leukemoid reaction
Reading File
Finding Sources
Finding Sources
Searching PubMed
"leukemoid reaction"
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive information from multiple authoritative textbooks. Here is the full answer:
Leukemoid Reaction
Definition
A leukemoid reaction is an excessive leukocytic response in the peripheral blood that mimics leukemia but is reactive (non-neoplastic) in origin. It is defined as a WBC count >50,000/μL (50 × 10⁹/L) with a pronounced left shift - the appearance of immature granulocytes (bands, metamyelocytes, myelocytes) in the circulation.
The peripheral blood smear can be virtually indistinguishable from chronic myelogenous leukemia (CML) on morphology alone - distinction depends on specific lab and molecular testing.
Peripheral Blood Smear
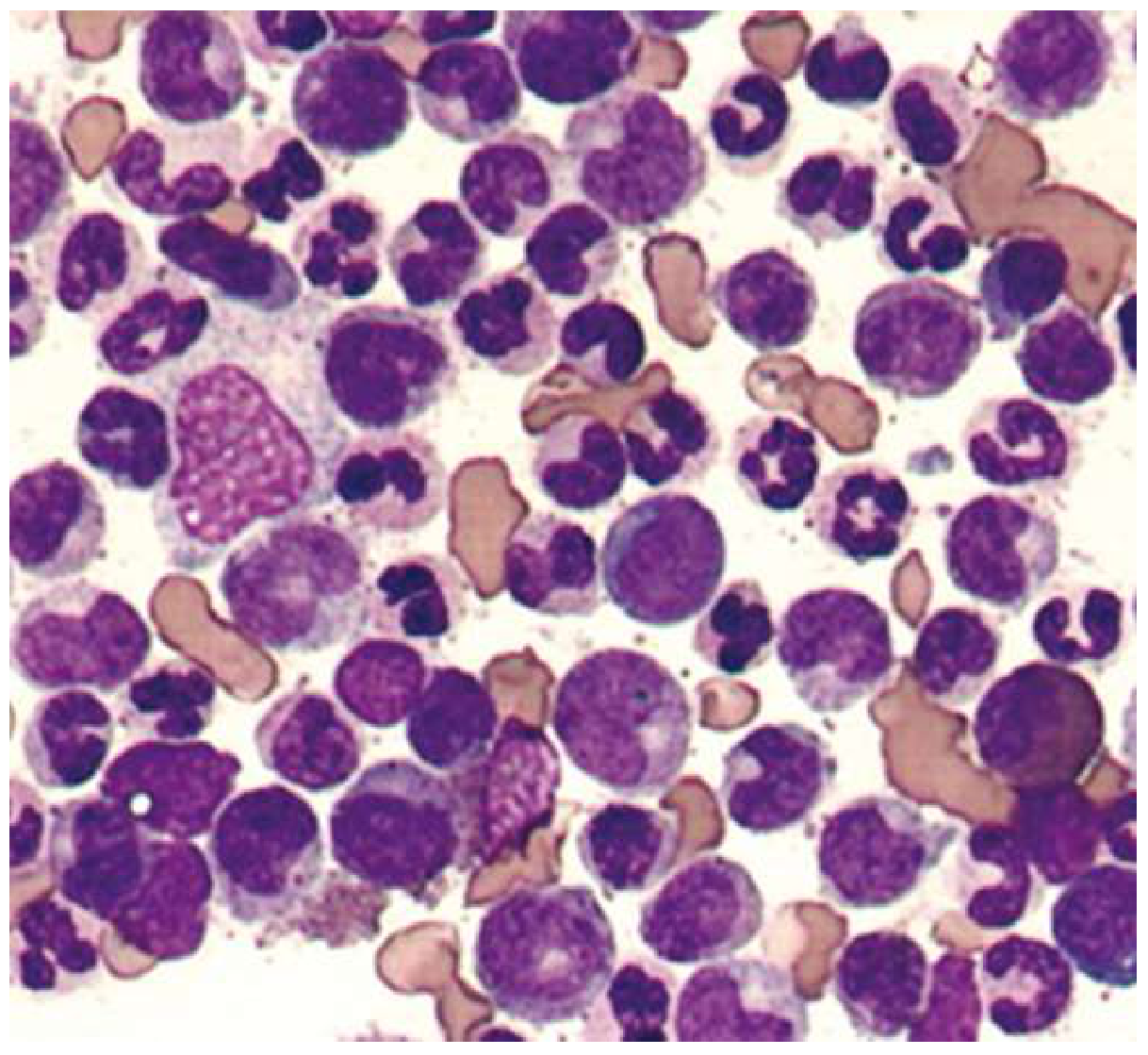
Peripheral blood from a patient with leukemoid reaction. From this smear, it would be impossible to distinguish a leukemoid reaction from chronic phase CML. Distinction depends on the presence or absence of BCR-ABL fusion. (Goldman-Cecil Medicine)
Types
Depending on the predominant cell type:
| Type | Description |
|---|---|
| Neutrophilic | Most common type; reactive neutrophils with left shift, toxic granulation, Döhle bodies, cytoplasmic vacuoles |
| Eosinophilic | Mainly in children; frequently caused by parasitic infection |
| Lymphocytic | Very high counts of normal lymphocytes (e.g., pertussis, infectious lymphocytosis) |
| Monocytic | Less common |
Causes
Neutrophilic leukemoid reactions occur in:
- Severe bacterial infections (e.g., Clostridioides difficile, tuberculosis - WBC can exceed 30,000/μL in ~1/4 of patients, reaching leukemoid threshold)
- Bacterial toxin-mediated infections (e.g., diphtheria)
- Malignancy with bone marrow involvement (e.g., Hodgkin lymphoma, metastatic carcinoma)
- Hemolysis and hemorrhage
- Myelofibrosis
- Severe burns
- Eclampsia
- Rebound granulocytosis
Lymphocytic leukemoid reactions: infectious lymphocytosis, pertussis, infectious mononucleosis (though with atypical cells, distinguishing from leukemia can be difficult)
Morphological Features (Granulocytic Type)
- Left shift: bands, metamyelocytes, myelocytes in peripheral blood
- Toxic granulation - prominent dark cytoplasmic granules
- Döhle bodies - pale blue cytoplasmic inclusions
- Cytoplasmic vacuoles
- These changes indicate a reactive, stressed marrow, not clonal proliferation
Leukoerythroblastosis
When circulating normoblasts (nucleated RBCs) accompany a neutrophilic leukemoid reaction, the term leukoerythroblastic reaction applies. This pattern is seen in:
- Metastatic carcinoma involving the bone marrow
- Marrow fibrosis or infection
- Benign conditions: GI bleeding, hemolytic anemia
Distinguishing Leukemoid Reaction from CML
This is the most clinically important distinction. CML can present identically on the smear.
| Feature | Leukemoid Reaction | CML |
|---|---|---|
| WBC pattern | Left shift, predominantly neutrophils/bands | "Panmyelosis" - all stages of neutrophil series; myelocyte "peak" (more myelocytes than metamyelocytes) |
| Basophilia | Absent | Present (independent adverse prognostic factor) |
| Eosinophilia | Absent | Present |
| Neutrophil Alkaline Phosphatase (NAP/LAP score) | Normal or elevated | Decreased (classic finding) |
| Thrombocytosis + anemia | Usually absent | Often present |
| Splenomegaly | Absent | Common |
| BCR-ABL (Philadelphia chromosome) | Absent | Present (definitive test) |
| Cause | Reactive - identifiable trigger | Clonal neoplasm |
Key mnemonic: In a leukemoid reaction, NAP/LAP score is high (the marrow is working hard reactively). In CML, the leukocytes are clonal and relatively lazy - NAP/LAP is low.
Distinguishing from Chronic Neutrophilic Leukemia (CNL)
CNL is rare: WBC ≥25,000/μL with >80% being segmented neutrophils/bands, <10% immature granulocytes, and hepatosplenomegaly. At least 50% harbor CSF3R mutations. Absence of BCR-ABL is shared with leukemoid reaction, but CSF3R testing and clinical context differentiate them.
Diagnostic Workup
- CBC with peripheral smear - assess morphology, presence of toxic changes
- NAP/LAP score - elevated in leukemoid reaction, low in CML
- BCR-ABL by PCR or FISH - the definitive test; if negative, rules out CML
- Acute phase reactants (CRP, procalcitonin) - elevated in reactive leukocytosis; CRP is an early, sensitive marker
- Bone marrow biopsy - rarely needed for leukemoid reaction alone, but indicated if leukocytosis is unexplained or leukoerythroblastic reaction suggests marrow infiltration; should include cultures for TB/fungi, cytogenetics, flow cytometry
Sources:
- Henry's Clinical Diagnosis and Management by Laboratory Methods, pp. 132, 734
- Goldman-Cecil Medicine, pp. 1763-1764
- Harrison's Principles of Internal Medicine 22E, p. 656
Valvular hear disease ( moderate MR/AR/ AS) Degenerative etiology, hyperkinetic movement disorder ? Left upper limb, chorea / athetosis and sever Anemia
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
This is a rich and clinically challenging constellation. Here is the full integrated analysis:
Clinical Scenario Analysis
The Triad: Degenerative Valvular Disease (MR/AR/AS) + Left Upper Limb Chorea/Athetosis + Severe Anemia
The combination of multivalvular disease, hyperkinetic movement disorder (unilateral, left upper limb), and severe anemia is not random - these three findings point strongly toward a unifying systemic autoimmune diagnosis, most likely Systemic Lupus Erythematosus (SLE) / Antiphospholipid Syndrome (APS), or less commonly rheumatic heart disease with cerebral sequelae.
Step 1 - Unifying Diagnosis Framework
Primary Consideration: SLE + Antiphospholipid Antibody Syndrome (APS)
This single diagnosis explains all three components of the triad:
| Feature | SLE/APS Mechanism |
|---|---|
| Multivalvular disease (MR/AR/AS) | Libman-Sacks endocarditis → scarring, thickening, regurgitation; antiphospholipid antibodies particularly associated with mitral and aortic valve disease |
| Chorea / athetosis (left upper limb) | Antiphospholipid antibodies cause cerebral microthrombi or direct basal ganglia injury → contralateral hemichorea (right basal ganglia/subthalamic nucleus lesion = left-sided movements) |
| Severe anemia | Autoimmune hemolytic anemia (AIHA) - a recognized complication of both SLE and APS |
"Other medical disorders associated with aPLAs include autoimmune hemolytic anemia, livedo reticularis, chorea gravidarum, transverse myelitis, pyoderma-like leg ulcers, and cardiac valve disease." - Creasy & Resnik's Maternal-Fetal Medicine
"Dyskinesias, especially chorea, occur in some patients with SLE, but underlying structural pathology of the basal ganglia is rare; chorea is associated with the presence of antiphospholipid antibodies." - Bradley and Daroff's Neurology in Clinical Practice
Step 2 - Valvular Heart Disease in SLE/APS
Libman-Sacks Endocarditis
- Classic non-infectious (sterile) verrucous vegetations on heart valves in SLE
- Typically on the atrial side of the mitral valve and arterial side of the aortic valve
- Active lesions: immunoglobulins, fibrin, focal necrosis, leukocytic infiltrate
- Healed lesions: fibrous scarring → permanent valve deformity → regurgitation (MR, AR) and occasionally stenosis (AS)
- Vegetations are non-mobile on echo (vs. infective endocarditis where they are mobile and leaflet-independent)
Key Point - Antiphospholipid Antibodies and Valves
Antiphospholipid antibodies (particularly in SLE-APS overlap) are more strongly associated with mitral and aortic valve disease than with the classic Libman-Sacks pattern itself. This can produce moderate-to-severe MR/AR/AS by inflammatory and thrombotic remodeling of valve leaflets.
"It is increasingly recognized that the presence of antiphospholipid antibodies in patients with SLE is more likely to be associated with cardiac valve disease, predominantly the mitral and aortic valve, rather than with Libman-Sacks endocarditis." - Rheumatology, 2-Volume Set (Elsevier)
Calling the etiology "degenerative" on echo reports is common - the chronic fibrotic changes of healed Libman-Sacks or APS-associated valvulitis are often mistaken for degenerative/calcific disease, especially if the autoimmune history is not available.
Step 3 - The Movement Disorder: Left Upper Limb Chorea/Athetosis
Localization
- Chorea (irregular, involuntary, non-patterned movements) and athetosis (slow, writhing, distal movements) localize to basal ganglia dysfunction (striatum - caudate/putamen)
- Unilateral left upper limb involvement = right hemisphere basal ganglia or subthalamic nucleus pathology
- In SLE/APS: this is caused by microthrombi or ischemic lacunar infarcts in the right striatum/subthalamic region, driven by antiphospholipid antibody-mediated thrombosis
Mechanism in APS
- Antiphospholipid antibodies (anti-cardiolipin IgG/IgM, anti-β2-glycoprotein-1, lupus anticoagulant) promote a prothrombotic state
- Small vessel thrombosis in perforating arteries supplying the basal ganglia
- Alternatively, cardioembolic mechanism: valve vegetations from Libman-Sacks endocarditis embolize to the middle cerebral artery territory → striatal infarct → contralateral hemichorea
- Chorea can also occur without structural lesion (antibody-mediated receptor dysfunction at the level of the striatum)
Differential for Hemichorea in This Context
| Cause | Key Features |
|---|---|
| APS-mediated | Most likely; antiphospholipid Ab+, associated with valvulopathy |
| Embolic stroke from Libman-Sacks vegetations | Sudden onset; MRI shows infarct |
| Sydenham's chorea (ARF) | Post-streptococcal; bilateral more common; younger patients; different valvular pattern (pure MR predominantly) |
| Calcific cerebral emboli from degenerative AS | Rare; small calcific showers; sudden |
| SLE cerebral vasculitis | Diffuse CNS disease; other features present |
Step 4 - Severe Anemia in This Context
Most Likely: Autoimmune Hemolytic Anemia (AIHA)
- Direct Coombs test positive
- Present in ~10-15% of SLE patients
- Part of APS spectrum: aPLAs directly associated with AIHA
- Lab: low Hb, elevated LDH, elevated indirect bilirubin, reticulocytosis, spherocytes on smear
Other Contributing Causes to Consider
| Cause | Mechanism |
|---|---|
| AIHA | Anti-RBC autoantibodies (IgG warm type in SLE) |
| Anemia of chronic inflammation | IL-6, hepcidin upregulation suppresses erythropoiesis |
| Microangiopathic hemolytic anemia (MAHA) | Catastrophic APS or TTP-like syndrome |
| Valve-related hemolysis | Turbulent flow across regurgitant/stenotic valves → mechanical RBC destruction; schistocytes on smear; elevated LDH |
| Drug-induced (hydroxychloroquine, azathioprine) | If patient already on SLE therapy |
| Renal involvement | SLE nephritis → EPO deficiency |
The severity of anemia in this scenario likely reflects AIHA ± valve-related hemolysis acting together.
Step 5 - Diagnostic Workup
Confirming the Diagnosis
Autoimmune workup:
- ANA (screening), anti-dsDNA, anti-Sm (SLE specific)
- Antiphospholipid panel: lupus anticoagulant, anti-cardiolipin (IgG/IgM), anti-β2-glycoprotein-1
- Complement levels: C3, C4 (low in active SLE)
- Direct Coombs test (AIHA)
Hematology:
- Peripheral blood smear: spherocytes (AIHA), schistocytes (MAHA/valve hemolysis)
- Reticulocyte count, LDH, indirect bilirubin, haptoglobin
- CBC with differential (thrombocytopenia also common in APS)
Cardiac:
- Transthoracic echo (TEE preferred) - characterize valve lesions, mobile vs. non-mobile vegetations, severity of MR/AR/AS
- Blood cultures (exclude infective endocarditis if febrile)
Neurological:
- MRI brain with DWI - right basal ganglia/subthalamic infarct or signal change
- MRA - assess cerebral vasculature
- Consider CSF if vasculitis suspected
Step 6 - Management Principles
| Problem | Management |
|---|---|
| SLE/APS underlying disease | Hydroxychloroquine (all SLE), immunosuppression (steroids, mycophenolate) for active disease |
| Valvular disease | Serial echo monitoring; anticoagulation (warfarin, target INR 2-3 or 3-4 in high-risk APS) prevents further thrombotic valve damage; valve surgery if hemodynamically significant |
| Chorea | Antiphospholipid Ab-associated chorea: anticoagulation is primary; haloperidol or clonazepam for symptomatic relief; steroids for SLE flare |
| AIHA | Steroids (prednisone 1 mg/kg/day); rituximab for refractory cases; IVIG for acute severe hemolysis; folate supplementation |
| Valve hemolysis | Optimize valve repair/replacement if hemolysis is severe and related to turbulent flow |
Summary - Most Likely Unifying Diagnosis
SLE with antiphospholipid antibody syndrome (APS) explains this entire triad:
- "Degenerative" MR/AR/AS = healed Libman-Sacks endocarditis + APS-mediated valvulitis with fibrous remodeling
- Left upper limb chorea/athetosis = right basal ganglia ischemia from antiphospholipid Ab-mediated thrombosis OR cardioembolism from valve vegetations
- Severe anemia = autoimmune hemolytic anemia (AIHA) ± valve-related mechanical hemolysis
The unifying pathophysiology is antiphospholipid antibody-driven: prothrombotic state affecting cerebral vessels (hemichorea), cardiac valves (multivalvular disease), and red blood cells (AIHA).
Sources:
- Bradley and Daroff's Neurology in Clinical Practice, p. 833
- Braunwald's Heart Disease, pp. 1169-1170 (Libman-Sacks endocarditis)
- Rheumatology 2-Volume Set (Elsevier 2022), pp. 1488-1495 (Valvular disease in SARD)
- Creasy & Resnik's Maternal-Fetal Medicine, p. 1281 (APS manifestations)
This is a shared conversation. Sign in to Orris to start your own chat.