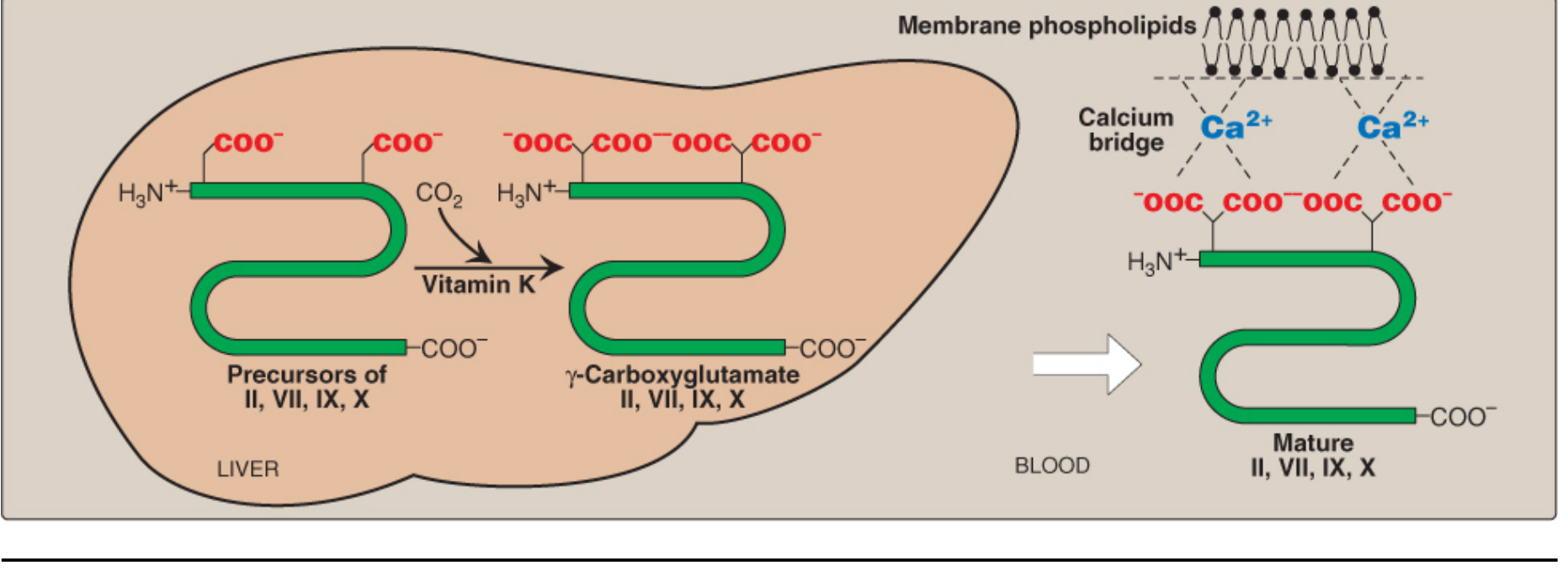
The Gla residues have two adjacent, negatively charged carboxylate groups - excellent chelators of positively charged Ca²⁺ ions. This allows:
- The clotting factor-Ca²⁺ complex to bind to negatively charged phospholipids on the surface of damaged endothelium and activated platelets
- Membrane anchoring greatly accelerates the rate of proteolytic activation of these factors
Vitamin K Epoxide Reductase Cycle (Harper's)
6. Proteins Requiring Vitamin K-Dependent Carboxylation
Pro-Coagulant Factors (in blood clotting cascade)
- Factor II (Prothrombin)
- Factor VII
- Factor IX
- Factor X
Anticoagulant Proteins (limiting clot formation)
- Protein C - vitamin K-dependent protease that cleaves and inactivates activated Factor V and Factor VIII
- Protein S - cofactor for Protein C
Bone and Other Proteins
- Osteocalcin (bone Gla protein) - in bone matrix; binds calcium; its release into blood is an index of vitamin D status
- Matrix Gla Protein (MGP) - in bone and cartilage; inhibits calcification of blood vessels
- Nephrocalcin - in kidney
- Gas6 protein - involved in regulation of differentiation, development in nervous system, and control of apoptosis
7. Warfarin - Mechanism of Action
Warfarin (and other coumarin anticoagulants) are structural analogs of vitamin K:
- They inhibit VKOR (Vitamin K Epoxide Reductase) - the enzyme that regenerates the functional hydroquinone form of vitamin K
- Without VKOR, vitamin K epoxide accumulates and is excreted - vitamin K is not recycled
- Result: inactive precursor forms (non-carboxylated, without Gla residues) of Factors II, VII, IX, X, Protein C, and Protein S accumulate in the blood
- These factors cannot bind Ca²⁺ or anchor to membranes → impaired coagulation
Antidote to warfarin overdose:
- High-dose vitamin K (as the quinone form) - can be reduced to hydroquinone by the warfarin-insensitive quinone reductase, bypassing the blocked VKOR step
- Fresh Frozen Plasma (FFP) provides immediate clotting factors
Certain cephalosporin antibiotics (e.g., cefamandole) cause hypoprothrombinemia by a warfarin-like mechanism inhibiting VKOR.
8. Deficiency
True dietary vitamin K deficiency is unusual in adults because:
- Adequate amounts come from diet (green vegetables)
- Intestinal bacteria (gut microbiota) synthesize vitamin K₂
When Deficiency Occurs:
| Cause | Mechanism |
|---|---|
| Antibiotics (broad spectrum) | Destroy gut bacteria → ↓ vitamin K₂ synthesis |
| Fat malabsorption | Reduced absorption of fat-soluble vitamin K |
| Newborns | Sterile intestines at birth → no bacterial synthesis; breast milk provides only ~1/5 of daily requirement |
| Liver disease | Impaired synthesis of clotting factors and decreased bile production |
| Debilitated/malnourished elderly | Marginal nutrition + reduced bacterial synthesis |
Clinical Features of Deficiency:
- Prolonged PT (Prothrombin Time) and APTT - most sensitive test
- Hemorrhagic tendency - easy bruising, mucosal bleeding, hematuria, melena
- Hypoprothrombinemia (low prothrombin activity)
Hemorrhagic Disease of the Newborn (HDN):
- Newborns have sterile intestines → lack vitamin K₂-synthesizing bacteria
- Breast milk provides only about 1/5 of the daily vitamin K requirement
- Prevention: A single intramuscular dose of vitamin K (phytomenadione) is given to all newborns at birth as prophylaxis
- Without prophylaxis: bleeding can occur from cord, skin, GI tract, or intracranially
9. Toxicity
- Natural forms (K₁, K₂): No UL set; not known to be toxic even at high doses
- Menadione (K₃ - synthetic form): Toxic in infants at high doses
- Causes hemolytic anemia (oxidative damage to RBC membranes)
- Causes neonatal jaundice (hyperbilirubinemia from hemolysis)
- Therefore menadione is no longer used to treat vitamin K deficiency
10. Summary - Vitamin K
| Feature | Detail |
|---|---|
| Type | Fat-soluble |
| Forms | K₁ (phylloquinone - diet), K₂ (menaquinone - gut bacteria), K₃ (menadione - synthetic) |
| Active form | Hydroquinone form |
| Mechanism | γ-glutamyl carboxylase: Glu → Gla (γ-carboxyglutamate) requiring O₂, CO₂ |
| Key function | Post-translational carboxylation of clotting factors (II, VII, IX, X) and proteins C, S |
| Why Gla matters | Chelates Ca²⁺ → membrane binding → clotting factor activation |
| VKOR | Regenerates active vitamin K hydroquinone; inhibited by warfarin |
| Deficiency disease | Bleeding tendency, hypoprothrombinemia, HDN in newborns |
| Key at-risk group | Newborns (sterile gut), patients on antibiotics |
| Warfarin antidote | High-dose vitamin K (quinone form) |
| AI (adults) | 120 μg/day (males), 90 μg/day (females) |
| Toxic form | Menadione (K₃) - hemolysis and jaundice in infants |
PART 2: Vitamin E (Tocopherol)
Fat-soluble vitamin. Sources: Lippincott Illustrated Reviews: Biochemistry (8th ed), Harper's Illustrated Biochemistry (32nd ed).
1. Nature and Forms
Vitamin E is the generic descriptor for two families of compounds:
- Tocopherols - saturated phytyl side chain
- Tocotrienols - unsaturated side chain (3 double bonds)
Structures - Tocopherol vs Tocotrienol
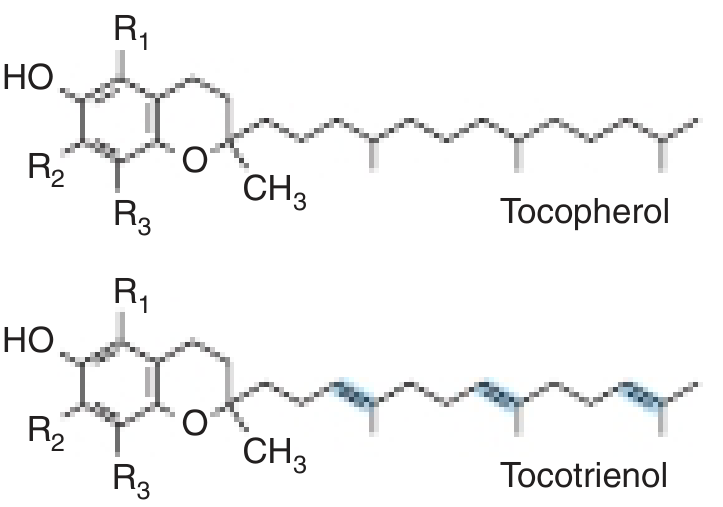
Within each family, there are α, β, γ, δ vitamers depending on the number of methyl (–CH₃) groups:
- α (alpha): R₁, R₂, R₃ all = –CH₃ (three methyls) → most biologically active
- β (beta): R₂ = H
- γ (gamma): R₁ = H
- δ (delta): R₁ and R₂ = H
Structure of α-Tocopherol (Lippincott)
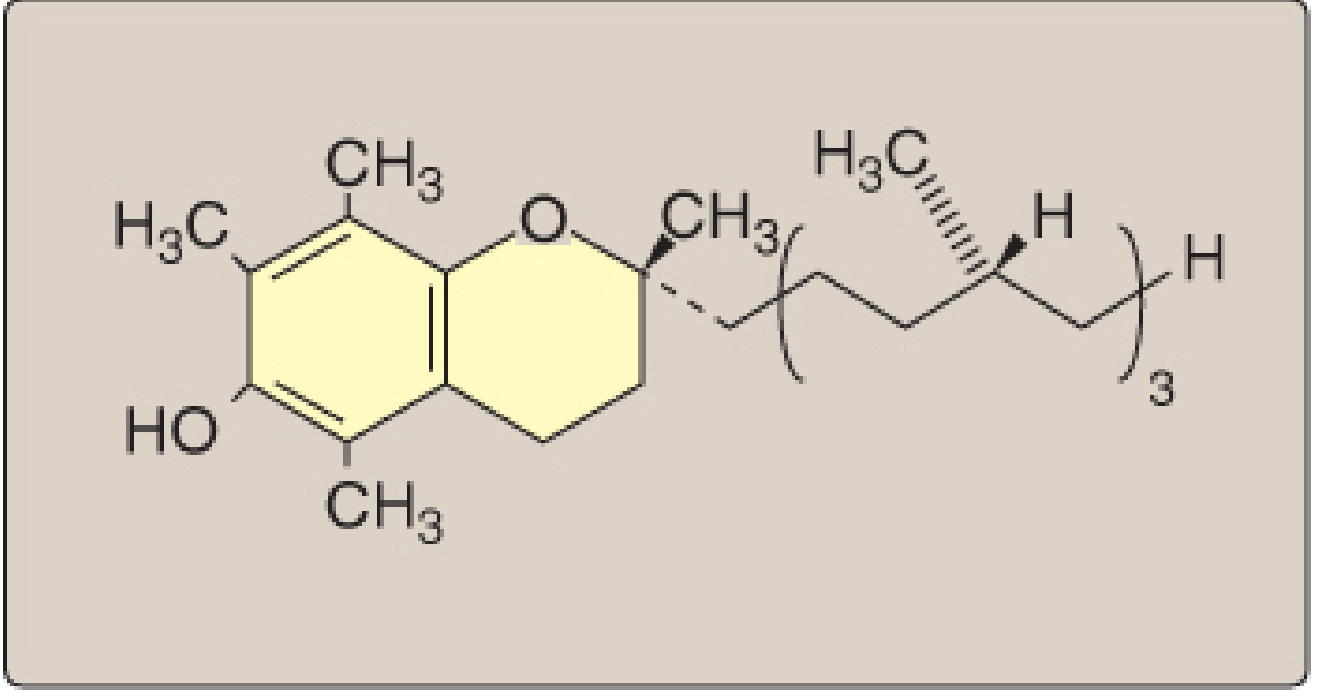
Potency: d-α-tocopherol (naturally occurring) > synthetic DL-α-tocopherol (less biologically potent)
Vitamin E activity is expressed in milligrams of d-α-tocopherol equivalents.
2. Dietary Sources and RDA
Rich sources:
- Vegetable oils (wheat germ oil, sunflower oil, safflower oil, corn oil) - richest sources
- Nuts and seeds (almonds, sunflower seeds)
- Whole grains
- Liver, eggs - moderate amounts
- Green leafy vegetables
| Group | RDA |
|---|---|
| Adults (males and females) | 15 mg/day of α-tocopherol |
| Tolerable Upper Limit | 1,000 mg/day |
The vitamin E requirement increases as the intake of polyunsaturated fatty acids (PUFAs) increases, because more PUFAs means more susceptibility to lipid peroxidation and greater need for antioxidant protection.
3. Biochemical Functions
A. Primary Function: Chain-Breaking Lipid-Soluble Antioxidant
Vitamin E is the major lipid-soluble antioxidant in cell membranes and plasma lipoproteins.
Mechanism:
- PUFAs in membrane phospholipids and LDL are highly susceptible to free radical chain reactions (lipid peroxidation)
- A free radical (R•) abstracts a hydrogen from a PUFA → lipid peroxyl radical (LOO•)
- Vitamin E (as tocopherol, TOH) donates a hydrogen atom to the peroxyl radical → lipid hydroperoxide (LOOH) + tocopheryl radical (TO•)
- The tocopheryl radical is relatively unreactive and does not propagate the chain - this is what makes vitamin E a "chain-breaking" antioxidant
- The tocopheryl radical is then reduced back to active tocopherol by vitamin C (from plasma), completing the cycle
- The resultant stable monodehydroascorbate radical undergoes further reaction to yield ascorbate and dehydroascorbate (neither is a radical)
Summary of the antioxidant interplay:
Free radical → LOO• → [Vit E donates H] → LOOH + TO• (tocopheryl radical)
↓
[Vit C reduces TO• back to TOH]
Ascorbate → Monodehydroascorbate → Dehydroascorbate
B. Specific Targets of Protection
- Membrane PUFAs - prevents lipid peroxidation, maintains membrane fluidity and integrity
- LDL oxidation - prevents oxidation of LDL particles (oxidized LDL is atherogenic)
- RBC membranes - prevents hemolysis
- Photoreceptors in retina - rich in PUFAs, very susceptible to oxidative damage
C. Cell Signaling
- Vitamin E has a relatively poorly defined role in cell signaling (beyond antioxidant function)
- No unique, precisely defined metabolic function beyond antioxidant activity has been established
4. Deficiency
Dietary deficiency of vitamin E in healthy humans is RARE because:
- Widely present in vegetable oils and common foods
- Large body reserves stored in adipose tissue and cell membranes
Who Gets Deficiency?
| Condition | Mechanism |
|---|---|
| Fat malabsorption (celiac, Crohn's, chronic pancreatitis) | Cannot absorb fat-soluble vitamin E |
| Cystic fibrosis | Fat malabsorption due to pancreatic insufficiency |
| Chronic liver disease (cirrhosis, cholestasis) | Cannot absorb or transport vitamin E |
| Abetalipoproteinemia | Defect in chylomicron and VLDL formation → vitamin E cannot be transported from intestine → classic genetic cause of vitamin E deficiency |
| Premature infants (VLBW) | Born with inadequate vitamin E reserves |
Clinical Features of Deficiency
| Feature | Explanation |
|---|---|
| Hemolytic anemia | Erythrocyte membranes are abnormally fragile due to lipid peroxidation of PUFA in RBC membranes → hemolysis |
| Spinocerebellar ataxia | Demyelination of posterior columns and spinocerebellar tracts |
| Peripheral neuropathy | Axonal degeneration due to membrane oxidative damage |
| Ophthalmoplegia | Extraocular muscle weakness |
| Retinopathy (in premature infants) | Peroxidative damage to retinal photoreceptors |
| Reproductive failure (animal studies) | Resorption of fetuses; testicular atrophy in experimental animals |
| Muscle weakness, myopathy | Oxidative damage to muscle membranes |
In experimental animals vitamin E deficiency causes resorption of fetuses and testicular atrophy - hence its original name "tocopherol" from Greek: tokos = childbirth + pherein = to bear (fertility vitamin).
Premature Infants:
- Given vitamin E supplements to prevent:
- Hemolytic anemia
- Retinopathy of prematurity
5. Vitamin E and Chronic Disease - Disappointing Clinical Results
Despite strong biological rationale as an antioxidant, clinical trials have been uniformly disappointing:
- Cardiovascular disease prevention: No benefit; in the Alpha-Tocopherol, Beta-Carotene (ATBC) Cancer Prevention Study, high-dose vitamin E showed no cardiovascular benefit and actually increased incidence of hemorrhagic stroke
- Cancer prevention: No definitive benefit shown in RCTs
- Common cold / immune function: Not clearly supported
- Exception: Vitamins E and C together are used to slow progression of age-related macular degeneration (AMD)
6. Toxicity
- Least toxic of all fat-soluble vitamins
- No toxicity observed at doses of 300 mg/day
- Tolerable Upper Limit: 1,000 mg/day
- Very high doses (>1,000 mg/day) may antagonize vitamin K → increased bleeding tendency (especially in patients already on warfarin)
- May increase risk of hemorrhagic stroke at very high doses
7. Summary - Vitamin E
| Feature | Detail |
|---|---|
| Type | Fat-soluble |
| Forms | Tocopherols (α, β, γ, δ) and Tocotrienols; α-tocopherol most active |
| Most active form | d-α-tocopherol |
| Main function | Chain-breaking lipid-soluble antioxidant in cell membranes and lipoproteins |
| Mechanism | Donates H to lipid peroxyl radicals → tocopheryl radical (unreactive) → regenerated by vitamin C |
| Targets | PUFA in membranes, LDL, RBC membranes, photoreceptors |
| Deficiency (common) | Fat malabsorption, cystic fibrosis, abetalipoproteinemia, premature infants |
| Deficiency features | Hemolytic anemia, spinocerebellar ataxia, peripheral neuropathy, retinopathy |
| RDA | 15 mg/day α-tocopherol equivalents |
| Requirement increases with | ↑ dietary PUFA intake |
| Toxicity | Least toxic fat-soluble vitamin; high doses antagonize vitamin K |
| UL | 1,000 mg/day |
| Clinical trials | Disappointing for CVD, cancer prevention |
Comparison: All Four Fat-Soluble Vitamins
| Feature | Vitamin A | Vitamin D | Vitamin E | Vitamin K |
|---|---|---|---|---|
| Active form | Retinol/Retinoic acid | Calcitriol (1,25-(OH)₂D₃) | α-Tocopherol | Hydroquinone |
| Main function | Vision, epithelial differentiation | Ca²⁺/PO₄ homeostasis | Antioxidant | γ-Carboxylation (coagulation) |
| Deficiency | Night blindness, xerophthalmia | Rickets/Osteomalacia | Hemolysis, ataxia | Bleeding, hypoprothrombinemia |
| Toxicity | Teratogenic, liver damage | Hypercalcemia, metastatic calcification | Antagonizes Vit K | Hemolysis (menadione only) |
| Storage | Liver (Ito cells) | Liver, adipose | Adipose, membranes | Liver |
| Mechanism | Nuclear receptors (RAR/RXR) | Nuclear receptors (VDR/RXR) | Free radical scavenging | Enzyme cofactor (carboxylase) |
Sources: Lippincott Illustrated Reviews: Biochemistry 8th ed, pp. 1094-1101 | Harper's Illustrated Biochemistry 32nd ed, Ch. 44
This is a shared conversation. Sign in to Orris to start your own chat.