What's milliary Tb
"miliary tuberculosis"[MeSH Terms]
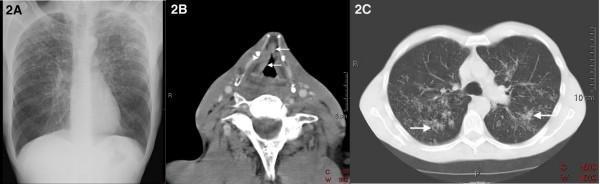
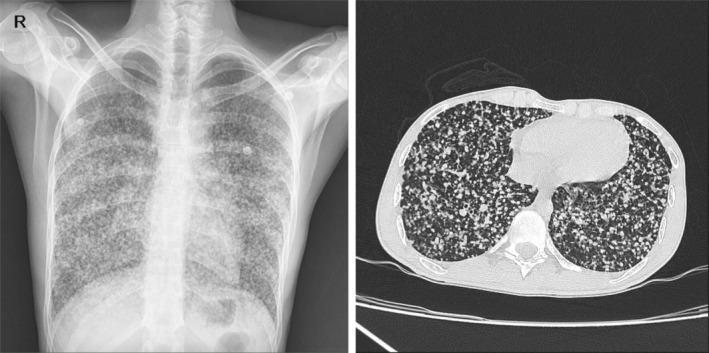
miliary tuberculosis chest X-ray CT scan
Miliary Tuberculosis
Definition & Name Origin
Pathogenesis
- Primary TB (in children, the immunocompromised, or those with impaired cell-mediated immunity)
- Reactivation TB (breakdown of a previously contained focus)
Who Gets It?
- Children and the elderly
- HIV/AIDS patients (most cutaneous cases occur here)
- Those with malnutrition or other immunocompromising conditions
- Post-viral immunosuppression (e.g., measles)
Clinical Features
- Multiorgan failure
- Shock
- ARDS
- Fever, night sweats, weight loss, anorexia
- Nonproductive cough
- Splenomegaly, lymphadenopathy
- Signs of multisystem involvement
- Choroidal tubercles on fundoscopy — pathognomonic for miliary TB
- Cutaneous lesions (seen especially in HIV): papules, vesiculopapules, erythematous macules/pustules, or purpuric "vasculitic" lesions (called tuberculosis cutis milaris disseminata)
Imaging
Histopathology
- Diffuse suppurative inflammation of dermis/subcutis with PMNs ± abscess formation
- Caseating granulomas may be present
- AFB are abundant (unlike other forms of TB where AFB are scarce)
Complications
| Organ | Complication |
|---|---|
| Lungs | ARDS, respiratory failure |
| CNS | TB meningitis (often seeds after miliary infection), tuberculomas |
| Liver | Hepatitis, elevated transaminases |
| Bone marrow | Pancytopenia, anemia |
| Adrenals | Addison disease (formerly a major cause) |
| Vertebrae | Pott disease |
| Genitourinary | Renal TB, fallopian tube involvement, infertility |
| Pleura | Pleural effusion, empyema |
Diagnosis
- Sputum AFB smear and culture (may be negative)
- BAL (bronchoscopy)
- Bone marrow biopsy — highly useful
- Liver biopsy — granulomas + AFB
- Blood cultures (mycobacterial)
- TST/IGRA — often negative due to anergy
- Fundoscopy — look for choroidal tubercles
Treatment
- Intensive phase (2 months): Isoniazid (INH) + Rifampicin + Pyrazinamide + Ethambutol (HRZE)
- Continuation phase (4–7 months): INH + Rifampicin
- Adjunctive corticosteroids are used for TB meningitis and pericarditis to reduce complications
- TB meningitis complicating miliary disease may require ventriculoperitoneal shunting in ~25% of patients for hydrocephalus
Surgery : orthopedic on fractures detailed notes
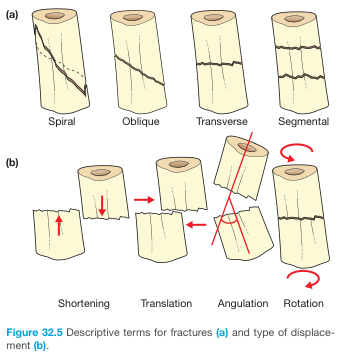
fracture types transverse oblique spiral comminuted bone diagram
Orthopedic Surgery: Fractures — Detailed Notes
1. DEFINITION
2. FRACTURE DESCRIPTION — HOW TO REPORT A FRACTURE
| Parameter | Details |
|---|---|
| Open vs. closed | Does the fracture communicate with outside environment? |
| Bone + side | Name of bone, left vs. right |
| Location | Proximal / middle / distal third; specific region (e.g., humeral neck, tibial plateau) |
| Fracture line direction | Transverse, oblique, spiral, comminuted |
| Completeness | Complete (both cortices) vs. incomplete (one cortex intact) |
| Displacement | Position of distal fragment relative to proximal |
| Alignment/angulation | Valgus, varus, dorsal, volar, rotational |
| Articular involvement | % of articular surface affected |
| Modifiers | Avulsion, impaction, depression, compression, pathologic, stress |
3. FRACTURE TYPES BY FRACTURE LINE PATTERN
| Type | Description | Mechanism |
|---|---|---|
| Transverse | Right angle to long axis of bone | Direct blow / bending force |
| Oblique | Diagonal across the bone | Angulation + axial compression |
| Spiral | Encircles the shaft; appears longer on X-ray | Rotational / torsion force — note: in children, raises suspicion of abuse |
| Comminuted | >2 fragments | High-energy trauma |
| Segmental | Two fracture lines creating a free "floating" segment | High-energy |
| Greenstick | One cortex fractures, one bends (incomplete) | Children; bone still flexible |
| Torus (Buckle) | Bulging of cortex without discrete fracture line | Children; axial compression |
| Avulsion | Bone fragment pulled off by tendon/ligament | Sudden forceful contraction |
| Impaction | One fragment driven into another | Axial force (e.g., proximal humerus in elderly) |
| Stress (March/Fatigue) | Repeated low-intensity forces → bone resorption | Overuse — long-distance running, military recruits |
| Pathologic | Through diseased bone (tumor, cyst, metabolic disease) | Often trivial trauma |
4. DISPLACEMENT AND ALIGNMENT TERMINOLOGY
- Displacement: position of the distal fragment relative to the proximal (by convention); expressed as mm or % of bone width, or qualitatively (none/minimal/moderate/severe)
- Angulation: deviation of the longitudinal axis; described by the direction of the apex
- Valgus: apex toward the midline
- Varus: apex away from midline
- Shortening: fragment overlap reducing overall bone length
- Translation: lateral shift of fragments
- Rotation: twisting of the distal fragment — clinically check by observing the fingers in flexion (scissoring deformity)
5. FRACTURE CLASSIFICATION SYSTEMS
5a. AO/OTA Classification (Universal System)
- Bone number (e.g., 2 = humerus, 3 = radius/ulna, 32 = femur shaft)
- Segment (1 = proximal, 2 = diaphysis, 3 = distal)
- Fracture type (A = simple, B = wedge/partial articular, C = complex/complete articular)
5b. Gustilo–Anderson Classification (Open Fractures)
| Grade | Description |
|---|---|
| I | Wound <1 cm, punctured from inside out, minimal contamination |
| II | Laceration 1–5 cm, no crush, no significant contamination |
| IIIA | >5 cm wound, extensive soft tissue but periosteum intact, coverage possible |
| IIIB | Periosteal stripping, extensive soft tissue loss, requires flap coverage |
| IIIC | Major vascular injury requiring repair (regardless of wound size) |
5c. Salter-Harris Classification (Physeal/Growth Plate Fractures in Children)
| Type | Description | Mnemonic |
|---|---|---|
| I | Through physis only (slipped) | S — Straight through |
| II | Fracture through physis + metaphysis (most common) | A — Above |
| III | Fracture through physis + epiphysis | L — Lower (epiphysis) |
| IV | Through metaphysis + physis + epiphysis | E — Everything |
| V | Crush/compression of physis (worst prognosis) | R — Rammed/crush |
6. FRACTURE HEALING — BIOLOGY
Stages of Fracture Healing (Secondary / Indirect Healing)
| Stage | Timeframe | Key Events |
|---|---|---|
| 1. Hematoma formation | Day 1–3 | Rupture of periosteal blood vessels → hematoma → procallus (no structural rigidity) |
| 2. Inflammatory phase | Days 1–7 | Macrophages, PMNs, cytokines (IL-1, IL-6, TNF); fracture line becomes more visible on X-ray at 10–14 days due to resorption + hyperemia |
| 3. Soft callus (fibrocartilaginous) | Weeks 2–4 | Periosteal + endosteal callus ("biologic splint"); mottled appearance on X-ray; swelling begins to regress |
| 4. Hard callus (bony bridging) | Weeks 4–12 | Callus mineralizes and ossifies; peripheral margins smooth out |
| 5. Remodeling | Months–years | Wolff's Law: bone remodels along lines of stress; eventually indistinguishable from mature bone |
Timeframes for Union (approximate)
| Bone | Time to Union |
|---|---|
| Phalanx/small bones | 3–4 weeks |
| Radius/ulna | 6–8 weeks |
| Humerus | ~8 weeks |
| Tibia | 10–16 weeks |
| Femur | ~4 months |
Primary (Direct) Healing
Mechanobiology — Interfragmentary Strain Theory (Perren)
- Strain = deformation / original length
- High strain environment → granulation tissue / fibrous tissue
- Intermediate strain → fibrocartilage
- Low strain → bone formation
- Zero strain ≠ optimal — some motion/load is necessary to stimulate callus
- Simple fractures with bridge plating (rigid but not anatomically reduced) → high nonunion rates
- Dynamic locking implants that allow symmetric motion → improved callus formation — Rockwood & Green's
7. ABNORMAL FRACTURE HEALING
| Term | Definition |
|---|---|
| Delayed union | Union occurring slower than expected for that fracture type/location |
| Malunion | Fracture heals with residual deformity (angulation, rotation, shortening) |
| Nonunion | Complete failure to heal; defined radiographically as no progressive healing over 3–6 months |
| Pseudarthrosis | Nonunion resulting in a false joint with motion at the fracture site |
- Hypertrophic (elephant foot): abundant callus, adequate vascularity — inadequate stability is the cause; treat with fixation
- Atrophic: no callus, poor vascularity — treat with bone graft + fixation
8. OPEN FRACTURES — EMERGENCY MANAGEMENT
- Control hemorrhage with sterile pressure dressing; remove gross debris
- Splint without reduction (unless vascular compromise)
- Irrigate with saline; cover with saline-soaked sponges
- Antibiotics as early as possible:
- Grade I: 1st-generation cephalosporin (cefazolin 2 g IV q8h)
- Grade II/III: add aminoglycoside (gentamicin 5 mg/kg OD) or broad-spectrum (piperacillin-tazobactam)
- Farm/fecal contamination: add ampicillin/penicillin (cover Clostridium)
- Tetanus prophylaxis (including TIG for large crush wounds)
- Surgical debridement + irrigation within 24 hours (the historical 6-hour rule is no longer strictly evidence-based)
- Stabilization (external fixator → definitive fixation)
9. COMPLICATIONS OF FRACTURES
Immediate
| Complication | Key Points |
|---|---|
| Hemorrhage | Femur: ~1000 mL; Pelvis: 1500–3000 mL; Tibia/fibula: ~500 mL; Forearm: 150–250 mL. Splinting reduces blood loss. |
| Vascular injury | Popliteal artery with knee dislocation/distal femur; brachial artery with supracondylar humerus fracture in children |
| Nerve injury | See table below |
| Fracture | Nerve at Risk |
|---|---|
| Distal radius (high energy) | Median nerve |
| Elbow fracture/dislocation | Median or ulnar nerve |
| Humeral shaft (mid/distal) | Radial nerve (Saturday night palsy pattern) |
| Shoulder dislocation | Axillary nerve |
| Sacral fracture | Cauda equina |
| Acetabular fracture | Sciatic nerve |
| Hip dislocation | Femoral nerve |
| Lateral tibial plateau | Peroneal nerve |
| Knee dislocation | Tibial or peroneal nerve |
- Neuropraxia: contusion/traction, axon intact — recovers in weeks to months
- Axonotmesis: axon + myelin disrupted, connective tissue intact — Schwann tubes guide spontaneous recovery (delayed)
- Neurotmesis: complete severing of nerve + stroma — requires surgical repair
Early
- Increased pressure within a closed fascial compartment → ischemia of muscle and nerves
- Most common after: tibial shaft fractures (40%), forearm fractures (18%)
- Classic signs: 5 P's — Pain (especially with passive stretch), Pressure (tense compartment), Paresthesia, Paralysis (late), Pallor/Pulselessness (very late)
- Compartment pressure >30 mmHg (or within 30 mmHg of diastolic pressure) = indication for fasciotomy
- Treatment: urgent four-compartment, two-incision fasciotomy (leg); wounds left open; negative pressure wound therapy; definitive fracture fixation follows
- Sequelae if missed: Volkmann's ischemic contracture, myonecrosis, rhabdomyolysis, renal failure, amputation
- Primarily in open fractures
- Prophylactic antibiotics ± surgical debridement essential
Late
| Complication | Notes |
|---|---|
| Avascular necrosis (AVN) | Disruption of blood supply; classic in femoral head (hip dislocation/neck fracture), scaphoid, talus |
| Post-traumatic arthritis | Intra-articular fractures with >2 mm step-off |
| Malunion | Malalignment, limb length discrepancy, gait problems |
| Nonunion | Hypertrophic or atrophic |
| Reflex sympathetic dystrophy (CRPS) | Burning pain, swelling, skin changes, osteoporosis |
| Fat embolism syndrome | Long bone / pelvic fractures; classic triad: hypoxia + confusion + petechiae; treat with O2 + early fixation |
| DVT/PE | Especially pelvic, hip, femur fractures; prophylaxis mandatory |
| Myositis ossificans | Heterotopic ossification in soft tissue at fracture site |
10. FRACTURE TREATMENT PRINCIPLES
Goals of Treatment (The 4 R's)
- Recognition — history, clinical examination, imaging
- Reduction — restore normal anatomic alignment
- Retention — hold fragments in position until union
- Rehabilitation — restore function
Methods of Reduction
- Closed reduction: manipulation under anesthesia/sedation; splint/cast applied
- Open reduction: surgical exposure to achieve anatomic reduction
- Traction: skin or skeletal traction (less common now)
Methods of Fixation (Retention)
| Method | Details | Indication |
|---|---|---|
| Plaster/Cast | Non-operative; 3-point moulding | Stable, undisplaced fractures; children |
| Functional brace | Allows early joint motion | Humeral shaft, tibial shaft |
| Traction | Skin or skeletal (tibial pin, femoral pin) | Femoral shaft, pre-op temporizing |
| External fixation (EF) | Frame + transcutaneous pins/wires | Open fractures, polytrauma, damage control, infected nonunion |
| Intramedullary nail (IMN) | Rod through medullary canal, locked proximally and distally | Diaphyseal fractures: femur, tibia, humerus — "load-sharing" device |
| Plates & screws | Applied to bone surface | Periarticular fractures, forearm (requires anatomic reduction for rotation); "load-bearing" device |
| Cannulated screws | Percutaneous | Hip fractures (Garden I/II), scaphoid fractures |
| Arthroplasty (hemi/total) | Replace femoral head/hip | Displaced femoral neck fractures in elderly (Garden III/IV) |
Absolute Stability vs. Relative Stability
- Absolute stability (compression plate, lag screw): primary bone healing, no callus
- Relative stability (IMN, bridge plate, external fixator): secondary bone healing with callus — requires some motion
11. SPECIFIC IMPORTANT FRACTURES
Colles' Fracture
- Distal radius fracture with dorsal displacement and volar apex angulation → "dinner fork" deformity
- Mechanism: FOOSH (fall on outstretched hand) in extension
- Most common in osteoporotic elderly women
- May involve ulnar styloid
- Nerve at risk: median nerve
- Treatment: closed reduction + cast if acceptable alignment; ORIF if unstable or intra-articular
Smith's Fracture
- "Reverse Colles'" — volar displacement of distal radius
- Mechanism: fall on flexed wrist
- Inherently unstable → usually needs ORIF
Scaphoid Fracture
- Most common carpal fracture
- Mechanism: FOOSH in dorsiflexion
- Often X-ray negative initially → MRI or CT needed if clinical suspicion
- Risk of AVN of the proximal pole (tenuous blood supply from distal end)
- Treatment: undisplaced → thumb spica cast 8–12 weeks; displaced → ORIF with headless compression screw
Hip Fractures (Proximal Femur)
| Grade | Description |
|---|---|
| I | Incomplete/valgus impacted — stable |
| II | Complete, undisplaced |
| III | Complete, partially displaced |
| IV | Complete, fully displaced |
- Garden I & II: cannulated screws or dynamic hip screw (DHS)
- Garden III & IV (elderly): hemiarthroplasty or total hip replacement; risk of AVN with fixation
- Intracapsular disrupts the medial femoral circumflex artery → AVN risk
- Intertrochanteric (extracapsular): DHS or cephalomedullary nail (CMN)
- Subtrochanteric: cephalomedullary nail
Femoral Shaft Fracture
- Requires high-energy trauma (MVA, fall from height)
- Blood loss ~1000 mL → monitor for hypovolemic shock
- Treatment: intramedullary nail (locked IM nail) — gold standard
- Nerve risk: peroneal nerve (from associated traction/positioning injury)
Tibial Shaft Fracture
- Most common long bone fracture requiring surgical treatment
- Scanty subcutaneous soft tissue → high risk of open fracture and compartment syndrome (40% of all compartment syndromes)
- Treatment: IM nail for displaced/unstable; cast for undisplaced
Pelvic Fractures
- Can cause catastrophic hemorrhage (1.5–3 L)
- Life-threatening: pelvic binder/sheet applied in the field for open-book fractures to close the pelvis
- Definitive: external fixation or internal fixation; interventional radiology embolization
Spinal Fractures (AO Spine Classification)
- Type A: Compression/burst — vertebral body compression
- Type B: Distraction — tension band injury
- Type C: Translational/rotational — most unstable
- Pott's disease = vertebral TB (collapse + kyphus)
- Neurological status guides urgency of intervention
12. PEDIATRIC-SPECIFIC CONSIDERATIONS
- Growth plate (physis) is the weakest area in children → Salter-Harris fractures
- Children's bones are more plastic → greenstick and torus fractures
- Remodeling potential is significant → greater tolerance for angulation (varies with age and proximity to physis)
- Spiral fractures in non-ambulatory children raise suspicion for non-accidental injury (child abuse)
- Supracondylar humerus fracture (most common elbow fracture in children): risk of anterior interosseous nerve injury and brachial artery injury → urgent reduction; "Gartland type III" needs emergency ORIF with K-wires
13. OSTEOPOROTIC (FRAGILITY/INSUFFICIENCY) FRACTURES
- Occur with low-energy trauma (from standing height or less)
- Common sites: distal radius, vertebrae, hip, proximal humerus
- Every fragility fracture mandates assessment and treatment for underlying osteoporosis
- Post-hip fracture: zoledronic acid or denosumab significantly reduce all-cause mortality
- Atypical femur fractures (AFFs): rare complication of long-term bisphosphonate use — lateral subtrochanteric, transverse, may be bilateral; prodromal thigh pain
14. LIFE-THREATENING & LIMB-THREATENING EMERGENCIES — SUMMARY TABLE
| Emergency | Complication |
|---|---|
| Open fracture | Osteomyelitis |
| Fracture/dislocation with vascular disruption (esp. popliteal) | Amputation |
| Major pelvic fracture | Exsanguination |
| Hip dislocation | AVN of femoral head |
| Compartment syndrome | Ischemic contracture; amputation; renal failure |
Generate sets of possible questions in it with answers exam oriented
Pediatrics 1 topics overview
Pediatrics 1 — Detailed Notes
Growth, Development, Nutrition & Neonatology
TOPIC 1: GROWTH & ANTHROPOMETRY
A. Growth Parameters
- Weight
- Length/Height
- Head Circumference (OFC — Occipito-Frontal Circumference)
- BMI (from age 2 years)
Normal Birth Parameters (Term Infant)
| Parameter | Normal Value |
|---|---|
| Birth weight | 2.5–4.0 kg (average ~3.4 kg) |
| Length | 48–52 cm |
| Head circumference | 33–35 cm |
Weight Gain Patterns
| Age | Expected Weight Gain |
|---|---|
| First 3–4 days | Lose up to 10% of birth weight (physiologic) |
| By day 10–14 | Regain birth weight |
| 0–3 months | ~30 g/day (200 g/week) |
| 3–6 months | ~20 g/day |
| 6–12 months | ~15 g/day |
| 5 months | Double birth weight |
| 12 months | Triple birth weight |
| 24 months | Quadruple birth weight |
Height/Length Growth
| Age | Expected Growth |
|---|---|
| Year 1 | +25 cm (~50% increase) |
| Year 2 | +12 cm |
| Year 3 | +9 cm |
| Year 4 onwards | ~6–7 cm/year until puberty |
| 4 years | Double birth length |
Head Circumference Growth
| Age | Growth Rate |
|---|---|
| Month 1–3 | ~2 cm/month |
| Month 3–6 | ~1 cm/month |
| Month 6–12 | ~0.5 cm/month |
| At 1 year | ~47 cm |
| At 2 years | ~49 cm (adult = ~57 cm) |
Classification by Size for Gestational Age
| Classification | Percentile | Risk |
|---|---|---|
| AGA (Appropriate for Gestational Age) | 10th–90th | Normal |
| SGA (Small for Gestational Age) | <10th | Hypoglycemia, hypothermia |
| LGA (Large for Gestational Age) | >90th | Hypoglycemia, birth trauma; often IDM |
Fontanels:
- Anterior fontanel: 4–6 cm; closes at 9–18 months
- Posterior fontanel: <1 cm; closes by 6–8 weeks
- Bulging = raised ICP | Large = hypothyroidism | Early closure = craniosynostosis
B. Pubertal Growth — Tanner Stages (briefly)
- Girls: Puberty begins 8–13 years; breast budding (thelarche) is first sign
- Boys: Puberty begins 9–14 years; testicular enlargement is first sign
- Pubertal growth spurt: Girls ~10–11 years; Boys ~12–13 years
TOPIC 2: DEVELOPMENTAL MILESTONES
A. Milestone Table (CDC/AAP 2022 Standards)
| Age | Gross Motor | Fine Motor | Language | Social/Cognitive |
|---|---|---|---|---|
| 2 months | Holds head up on tummy; moves all limbs | Opens hands briefly | Cooing sounds; reacts to loud sounds | Smiles socially; calms to voice |
| 4 months | Holds head steady unsupported; pushes up on elbows | Holds toy placed in hand; brings hands to mouth | Cooing "ooo/aah"; turns to voice | Chuckles; makes sounds to get attention |
| 6 months | Rolls tummy→back; pushes up on straight arms | Reaches and grasps; transfers objects hand-to-hand | Babbles ("mamamama"); takes turns making sounds | Recognises familiar people; laughs; mirror interest |
| 9 months | Sits without support; pulls to stand beginning | Pincer grasp developing; "rakes" food | Babbles "ma-ma, ba-ba"; lifts arms to be picked up | Stranger anxiety; waves bye-bye; plays peek-a-boo |
| 12 months | Pulls to stand; cruises furniture; may take first steps | Mature pincer grasp | Says "mama/dada" specifically; understands "no"; 1–3 words | Plays pat-a-cake; drinks from cup with help |
| 15 months | Walks independently; stoops to pick up toy | Stacks 2 blocks; scribbles | 1–2 words besides mama/dada; points to ask | Copies other children; hugs toys; shows affection |
| 18 months | Walks well; runs stiffly; kicks ball | Stacks 4 blocks; uses spoon | 10–25 words; says own name | Points to show interest; pretend play begins |
| 24 months | Runs well; kicks ball; walks up stairs with help | Stacks 6 blocks; scribbles circles | 2-word phrases ("More milk"); 50+ words | Parallel play; copies actions; uses "I/me/we" |
| 30 months | Jumps with both feet; turns doorknobs | Turns book pages one at a time | 50+ words; 2-word phrases with action word | Pretend play; follows 2-step instructions; knows 1 color |
| 3 years | Rides tricycle; runs well; walks up stairs alternating feet | Uses fork; strings beads; draws circle | 3-word sentences; "who/what/where" questions; 75% intelligible | Plays with other children; names |
| 4 years | Hops on one foot; catches bounced ball | Draws a person with 3+ parts; uses scissors | 4+ word sentences; tells stories; 100% intelligible | Pretend play (roles); comforts others; follows rules |
| 5 years | Skips; walks heel-to-toe | Copies triangle; prints some letters | Full sentences; tells longer stories | Distinguishes fantasy from reality; cooperative play |
B. Developmental "Red Flags" (Absolute Indicators for Referral)
| Age | Red Flag |
|---|---|
| Any age | Loss of previously acquired skills (regression) — always abnormal |
| Any age | Hearing loss; vision concerns; persistent low muscle tone; asymmetric movements |
| Any age | Head circumference >99.6th or <0.4th centile, or crossing 2 centile lines |
| 5 months (corrected) | Cannot hold object placed in hand |
| 6 months (corrected) | Not reaching for objects |
| 12 months | Cannot sit unsupported |
| 18 months | Not walking (boys); not pointing to share interest |
| 24 months | Not walking (girls); no 2-word phrases |
| Any age | No babbling by 12 months; no words by 16 months; no 2-word spontaneous phrases by 24 months |
Key Rule: Any regression (loss of skills) at any age = immediate evaluation for metabolic, neurological, or neurodegenerative disease.
C. Developmental Screening Tools
- ASQ (Ages & Stages Questionnaire) — parent-completed; 0–66 months
- MCHAT-R (Modified Checklist for Autism in Toddlers) — autism screening at 18 and 24 months
- Denver II (DDST) — widely used; 4 domains; birth to 6 years
D. Developmental Theories
| Theorist | Theory | Key Concepts |
|---|---|---|
| Piaget | Cognitive development | Sensorimotor (0–2 yr) → Preoperational (2–7 yr) → Concrete operational (7–12 yr) → Formal operational (12+) |
| Erikson | Psychosocial development | Trust vs. Mistrust (0–1); Autonomy vs. Shame (1–3); Initiative vs. Guilt (3–6); Industry vs. Inferiority (6–12) |
| Freud | Psychosexual | Oral (0–1); Anal (1–3); Phallic (3–6); Latency (6–12); Genital (12+) |
| Vygotsky | Sociocultural | Zone of Proximal Development (ZPD); scaffolding |
TOPIC 3: PRIMITIVE NEONATAL REFLEXES
| Reflex | Elicitation | Normal Duration | Note |
|---|---|---|---|
| Moro | Abruptly lower supine infant → arms abduct/extend, then flex ("embrace") | Birth → 4–6 months | Absent = severe CNS injury; asymmetric = brachial plexus injury |
| Rooting | Stroke skin near mouth → infant turns toward stimulus | Birth → 3–4 months | Facilitates breastfeeding |
| Palmar grasp | Press on palm → infant grabs finger | Birth → 3–4 months | Replaced by voluntary grasp |
| Plantar grasp | Press plantar surface → toes curl | Birth → 3–4 months | |
| Stepping | Hold upright with feet on surface → alternating stepping movements | Birth → 1–2 months | Reappears as voluntary walking ~12 months |
| Asymmetric Tonic Neck (ATNR) | Turn head to one side → ipsilateral limbs extend, contralateral flex ("fencing posture") | Birth → 2–4 months | Persistence beyond 6 months = cerebral palsy |
| Galant | Stroke paravertebral back → trunk curves toward stimulus | Birth → 2 months | |
| Babinski | Stroke lateral sole upward → great toe dorsiflexes, others fan | Normal in infants up to 2 years | Abnormal in adults = upper motor neuron lesion |
| Parachute | Held prone, then moved face-down rapidly → arms extend to "catch" | Appears ~6–9 months, persists lifelong | Absence = cerebral palsy concern |
Key: Persistence of primitive reflexes beyond their expected time = abnormal, suggests CNS dysfunction.
TOPIC 4: NEONATOLOGY
A. Apgar Score (Assessed at 1 and 5 Minutes)
| Sign | 0 | 1 | 2 |
|---|---|---|---|
| Appearance (color) | Blue/pale | Blue extremities, pink body | Completely pink |
| Pulse (heart rate) | Absent | <100/min | ≥100/min |
| Grimace (reflex irritability) | No response | Grimace | Cough, sneeze, cry |
| Activity (muscle tone) | Limp | Some flexion | Active motion |
| Respiration | Absent | Irregular/slow | Strong cry |
- 7–10: Normal
- 4–6: Moderately depressed — stimulate and give O₂
- 0–3: Severely depressed — immediate resuscitation
Apgar is assessed at 1 min (need for resuscitation) and 5 min (efficacy). If <7 at 5 min, repeat every 5 minutes up to 20 min. Do NOT delay resuscitation to calculate Apgar.
B. Gestational Age Assessment — New Ballard Score
Neuromuscular Maturity
- Posture
- Square window (wrist flexion angle)
- Arm recoil
- Popliteal angle
- Scarf sign
- Heel-to-ear
Physical Maturity
- Skin (thin/transparent → thick/leathery)
- Lanugo (abundant → none)
- Plantar creases
- Breast tissue
- Ear cartilage
- Genitalia
- If discrepancy >1 week between dates and Ballard: use earlier gestational age
C. Gestational Age Classification
| Category | Gestational Age |
|---|---|
| Extremely preterm | <28 weeks |
| Very preterm | 28–32 weeks |
| Moderate/Late preterm | 32–37 weeks |
| Term | 37–42 weeks |
| Post-term | >42 weeks |
D. Newborn Physical Examination Highlights
- Clamp and cut umbilical cord (delayed clamping 30–60 sec recommended)
- Umbilical cord: 2 arteries + 1 vein (single artery → renal anomalies)
- Vitamin K IM, eye prophylaxis (erythromycin), Hepatitis B vaccine at birth
| Lesion | Key Features |
|---|---|
| Caput succedaneum | Scalp edema; crosses suture lines; present at birth; resolves in days |
| Cephalohematoma | Subperiosteal blood; does NOT cross suture lines; appears hours after birth; resolves weeks–months; risk of jaundice |
| Subgaleal hematoma | Most dangerous; crosses suture lines; can cause massive blood loss |
E. Common Neonatal Skin Conditions
| Condition | Features | Management |
|---|---|---|
| Erythema toxicum neonatorum (ETN) | Multiple erythematous macules/papules → pustules; trunk/proximal limbs; spares palms/soles; appears 24–48 hr, resolves 5–7 days | Reassure; Eosinophils on Wright stain |
| Transient neonatal pustular melanosis (TNPM) | Superficial pustules → hyperpigmented macules; more in dark-skinned infants | Self-limited; reassure |
| Milia | Tiny white pearly papules on nose/cheeks; blocked sebaceous glands | Resolve spontaneously in weeks |
| Mongolian spots | Blue-grey hyperpigmented macules; sacral/buttock area; more in Asian/African-American infants | Benign; document to avoid confusion with bruising |
| Salmon patch (stork bite/angel kiss) | Flat pink/red capillary malformation; nape of neck, eyelids | Most resolve by 1–2 years |
| Port wine stain | Dark red, unilateral; face | Permanent; if in V1/V2 → Sturge-Weber syndrome; refer |
F. Neonatal Jaundice
Physiologic vs. Pathologic
| Feature | Physiologic | Pathologic |
|---|---|---|
| Onset | >24 hours after birth | <24 hours — always pathological |
| Type | Unconjugated (indirect) | Can be conjugated or unconjugated |
| Peak | Day 3–5 (term); Day 5–7 (preterm) | Varies |
| Duration | <2 weeks (term); <3 weeks (preterm) | >2 weeks |
| Cause | Increased RBC breakdown + immature hepatic conjugation + increased enterohepatic circulation | Hemolysis (ABO, Rh incompatibility), G6PD, sepsis, biliary atresia |
Bilirubin and Zones of Jaundice (Kramer's Rule)
- Zone 1: Face — bilirubin ~5 mg/dL
- Zone 2: Chest — ~10 mg/dL
- Zone 3: Abdomen — ~12 mg/dL
- Zone 4: Legs — ~15 mg/dL
- Zone 5: Palms/soles — >20 mg/dL (severe; risk of kernicterus)
Causes of Pathologic Jaundice
- <24 hr: Hemolytic disease (Rh/ABO incompatibility), G6PD deficiency, sepsis
- 2–14 days: ABO incompatibility, spherocytosis, polycythemia, breast milk jaundice
- >2 weeks (persistent): Biliary atresia (conjugated ↑), hypothyroidism, breast milk jaundice (unconjugated)
Management
- Phototherapy: most common treatment; blue-green light (wavelength 460–490 nm) converts bilirubin to water-soluble isomers
- Exchange transfusion: for severe hyperbilirubinemia unresponsive to phototherapy or imminent kernicterus
- Kernicterus (Bilirubin encephalopathy): Unconjugated bilirubin crosses BBB → basal ganglia/hippocampus damage → choreoathetosis, sensorineural deafness, upward gaze palsy, intellectual disability
G. Prematurity and its Complications
| Complication | Details |
|---|---|
| Respiratory Distress Syndrome (RDS/HMD) | Surfactant deficiency; ground-glass appearance on CXR; treat with exogenous surfactant + CPAP/ventilation |
| Intraventricular Hemorrhage (IVH) | Germinal matrix bleed; graded I–IV; Grade III/IV → hydrocephalus, neurodevelopmental disability |
| Necrotizing Enterocolitis (NEC) | Gut ischemia + bacterial invasion; bloody stools, abdominal distension, pneumatosis intestinalis on X-ray |
| Retinopathy of Prematurity (ROP) | Abnormal retinal vascularization; screen all <30 weeks or <1500 g; treat with laser/anti-VEGF |
| Patent Ductus Arteriosus (PDA) | Failure of DA to close; continuous "machine" murmur; indomethacin or ligation |
| Apnea of Prematurity | Central; treat with caffeine (methylxanthine) |
| Hypoglycemia | SGA, LGA (IDM), preterm; BG <45 mg/dL requires treatment |
TOPIC 5: PEDIATRIC NUTRITION
A. Breastfeeding
Benefits of Breastfeeding
| For Infant | For Mother |
|---|---|
| Optimal nutrition (changes with infant needs) | Reduced postpartum hemorrhage (oxytocin release) |
| Passive immunity (sIgA, macrophages, lactoferrin) | Reduced risk of breast/ovarian cancer |
| Reduced risk of otitis media, GI infections, URTI | Promotes uterine involution |
| Reduced risk of SIDS, obesity, type 1 DM | Promotes bonding; contraceptive effect (LAM) |
| Promotes mother-infant bonding |
Composition of Breast Milk
| Type | When | Characteristics |
|---|---|---|
| Colostrum | First 2–5 days | Yellow, thick; high in antibodies (IgA), low in fat; laxative effect (meconium) |
| Transitional | Days 5–14 | Increasing fat and lactose |
| Mature milk | After 2 weeks | Foremilk (watery, quenches thirst) → Hindmilk (high fat, calorie-dense) |
Contraindications to Breastfeeding
- Maternal: HIV (in developed countries), active untreated TB (until 2 weeks of treatment), HTLV-1/2, active herpes lesions on breast, certain chemotherapy agents
- Infant: Galactosemia (classic), phenylketonuria (partial restriction)
- NB: Hepatitis B/C, CMV, and most medications are NOT absolute contraindications
B. Formula Feeding
- Standard infant formula: 20 kcal/oz (same as breast milk)
- Cow's milk–based formula (most common)
- Soy formula: for galactosemia, cow's milk protein allergy
- Whole cow's milk: NOT before 12 months (inadequate iron, high renal solute load)
- Honey: NOT before 12 months (risk of infant botulism)
C. Complementary Feeding (Weaning)
| Age | Recommendation |
|---|---|
| 0–6 months | Exclusive breastfeeding (or formula) |
| ~6 months | Introduce complementary solid foods; continue breastfeeding |
| Introduction order | Iron-fortified cereals, pureed vegetables, fruits, then meats |
| No honey | Until 12 months (botulism risk) |
| No whole cow's milk | Until 12 months |
| No added salt/sugar | <2 years |
| No juice | <12 months; limit to 4 oz/day 1–3 years |
- Sits with minimal support
- Shows interest in food
- Loss of extrusion reflex
- Head control established
D. Nutritional Requirements
| Nutrient | Notes |
|---|---|
| Calories | Infants: ~100 kcal/kg/day; decreases with age |
| Protein | 1.5–2 g/kg/day (infants); 1 g/kg/day (older children) |
| Vitamin D | 400 IU/day from birth (all breastfed infants + formula-fed if <1L/day formula) |
| Iron | Breastfed infants: 1 mg/kg/day supplement from 4 months; formula already iron-fortified. Introduce iron-rich foods at 6 months |
| Fluoride | Supplement if water not fluoridated; start at 6 months |
| Vitamin K | IM at birth to prevent hemorrhagic disease of newborn |
E. Malnutrition
Classification (WHO — Weight-for-Height or MUAC)
| Type | Weight/Height Z-score | Clinical Features |
|---|---|---|
| Moderate Acute Malnutrition (MAM) | -3 to -2 SD | Visible wasting |
| Severe Acute Malnutrition (SAM) | <-3 SD or MUAC <115 mm | Requires therapeutic feeding |
| Marasmus | Severe caloric deficiency | Wasted, "old man face," baggy pants skin, no edema |
| Kwashiorkor | Severe protein deficiency | Edema (pitting), skin changes (crazy-paving), hair changes (flag sign), hepatomegaly, moon face |
| Marasmic-Kwashiorkor | Mixed | Both wasting AND edema |
TOPIC 6: IMMUNIZATION / VACCINATION
Principles
- Active immunity: vaccine stimulates own immune response (live-attenuated or inactivated/subunit/toxoid)
- Passive immunity: pre-formed antibodies (immunoglobulins, maternal transfer)
- Live vaccines contraindicated in immunocompromised children and pregnancy
Key Live-Attenuated Vaccines
| Vaccine | Disease |
|---|---|
| OPV (oral polio) / now IPV in many countries | Poliomyelitis |
| MMR | Measles, Mumps, Rubella |
| Varicella (VZV) | Chickenpox |
| BCG | Tuberculosis (given at birth in endemic countries) |
| Rotavirus | Rotavirus gastroenteritis |
| Yellow fever | Yellow fever |
Typical Expanded Programme on Immunization (EPI) Schedule (WHO-based)
| Age | Vaccines |
|---|---|
| Birth | BCG, OPV-0, HBV-1 (Hepatitis B) |
| 6 weeks | DPT-1 (Diphtheria, Pertussis, Tetanus), OPV-1/IPV-1, HBV-2, Hib-1, PCV-1, Rota-1 |
| 10 weeks | DPT-2, OPV-2/IPV-2, HBV-3, Hib-2, PCV-2, Rota-2 |
| 14 weeks | DPT-3, OPV-3/IPV-3, Hib-3, PCV-3, Rota-3 |
| 9 months | Measles (or MMR), Yellow fever (endemic areas), MenA |
| 12–15 months | MMR booster, Varicella, PCV booster |
| 15–18 months | DPT booster (DTP-4) |
| 4–6 years | MMR-2, DPT-5, OPV-5 |
Specific countries (Nigeria/West Africa): BCG at birth is standard; MMR at 9 months + 15 months.
TOPIC 7: WELL-CHILD CARE (Preventive Pediatrics)
Well-Child Visit Schedule (AAP)
- Growth monitoring — plot weight, height, OFC, BMI on WHO/CDC charts
- Developmental surveillance — parental concerns, direct observation
- Formal developmental screening at 9, 18, 30 months + autism screening 18 & 24 months
- Immunizations per schedule
- Anticipatory guidance — safety, nutrition, sleep, dental health, screen time
- Physical exam — with age-appropriate focus
- Vision and hearing screening
- Hematocrit/lead screening (at 9–12 months in high-risk)
SUMMARY — KEY FACTS TO MEMORIZE
| Fact | Value |
|---|---|
| Birth weight doubles by | 5 months |
| Birth weight triples by | 12 months |
| Birth weight quadruples by | 24 months |
| Birth length doubles by | 4 years |
| Anterior fontanel closes | 9–18 months |
| Posterior fontanel closes | 6–8 weeks |
| First word (other than mama/dada) | ~12 months |
| 2-word phrases | ~24 months |
| Walks independently | ~12 months |
| Sits unsupported | ~6–9 months |
| Apgar normal | 7–10 |
| Apgar — repeat if <7 at 5 min | Every 5 min up to 20 min |
| Exclusive breastfeeding until | 6 months |
| Complementary foods start | ~6 months |
| No whole cow's milk until | 12 months |
| No honey until | 12 months |
| Vitamin D supplement in breastfed infants | 400 IU/day from birth |
| Iron supplement in breastfed infants | 1 mg/kg/day from 4 months |
| Physiologic jaundice onset | >24 hours after birth |
| Pathologic jaundice onset | <24 hours = always abnormal |
| Moro reflex disappears by | 4–6 months |
| ATNR persistence beyond | 6 months = abnormal (CP) |
Can generate sets of questions for revision exam oriented
How to take comprehensive history taking of obs and gynae smart memory aid
Obs & Gynae History Taking — Comprehensive Smart Memory Aid
THE MASTER MNEMONIC: "CAMPS-SOFAS"
Use this to never miss a section: Chief complaint → Antenatal/Obstetric history → Menstrual history → Present illness → Sexual & Contraception → Systemic/PMH → Obstetric (previous) → Family history → Allergies & Drugs → Social history
PART A: GYNAECOLOGICAL HISTORY
STEP 1 — PRESENTING COMPLAINT (PC)
| Letter | Question |
|---|---|
| Site | Where is it? |
| Onset | When did it start? Sudden or gradual? |
| Character | Nature of symptoms (burning, cramping, sharp) |
| Radiation | Does it spread anywhere? |
| Associating symptoms | Bleeding? Discharge? Fever? Nausea? |
| Time course | Constant or intermittent? Getting worse? |
| Exacerbating/relieving | Worse with intercourse? Periods? Better with analgesia? |
| Severity | 1–10 score / functional impact |
STEP 2 — MENSTRUAL HISTORY
Mnemonic: "PALM-COEIN" (for abnormal bleeding) + "DAMP"
Full Menstrual History Checklist
| Question | What to Establish |
|---|---|
| LMP (Last Menstrual Period) | Exact date (day 1 of last period) → calculate EDD if pregnant |
| Cycle length | Normal: 21–35 days; average 28 days |
| Duration of flow | Normal: 2–7 days |
| Amount | Normal: 20–80 mL per cycle; >80 mL = menorrhagia |
| Regularity | Regular / irregular |
| Intermenstrual bleeding (IMB) | Bleeding between periods |
| Post-coital bleeding (PCB) | Bleeding after sex → think cervical pathology (cervical cancer, polyp, ectropion) |
| Postmenopausal bleeding (PMB) | If >12 months since last period → endometrial cancer until proven otherwise |
| Dysmenorrhoea | Primary (no pathology) vs. secondary (endometriosis, PID, fibroids) |
| Premenstrual symptoms | Bloating, mood change, breast tenderness |
| Menarche | Age of first period (normal 10–16 years) |
| Menopause | Age at last period (normal ~51 years average) |
PALM-COEIN Classification (Abnormal Uterine Bleeding — AUB)
| Structural (PALM) | Non-structural (COEIN) |
|---|---|
| Polyp | Coagulopathy |
| Adenomyosis | Ovulatory dysfunction |
| Leiomyoma (fibroid) | Endometrial |
| Malignancy & hyperplasia | Iatrogenic |
| Not yet classified |
STEP 3 — SEXUAL HISTORY
| P | Question |
|---|---|
| Partners | How many partners? Male, female, or both? Current relationship? |
| Practices | Vaginal, oral, anal intercourse? |
| Protection | Contraception used? Consistent condom use? |
| Past STIs | Previous sexually transmitted infections? Treated? |
| Pregnancy | Any previous pregnancies? Desired fertility now? |
- Any pain during intercourse? (dyspareunia — superficial or deep)
- Any pain after intercourse?
- Libido changes?
- Any history of sexual coercion/assault (sensitively, if relevant)
STEP 4 — VAGINAL DISCHARGE HISTORY
| Letter | Question |
|---|---|
| Volume | How much? |
| Odour | Fishy (BV), offensive |
| Duration | How long? |
| Colour | White/grey (BV), yellow/green (Trichomonas/gonorrhoea), cottage-cheese white (Candida) |
| Associated symptoms | Itch (Candida), dysuria, dyspareunia, abdominal pain |
| Sexually associated | New partner? Unprotected sex? |
| Triggers | Antibiotics, immunosuppression, pregnancy |
Quick Reference — Discharge Types
| Condition | Colour | Odour | Itch | Other |
|---|---|---|---|---|
| Bacterial Vaginosis | Grey/white, thin | Fishy (worse after sex) | No | pH >4.5; clue cells |
| Candidiasis | White, thick "cottage cheese" | None | Yes (intense) | Vulval erythema |
| Trichomonas | Yellow-green, frothy | Offensive | Yes | Strawberry cervix |
| Gonorrhoea | Yellow, purulent | Variable | No | Cervicitis, dysuria |
| Chlamydia | Often none | None | No | Often asymptomatic |
STEP 5 — CONTRACEPTION HISTORY
- Current method and duration of use
- Previous methods and reasons for changing
- Compliance / missed pills?
- Complications (e.g., breakthrough bleeding on COCP)
- Desire for future pregnancy?
STEP 6 — CERVICAL SMEAR / SCREENING HISTORY
- Date of last cervical smear (Pap smear)
- Any abnormal smears? (CIN grade, treatment — LLETZ, cone biopsy)
- HPV vaccination status
STEP 7 — PELVIC PAIN HISTORY
| E | Possible Cause |
|---|---|
| Ectopic pregnancy | Unilateral sharp pain + amenorrhoea + PV bleeding |
| Endometriosis | Cyclical pain, deep dyspareunia, infertility |
| Endomyometritis / PID | Fever, discharge, bilateral lower abdominal pain |
| Enlarging fibroid | Pressure symptoms, menorrhagia |
| Enteric/GI cause | Constipation, IBS, appendicitis |
| Extra-pelvic | MSK, referred pain from spine |
PART B: OBSTETRIC HISTORY
STEP 1 — CURRENT PREGNANCY OVERVIEW
Mnemonic: "GPAL + DATE + ANC"
| Component | Details |
|---|---|
| Gravida | Total number of pregnancies (including current) |
| Para | Number of deliveries >20–24 weeks (viable) |
| Abortus | Losses <20–24 weeks (miscarriages + terminations) |
| Living children | Number of living children |
Example: G4 P2+1+1+2 = 4 pregnancies, 2 term deliveries, 1 preterm, 1 abortion, 2 living children
Calculating EDD — Naegele's Rule
EDD = LMP + 9 months + 7 days (or + 1 year - 3 months + 7 days) Valid for a 28-day cycle. Adjust +1 day for each day cycle is >28, -1 day for each day <28.
| Method | Details |
|---|---|
| LMP-based | Naegele's Rule (40 weeks from LMP) |
| Ultrasound | Most accurate if done <13 weeks (crown-rump length) |
| Fundal height | After 20 weeks: fundal height (cm) ≈ gestational age (weeks) ±2 cm |
STEP 2 — PRESENTING COMPLAINT IN CURRENT PREGNANCY
| Symptom | Think |
|---|---|
| Vaginal bleeding (any trimester) | Miscarriage, ectopic, placenta praevia, abruption |
| Severe headache | Pre-eclampsia |
| Visual disturbances (flashing lights, blurring) | Pre-eclampsia |
| Epigastric pain / RUQ pain | HELLP syndrome, liver capsule stretch |
| Reduced / absent fetal movements | Fetal distress, IUFD |
| Swelling (face, hands, legs) | Pre-eclampsia, DVT |
| Leaking fluid PV | Prelabour rupture of membranes (PROM) |
| Fever + rigors | Chorioamnionitis, UTI, malaria |
| Fits / convulsions | Eclampsia |
| Difficulty breathing | PE, cardiac disease |
STEP 3 — ANTENATAL HISTORY (Current Pregnancy)
Mnemonic: "ABCD-FIGS"
| Letter | Component |
|---|---|
| Attendance | ANC visits — how many? Where? Booking visit timing? |
| Book | Booking bloods: blood group, Rh status, FBC, HIV, syphilis, HBsAg, rubella |
| Complications | Any complications this pregnancy? |
| Drugs | Any medications this pregnancy? Folic acid taken? |
| Fetal | Fetal movements — when started (quickening ~18–20 wks primip; ~16–18 wks multip), current frequency |
| Immunisation | Tetanus toxoid, malaria prophylaxis |
| Growth scans | Any ultrasound scans done? Reports? |
| Symptoms | Morning sickness, heartburn, urinary symptoms, constipation |
STEP 4 — PREVIOUS OBSTETRIC HISTORY
| Question | Details |
|---|---|
| Year and outcome | Live birth / stillbirth / miscarriage / TOP |
| Gestational age at delivery | Term / preterm / post-term |
| Mode of delivery | SVD / instrumental (forceps/ventouse) / LSCS |
| Reason for CS | Previous CS type (classical vs. lower segment) |
| Birth weight | Small / large for dates |
| Complications in labour | PPH, prolonged labour, shoulder dystocia |
| Neonatal outcome | SCBU admission? APGAR scores? Congenital abnormalities? |
| Postnatal complications | Infection, wound breakdown, puerperal psychosis |
Key Red Flags in Previous Obstetric History
- Previous CS → risk of uterine rupture in subsequent labour; discuss VBAC vs. repeat CS
- Previous PPH → increased risk of recurrence; alert team
- Pre-eclampsia → 20% recurrence risk
- Gestational diabetes → 50% recurrence risk; screen early
- Preterm birth → screen for cervical length; consider cervical cerclage
STEP 5 — GYNAECOLOGICAL HISTORY (within OBS context)
- Fibroids (can obstruct labour)
- Ovarian cysts in pregnancy
- Previous pelvic surgery / cervical surgery (LLETZ → risk of preterm birth)
- STIs
- Infertility treatment (IVF → higher risk multiple pregnancy)
PART C: SHARED HISTORY SECTIONS (Both OBS & GYNAE)
STEP 6 — PAST MEDICAL HISTORY (PMH)
Mnemonic: "MJ THREADS"
| Letter | Condition |
|---|---|
| MI / cardiac | Cardiac disease in pregnancy = high risk |
| Jaundice / liver | Obstetric cholestasis, hepatitis |
| Thyroid | Hypo/hyperthyroidism |
| Hypertension | Pre-existing vs. gestational |
| Rheumatological | SLE → pregnancy complications |
| Epilepsy | AEDs affect folic acid; seizure risk |
| Anaemia / haematological | Sickle cell, thalassaemia |
| Diabetes mellitus | Pre-existing vs. gestational |
| Surgeries (previous) | Abdominal scars, uterine surgery |
STEP 7 — DRUG HISTORY
- Current medications (prescribed, OTC, herbal)
- Folic acid — 400 mcg/day (start pre-conception, continue to 12 weeks); 5 mg/day if high risk (epilepsy, previous NTD, diabetes, BMI >30)
- Teratogenic drugs to specifically ask about: methotrexate, warfarin, valproate, retinoids, ACE inhibitors, lithium
- Allergies — drug name AND type of reaction
STEP 8 — FAMILY HISTORY
| Condition | Why Important |
|---|---|
| Hypertension / pre-eclampsia | Increased risk |
| Diabetes | Gestational diabetes risk |
| Multiple gestation | Familial dizygotic twins |
| Breast/ovarian cancer | BRCA1/2 relevance |
| Congenital abnormalities | Genetic counselling |
| Thromboembolic disease | Inherited thrombophilia (Factor V Leiden) |
| Genetic conditions | Down syndrome, CF, sickle cell |
STEP 9 — SOCIAL HISTORY
Mnemonic: "HEADS-SS" (adapted from adolescent HEADS)
| Letter | Component |
|---|---|
| Home | Living situation, housing, support at home, domestic violence |
| Education/Employment | Occupation, maternity leave planning |
| Alcohol | Units per week; timing in pregnancy (any = risk) |
| Drugs | Recreational drug use (cannabis, cocaine, heroin → FGR, NAS) |
| Smoking | Cigarettes/day; passive smoking |
| Support | Social support, partner involvement, financial situation |
| Stress/mental health | Depression (Edinburgh scale in antenatal), anxiety, previous psychiatric history |
STEP 10 — SYSTEMS REVIEW (RELEVANT)
| System | Key Questions |
|---|---|
| Urinary | Dysuria, frequency, haematuria (UTI, renal stones) |
| Bowel | Constipation, rectal bleeding, change in habit |
| Cardiovascular | Palpitations, chest pain, SOB, ankle oedema |
| Respiratory | Cough, wheeze, SOB |
| Neurological | Headache, visual disturbance, fits |
| Musculoskeletal | Pelvic girdle pain (PGP), lower back pain |
QUICK REFERENCE SUMMARY CARD
Gynaecology History — "MSPDC"
| Letter | Domain |
|---|---|
| Menstrual history | LMP, cycle, flow, dysmenorrhoea, PMB, IMB, PCB |
| Sexual & STI | Partners, practices, protection, STIs, dyspareunia |
| Pain | SOCRATES; 6 E's for pelvic pain |
| Discharge | VODCAST |
| Contraception & Cervical smear | Current method, last smear, HPV |
Obstetric History — "GPAL + DATE + ANC + Previous"
| Component | Key Points |
|---|---|
| GPAL | Gravida, Para, Abortus, Living |
| DATE | LMP → EDD (Naegele); USS dating |
| ANC | Booking bloods, scans, complications, fetal movements |
| Previous pregnancies | Mode, outcome, complications (each one) |
Shared Sections — "PDFS"
| Letter | Section |
|---|---|
| Past medical & surgical history | MJ THREADS |
| Drugs & Allergies | Teratogens, folic acid |
| Family history | Pre-eclampsia, diabetes, genetic conditions |
| Social history | HEADS-SS |
DANGER SIGNS IN PREGNANCY — "HAVE SELF"
| Letter | Sign |
|---|---|
| Headache (severe) | Pre-eclampsia |
| Abdominal pain (epigastric/RUQ) | HELLP |
| Vaginal bleeding | Placenta praevia/abruption/ectopic |
| Edema (sudden, face/hands) | Pre-eclampsia |
| Seeing things (visual disturbance) | Pre-eclampsia |
| Eclamptic fits | Eclampsia |
| Liquor (leaking PV) | PROM |
| Fetal movements reduced | Fetal compromise |
Obs/ gynae history taking sheet simple made separately detailed
Obs history taking sheet code smart memory aid detailed
ls -la /home/daytona/workspace/ 2>/dev/null || echo "workspace empty or not found"
mkdir -p /home/daytona/workspace/obs-history
~/obs-history/obs_history_sheet.html
<!DOCTYPE html>
<html lang="en">
<head>
<meta charset="UTF-8">
<meta name="viewport" content="width=device-width, initial-scale=1.0">
<title>Obstetric History Taking — Smart Memory Aid</title>
<style>
@import url('https://fonts.googleapis.com/css2?family=Inter:wght@300;400;500;600;700;800&display=swap');
* { box-sizing: border-box; margin: 0; padding: 0; }
body {
font-family: 'Inter', Arial, sans-serif;
background: #f0f4f8;
color: #1a202c;
font-size: 13px;
line-height: 1.5;
}
.page {
max-width: 1100px;
margin: 0 auto;
padding: 20px;
}
/* ── HEADER ── */
.header {
background: linear-gradient(135deg, #1a365d 0%, #2b6cb0 60%, #4299e1 100%);
color: white;
border-radius: 14px;
padding: 22px 28px 18px;
margin-bottom: 18px;
display: flex;
align-items: center;
justify-content: space-between;
box-shadow: 0 4px 20px rgba(43,108,176,0.3);
}
.header-left h1 {
font-size: 22px;
font-weight: 800;
letter-spacing: -0.5px;
}
.header-left p {
font-size: 12px;
opacity: 0.85;
margin-top: 3px;
}
.header-badge {
background: rgba(255,255,255,0.18);
border: 1.5px solid rgba(255,255,255,0.4);
border-radius: 8px;
padding: 8px 14px;
text-align: center;
font-size: 11px;
}
.header-badge strong { font-size: 16px; display: block; }
/* ── MASTER MNEMONIC BANNER ── */
.master-banner {
background: linear-gradient(135deg, #744210, #c05621);
color: white;
border-radius: 10px;
padding: 12px 20px;
margin-bottom: 18px;
display: flex;
align-items: center;
gap: 14px;
box-shadow: 0 3px 12px rgba(192,86,33,0.3);
}
.master-banner .label {
font-size: 10px;
font-weight: 700;
letter-spacing: 1px;
text-transform: uppercase;
opacity: 0.85;
white-space: nowrap;
}
.master-banner .mnemonic {
font-size: 14px;
font-weight: 700;
letter-spacing: 0.5px;
}
.master-banner .mnemonic span {
background: rgba(255,255,255,0.2);
border-radius: 4px;
padding: 1px 6px;
margin: 0 2px;
font-size: 15px;
}
/* ── GRID LAYOUT ── */
.grid-2 { display: grid; grid-template-columns: 1fr 1fr; gap: 14px; margin-bottom: 14px; }
.grid-3 { display: grid; grid-template-columns: 1fr 1fr 1fr; gap: 14px; margin-bottom: 14px; }
.grid-1 { margin-bottom: 14px; }
.span-2 { grid-column: span 2; }
.span-3 { grid-column: span 3; }
/* ── CARDS ── */
.card {
background: white;
border-radius: 10px;
overflow: hidden;
box-shadow: 0 2px 8px rgba(0,0,0,0.07);
border: 1px solid #e2e8f0;
}
.card-header {
padding: 9px 14px;
display: flex;
align-items: center;
gap: 8px;
}
.card-header .icon {
width: 26px;
height: 26px;
border-radius: 6px;
background: rgba(255,255,255,0.25);
display: flex;
align-items: center;
justify-content: center;
font-size: 13px;
flex-shrink: 0;
}
.card-header .title {
font-size: 12px;
font-weight: 700;
text-transform: uppercase;
letter-spacing: 0.5px;
color: white;
}
.card-header .subtitle {
font-size: 10px;
color: rgba(255,255,255,0.8);
margin-left: auto;
font-style: italic;
}
/* Color themes */
.blue .card-header { background: linear-gradient(135deg, #2b6cb0, #4299e1); }
.teal .card-header { background: linear-gradient(135deg, #285e61, #38b2ac); }
.purple .card-header { background: linear-gradient(135deg, #553c9a, #805ad5); }
.green .card-header { background: linear-gradient(135deg, #276749, #48bb78); }
.red .card-header { background: linear-gradient(135deg, #9b2335, #e53e3e); }
.orange .card-header { background: linear-gradient(135deg, #7b341e, #ed8936); }
.pink .card-header { background: linear-gradient(135deg, #702459, #ed64a6); }
.navy .card-header { background: linear-gradient(135deg, #1a365d, #4a5568); }
.brown .card-header { background: linear-gradient(135deg, #744210, #d69e2e); }
.card-body { padding: 12px 14px; }
/* ── PATIENT INFO ROW ── */
.info-row {
display: flex;
gap: 10px;
flex-wrap: wrap;
margin-bottom: 6px;
}
.info-field {
flex: 1;
min-width: 120px;
}
.info-field label {
font-size: 9px;
font-weight: 700;
text-transform: uppercase;
letter-spacing: 0.5px;
color: #718096;
display: block;
margin-bottom: 2px;
}
.info-field .line {
border-bottom: 1.5px solid #cbd5e0;
height: 22px;
}
/* ── SECTION HEADING ── */
.sec-heading {
font-size: 10px;
font-weight: 700;
text-transform: uppercase;
letter-spacing: 0.8px;
color: #4a5568;
border-bottom: 1.5px solid #e2e8f0;
padding-bottom: 3px;
margin-bottom: 8px;
margin-top: 10px;
}
.sec-heading:first-child { margin-top: 0; }
/* ── ITEMS ── */
.item {
display: flex;
align-items: flex-start;
gap: 7px;
margin-bottom: 6px;
}
.item-dot {
width: 6px;
height: 6px;
border-radius: 50%;
margin-top: 5px;
flex-shrink: 0;
}
.item-label {
font-weight: 600;
font-size: 12px;
min-width: 100px;
flex-shrink: 0;
}
.item-line {
flex: 1;
border-bottom: 1px solid #e2e8f0;
height: 18px;
}
/* ── WRITE LINES ── */
.write-lines .wl {
border-bottom: 1px solid #e2e8f0;
height: 22px;
margin-bottom: 4px;
}
/* ── MNEMONIC BOXES ── */
.mbox {
display: flex;
flex-wrap: wrap;
gap: 5px;
margin: 8px 0;
}
.mbox-item {
border-radius: 6px;
padding: 5px 8px;
font-size: 11px;
text-align: center;
min-width: 70px;
flex: 1;
}
.mbox-item .letter {
font-size: 18px;
font-weight: 800;
line-height: 1;
display: block;
}
.mbox-item .word {
font-size: 9px;
font-weight: 600;
display: block;
text-transform: uppercase;
letter-spacing: 0.3px;
opacity: 0.85;
margin-top: 1px;
}
/* ── TABLE ── */
.mini-table {
width: 100%;
border-collapse: collapse;
font-size: 11px;
margin: 6px 0;
}
.mini-table th {
background: #edf2f7;
padding: 5px 8px;
text-align: left;
font-weight: 700;
font-size: 10px;
text-transform: uppercase;
letter-spacing: 0.3px;
color: #4a5568;
border: 1px solid #e2e8f0;
}
.mini-table td {
padding: 5px 8px;
border: 1px solid #e2e8f0;
vertical-align: top;
}
.mini-table tr:nth-child(even) td { background: #f7fafc; }
/* ── CHECKBOX LIST ── */
.chk-list {
display: grid;
grid-template-columns: 1fr 1fr;
gap: 4px;
font-size: 11px;
}
.chk-list.cols-3 { grid-template-columns: 1fr 1fr 1fr; }
.chk-item {
display: flex;
align-items: center;
gap: 5px;
}
.chk-box {
width: 13px;
height: 13px;
border: 1.5px solid #a0aec0;
border-radius: 3px;
flex-shrink: 0;
}
/* ── DANGER SIGNS ── */
.danger-grid {
display: grid;
grid-template-columns: repeat(4, 1fr);
gap: 5px;
margin: 6px 0;
}
.danger-item {
background: #fff5f5;
border: 1.5px solid #feb2b2;
border-radius: 7px;
padding: 6px 8px;
text-align: center;
font-size: 10px;
}
.danger-item .d-letter {
font-size: 20px;
font-weight: 800;
color: #c53030;
line-height: 1;
}
.danger-item .d-word {
font-weight: 700;
color: #c53030;
font-size: 9px;
display: block;
margin: 1px 0;
}
.danger-item .d-desc {
color: #742a2a;
font-size: 9px;
line-height: 1.3;
}
/* ── GPAL BOX ── */
.gpal-row {
display: grid;
grid-template-columns: repeat(4, 1fr);
gap: 8px;
margin: 8px 0;
}
.gpal-box {
background: #ebf8ff;
border: 2px solid #bee3f8;
border-radius: 8px;
padding: 8px;
text-align: center;
}
.gpal-box .g-letter {
font-size: 22px;
font-weight: 800;
color: #2b6cb0;
line-height: 1;
}
.gpal-box .g-word {
font-size: 9px;
font-weight: 700;
color: #2c5282;
text-transform: uppercase;
display: block;
margin: 2px 0;
}
.gpal-box .g-line {
border-bottom: 1.5px solid #90cdf4;
height: 22px;
margin-top: 4px;
}
/* ── TRIMESTER TAG ── */
.tri-row {
display: flex;
gap: 8px;
margin: 6px 0;
}
.tri-item {
flex: 1;
border-radius: 7px;
padding: 7px 10px;
font-size: 11px;
}
.tri-item .t-title {
font-weight: 700;
font-size: 10px;
text-transform: uppercase;
margin-bottom: 4px;
}
.tri-item.t1 { background: #e6fffa; border: 1.5px solid #81e6d9; }
.tri-item.t1 .t-title { color: #234e52; }
.tri-item.t2 { background: #ebf8ff; border: 1.5px solid #90cdf4; }
.tri-item.t2 .t-title { color: #1a365d; }
.tri-item.t3 { background: #fff5f5; border: 1.5px solid #feb2b2; }
.tri-item.t3 .t-title { color: #742a2a; }
/* ── PREVIOUS PREG TABLE ── */
.prev-preg-table {
width: 100%;
border-collapse: collapse;
font-size: 10.5px;
}
.prev-preg-table th {
background: #4a5568;
color: white;
padding: 5px 6px;
text-align: center;
font-size: 9.5px;
font-weight: 700;
text-transform: uppercase;
letter-spacing: 0.3px;
border: 1px solid #2d3748;
}
.prev-preg-table td {
padding: 5px 6px;
border: 1px solid #e2e8f0;
text-align: center;
height: 24px;
background: white;
}
.prev-preg-table tr:nth-child(even) td { background: #f7fafc; }
/* ── EDD CALCULATOR BOX ── */
.edd-box {
background: linear-gradient(135deg, #f0fff4, #c6f6d5);
border: 2px solid #68d391;
border-radius: 10px;
padding: 10px 14px;
margin: 8px 0;
}
.edd-box .edd-title {
font-size: 11px;
font-weight: 700;
color: #276749;
margin-bottom: 8px;
text-transform: uppercase;
letter-spacing: 0.5px;
}
.edd-row {
display: flex;
align-items: center;
gap: 8px;
font-size: 12px;
margin-bottom: 5px;
}
.edd-label {
font-weight: 600;
min-width: 50px;
color: #2d6a4f;
font-size: 11px;
}
.edd-line {
flex: 1;
border-bottom: 1.5px solid #48bb78;
height: 20px;
}
.edd-formula {
font-size: 11px;
color: #276749;
background: rgba(255,255,255,0.6);
border-radius: 5px;
padding: 4px 8px;
margin-top: 5px;
font-style: italic;
}
/* ── BADGE ── */
.badge {
display: inline-block;
padding: 1px 6px;
border-radius: 4px;
font-size: 9px;
font-weight: 700;
text-transform: uppercase;
letter-spacing: 0.3px;
}
.badge-red { background: #fed7d7; color: #c53030; }
.badge-blue { background: #bee3f8; color: #2c5282; }
.badge-green { background: #c6f6d5; color: #276749; }
.badge-orange { background: #feebc8; color: #744210; }
.badge-purple { background: #e9d8fd; color: #553c9a; }
/* ── NOTES AREA ── */
.notes-area {
border: 1.5px dashed #cbd5e0;
border-radius: 8px;
padding: 8px 10px;
margin-top: 6px;
min-height: 50px;
}
.notes-area .note-line {
border-bottom: 1px solid #edf2f7;
height: 20px;
margin-bottom: 2px;
}
/* ── FOOTER ── */
.footer {
text-align: center;
font-size: 10px;
color: #718096;
padding: 14px 0 6px;
border-top: 1px solid #e2e8f0;
margin-top: 18px;
}
/* ── PRINT ── */
@media print {
body { background: white; font-size: 11px; }
.page { padding: 10px; max-width: 100%; }
.card { box-shadow: none; border: 1px solid #cbd5e0; break-inside: avoid; }
.grid-2, .grid-3 { gap: 10px; }
.header { background: #1a365d !important; -webkit-print-color-adjust: exact; print-color-adjust: exact; }
}
.print-btn {
position: fixed;
top: 16px;
right: 16px;
background: linear-gradient(135deg, #2b6cb0, #4299e1);
color: white;
border: none;
padding: 10px 18px;
border-radius: 8px;
font-size: 13px;
font-weight: 600;
cursor: pointer;
box-shadow: 0 3px 12px rgba(43,108,176,0.4);
z-index: 999;
}
.print-btn:hover { background: linear-gradient(135deg, #1a365d, #2b6cb0); }
@media print { .print-btn { display: none; } }
</style>
</head>
<body>
<button class="print-btn" onclick="window.print()">🖨️ Print / Save PDF</button>
<div class="page">
<!-- ══════════ HEADER ══════════ -->
<div class="header">
<div class="header-left">
<h1>🤰 Obstetric History Taking</h1>
<p>Comprehensive Smart Memory Aid | Obs & Gynae Clinical Sheet</p>
</div>
<div class="header-badge">
<strong>OBS-HX</strong>
Smart Aid v1.0
</div>
</div>
<!-- ══════════ MASTER MNEMONIC ══════════ -->
<div class="master-banner">
<div class="label">Master<br>Framework</div>
<div class="mnemonic">
<span>G</span>PAL →
<span>L</span>MP/EDD →
<span>A</span>NC →
<span>P</span>revious Preg →
<span>M</span>edical Hx →
<span>D</span>rugs →
<span>F</span>amily →
<span>S</span>ocial
</div>
</div>
<!-- ══════════ ROW 1: Patient Info + GPAL ══════════ -->
<div class="grid-2">
<!-- Patient Info -->
<div class="card blue">
<div class="card-header">
<div class="icon">👤</div>
<div class="title">Patient Information</div>
</div>
<div class="card-body">
<div class="info-row">
<div class="info-field"><label>Full Name</label><div class="line"></div></div>
<div class="info-field"><label>Age</label><div class="line"></div></div>
<div class="info-field"><label>Date</label><div class="line"></div></div>
</div>
<div class="info-row">
<div class="info-field"><label>Hospital No.</label><div class="line"></div></div>
<div class="info-field"><label>Ward / Clinic</label><div class="line"></div></div>
<div class="info-field"><label>Clinician</label><div class="line"></div></div>
</div>
<div class="info-row">
<div class="info-field"><label>Occupation</label><div class="line"></div></div>
<div class="info-field"><label>Marital Status</label><div class="line"></div></div>
<div class="info-field"><label>Religion / Ethnicity</label><div class="line"></div></div>
</div>
<div class="sec-heading">Chief Complaint</div>
<div class="write-lines">
<div class="wl"></div><div class="wl"></div>
</div>
</div>
</div>
<!-- GPAL Status -->
<div class="card teal">
<div class="card-header">
<div class="icon">🔢</div>
<div class="title">GPAL Obstetric Status</div>
<div class="subtitle">Fill in the boxes</div>
</div>
<div class="card-body">
<div class="gpal-row">
<div class="gpal-box">
<div class="g-letter">G</div>
<div class="g-word">Gravida</div>
<div style="font-size:9px;color:#4a5568;margin:2px 0;">Total pregnancies<br>(incl. current)</div>
<div class="g-line"></div>
</div>
<div class="gpal-box">
<div class="g-letter">P</div>
<div class="g-word">Para</div>
<div style="font-size:9px;color:#4a5568;margin:2px 0;">Deliveries<br>≥20 wks (viable)</div>
<div class="g-line"></div>
</div>
<div class="gpal-box">
<div class="g-letter">A</div>
<div class="g-word">Abortus</div>
<div style="font-size:9px;color:#4a5568;margin:2px 0;">Losses<br><20 wks</div>
<div class="g-line"></div>
</div>
<div class="gpal-box">
<div class="g-letter">L</div>
<div class="g-word">Living</div>
<div style="font-size:9px;color:#4a5568;margin:2px 0;">Living<br>children</div>
<div class="g-line"></div>
</div>
</div>
<div style="background:#f0fff4;border-radius:6px;padding:6px 10px;font-size:10px;color:#276749;border:1px solid #c6f6d5;">
<strong>Example:</strong> G3 P2+0+1+2 = 3 pregnancies, 2 term deliveries, 0 preterm, 1 miscarriage, 2 living children
</div>
</div>
</div>
</div>
<!-- ══════════ ROW 2: EDD + Presenting Complaint ══════════ -->
<div class="grid-2">
<!-- LMP + EDD -->
<div class="card green">
<div class="card-header">
<div class="icon">📅</div>
<div class="title">LMP, EDD & Gestational Age</div>
</div>
<div class="card-body">
<div class="edd-box">
<div class="edd-title">📐 Naegele's Rule</div>
<div class="edd-row">
<div class="edd-label">LMP:</div>
<div class="edd-line"></div>
</div>
<div class="edd-row">
<div class="edd-label">EDD:</div>
<div class="edd-line"></div>
</div>
<div class="edd-row">
<div class="edd-label">GA Today:</div>
<div class="edd-line"></div>
</div>
<div class="edd-formula">LMP + 9 months + 7 days = EDD | Adjust for cycle ≠ 28 days</div>
</div>
<div class="sec-heading">Cycle Details</div>
<div class="item">
<div class="item-dot" style="background:#48bb78;"></div>
<div class="item-label">Cycle Length:</div>
<div class="item-line"></div>
</div>
<div class="item">
<div class="item-dot" style="background:#48bb78;"></div>
<div class="item-label">Regular/Irregular:</div>
<div class="item-line"></div>
</div>
<div class="item">
<div class="item-dot" style="background:#48bb78;"></div>
<div class="item-label">USS Dating Scan:</div>
<div class="item-line"></div>
</div>
<div class="item">
<div class="item-dot" style="background:#48bb78;"></div>
<div class="item-label">CRL (at <13wks):</div>
<div class="item-line"></div>
</div>
</div>
</div>
<!-- Presenting Complaint -->
<div class="card red">
<div class="card-header">
<div class="icon">🚨</div>
<div class="title">Presenting Complaint — SOCRATES</div>
</div>
<div class="card-body">
<div class="mbox">
<div class="mbox-item" style="background:#fff5f5;border:1.5px solid #feb2b2;">
<span class="letter" style="color:#c53030;">S</span>
<span class="word" style="color:#742a2a;">Site</span>
</div>
<div class="mbox-item" style="background:#fff5f5;border:1.5px solid #feb2b2;">
<span class="letter" style="color:#c53030;">O</span>
<span class="word" style="color:#742a2a;">Onset</span>
</div>
<div class="mbox-item" style="background:#fff5f5;border:1.5px solid #feb2b2;">
<span class="letter" style="color:#c53030;">C</span>
<span class="word" style="color:#742a2a;">Character</span>
</div>
<div class="mbox-item" style="background:#fff5f5;border:1.5px solid #feb2b2;">
<span class="letter" style="color:#c53030;">R</span>
<span class="word" style="color:#742a2a;">Radiation</span>
</div>
<div class="mbox-item" style="background:#fff5f5;border:1.5px solid #feb2b2;">
<span class="letter" style="color:#c53030;">A</span>
<span class="word" style="color:#742a2a;">Assoc. Sx</span>
</div>
<div class="mbox-item" style="background:#fff5f5;border:1.5px solid #feb2b2;">
<span class="letter" style="color:#c53030;">T</span>
<span class="word" style="color:#742a2a;">Timing</span>
</div>
<div class="mbox-item" style="background:#fff5f5;border:1.5px solid #feb2b2;">
<span class="letter" style="color:#c53030;">E</span>
<span class="word" style="color:#742a2a;">Exac/Reliev</span>
</div>
<div class="mbox-item" style="background:#fff5f5;border:1.5px solid #feb2b2;">
<span class="letter" style="color:#c53030;">S</span>
<span class="word" style="color:#742a2a;">Severity</span>
</div>
</div>
<div class="write-lines">
<div class="wl"></div><div class="wl"></div><div class="wl"></div>
<div class="wl"></div><div class="wl"></div>
</div>
</div>
</div>
</div>
<!-- ══════════ ROW 3: ANC History ══════════ -->
<div class="grid-1">
<div class="card purple">
<div class="card-header">
<div class="icon">🏥</div>
<div class="title">Antenatal Care (ANC) History — Current Pregnancy</div>
<div class="subtitle">Mnemonic: ABCD-FIGS</div>
</div>
<div class="card-body">
<div class="mbox" style="margin-bottom:10px;">
<div class="mbox-item" style="background:#faf5ff;border:1.5px solid #d6bcfa;">
<span class="letter" style="color:#553c9a;">A</span>
<span class="word" style="color:#44337a;">Attendance</span>
</div>
<div class="mbox-item" style="background:#faf5ff;border:1.5px solid #d6bcfa;">
<span class="letter" style="color:#553c9a;">B</span>
<span class="word" style="color:#44337a;">Booking</span>
</div>
<div class="mbox-item" style="background:#faf5ff;border:1.5px solid #d6bcfa;">
<span class="letter" style="color:#553c9a;">C</span>
<span class="word" style="color:#44337a;">Complications</span>
</div>
<div class="mbox-item" style="background:#faf5ff;border:1.5px solid #d6bcfa;">
<span class="letter" style="color:#553c9a;">D</span>
<span class="word" style="color:#44337a;">Drugs/Folic</span>
</div>
<div class="mbox-item" style="background:#faf5ff;border:1.5px solid #d6bcfa;">
<span class="letter" style="color:#553c9a;">F</span>
<span class="word" style="color:#44337a;">Fetal Mvmts</span>
</div>
<div class="mbox-item" style="background:#faf5ff;border:1.5px solid #d6bcfa;">
<span class="letter" style="color:#553c9a;">I</span>
<span class="word" style="color:#44337a;">Immunisation</span>
</div>
<div class="mbox-item" style="background:#faf5ff;border:1.5px solid #d6bcfa;">
<span class="letter" style="color:#553c9a;">G</span>
<span class="word" style="color:#44337a;">Growth Scans</span>
</div>
<div class="mbox-item" style="background:#faf5ff;border:1.5px solid #d6bcfa;">
<span class="letter" style="color:#553c9a;">S</span>
<span class="word" style="color:#44337a;">Symptoms</span>
</div>
</div>
<div class="grid-3">
<div>
<div class="sec-heading">📋 Attendance & Booking</div>
<div class="item"><div class="item-dot" style="background:#805ad5;"></div><div class="item-label">No. of ANC visits:</div><div class="item-line"></div></div>
<div class="item"><div class="item-dot" style="background:#805ad5;"></div><div class="item-label">Booking visit GA:</div><div class="item-line"></div></div>
<div class="item"><div class="item-dot" style="background:#805ad5;"></div><div class="item-label">Booking facility:</div><div class="item-line"></div></div>
<div class="sec-heading">🩸 Booking Bloods</div>
<div class="chk-list">
<div class="chk-item"><div class="chk-box"></div> Blood group</div>
<div class="chk-item"><div class="chk-box"></div> Rh status</div>
<div class="chk-item"><div class="chk-box"></div> FBC / Hb</div>
<div class="chk-item"><div class="chk-box"></div> HIV</div>
<div class="chk-item"><div class="chk-box"></div> VDRL/Syphilis</div>
<div class="chk-item"><div class="chk-box"></div> HBsAg</div>
<div class="chk-item"><div class="chk-box"></div> Rubella IgG</div>
<div class="chk-item"><div class="chk-box"></div> MSU/UA</div>
</div>
<div style="margin-top:6px;">
<div class="item"><div class="item-dot" style="background:#805ad5;"></div><div class="item-label">Blood Group:</div><div class="item-line"></div></div>
<div class="item"><div class="item-dot" style="background:#805ad5;"></div><div class="item-label">Hb (g/dL):</div><div class="item-line"></div></div>
<div class="item"><div class="item-dot" style="background:#805ad5;"></div><div class="item-label">HIV status:</div><div class="item-line"></div></div>
</div>
</div>
<div>
<div class="sec-heading">🔬 Ultrasound Scans</div>
<table class="mini-table">
<tr><th>Scan</th><th>GA</th><th>Findings</th></tr>
<tr><td>Dating (<13wk)</td><td></td><td></td></tr>
<tr><td>Anomaly (18–20wk)</td><td></td><td></td></tr>
<tr><td>Growth scan</td><td></td><td></td></tr>
<tr><td>Placenta site</td><td></td><td></td></tr>
<tr><td>AFI / liquor</td><td></td><td></td></tr>
</table>
<div class="sec-heading" style="margin-top:8px;">💉 Immunisations</div>
<div class="chk-list">
<div class="chk-item"><div class="chk-box"></div> Tetanus Toxoid 1</div>
<div class="chk-item"><div class="chk-box"></div> Tetanus Toxoid 2</div>
<div class="chk-item"><div class="chk-box"></div> Hep B vaccine</div>
<div class="chk-item"><div class="chk-box"></div> IPT (malaria)</div>
</div>
</div>
<div>
<div class="sec-heading">💊 Drugs & Supplements</div>
<div class="chk-list">
<div class="chk-item"><div class="chk-box"></div> Folic acid</div>
<div class="chk-item"><div class="chk-box"></div> Iron supplement</div>
<div class="chk-item"><div class="chk-box"></div> Calcium</div>
<div class="chk-item"><div class="chk-box"></div> Aspirin</div>
<div class="chk-item"><div class="chk-box"></div> Haematinics</div>
<div class="chk-item"><div class="chk-box"></div> HAART (if HIV+)</div>
</div>
<div class="item" style="margin-top:6px;"><div class="item-dot" style="background:#805ad5;"></div><div class="item-label">Other meds:</div><div class="item-line"></div></div>
<div class="sec-heading">👶 Fetal Movements</div>
<div class="item"><div class="item-dot" style="background:#805ad5;"></div><div class="item-label">Quickening at:</div><div class="item-line"></div></div>
<div class="item"><div class="item-dot" style="background:#805ad5;"></div><div class="item-label">Currently:</div><div class="item-line"></div></div>
<div style="font-size:10px;color:#553c9a;margin-top:3px;padding:4px 6px;background:#faf5ff;border-radius:5px;">
Normal: ≥10 movements in 12 hrs<br>
Primip quickening: ~18–20 wks<br>
Multip quickening: ~16–18 wks
</div>
</div>
</div>
<!-- Trimester Complications -->
<div class="sec-heading">⚠️ Complications by Trimester</div>
<div class="tri-row">
<div class="tri-item t1">
<div class="t-title">1st Trimester (<14 wks)</div>
<div class="chk-list">
<div class="chk-item"><div class="chk-box"></div> Hyperemesis gravidarum</div>
<div class="chk-item"><div class="chk-box"></div> Threatened miscarriage</div>
<div class="chk-item"><div class="chk-box"></div> Ectopic concern</div>
<div class="chk-item"><div class="chk-box"></div> UTI</div>
</div>
</div>
<div class="tri-item t2">
<div class="t-title">2nd Trimester (14–28 wks)</div>
<div class="chk-list">
<div class="chk-item"><div class="chk-box"></div> Anaemia</div>
<div class="chk-item"><div class="chk-box"></div> GDM screening</div>
<div class="chk-item"><div class="chk-box"></div> Cervical incompetence</div>
<div class="chk-item"><div class="chk-box"></div> Placenta praevia</div>
</div>
</div>
<div class="tri-item t3">
<div class="t-title">3rd Trimester (28+ wks)</div>
<div class="chk-list">
<div class="chk-item"><div class="chk-box"></div> Pre-eclampsia / HTN</div>
<div class="chk-item"><div class="chk-box"></div> GDM / raised BSL</div>
<div class="chk-item"><div class="chk-box"></div> APH / abruption</div>
<div class="chk-item"><div class="chk-box"></div> PROM / preterm labour</div>
</div>
</div>
</div>
</div>
</div>
</div>
<!-- ══════════ ROW 4: Danger Signs ══════════ -->
<div class="grid-1">
<div class="card red">
<div class="card-header">
<div class="icon">🚨</div>
<div class="title">DANGER SIGNS in Pregnancy — "HAVE SELF"</div>
<div class="subtitle">Any ✓ = urgent escalation</div>
</div>
<div class="card-body">
<div class="danger-grid">
<div class="danger-item">
<div class="d-letter">H</div>
<span class="d-word">Headache</span>
<div class="d-desc">Severe, persistent<br>→ Pre-eclampsia</div>
<div style="margin-top:4px;"><div class="chk-box" style="margin:0 auto;"></div></div>
</div>
<div class="danger-item">
<div class="d-letter">A</div>
<span class="d-word">Abdominal Pain</span>
<div class="d-desc">Epigastric / RUQ<br>→ HELLP</div>
<div style="margin-top:4px;"><div class="chk-box" style="margin:0 auto;"></div></div>
</div>
<div class="danger-item">
<div class="d-letter">V</div>
<span class="d-word">Vaginal Bleeding</span>
<div class="d-desc">Any trimester<br>→ Praevia/Abruption</div>
<div style="margin-top:4px;"><div class="chk-box" style="margin:0 auto;"></div></div>
</div>
<div class="danger-item">
<div class="d-letter">E</div>
<span class="d-word">Edema</span>
<div class="d-desc">Face/hands/legs<br>→ Pre-eclampsia</div>
<div style="margin-top:4px;"><div class="chk-box" style="margin:0 auto;"></div></div>
</div>
<div class="danger-item">
<div class="d-letter">S</div>
<span class="d-word">Seeing Blurs</span>
<div class="d-desc">Visual disturbance<br>→ Pre-eclampsia</div>
<div style="margin-top:4px;"><div class="chk-box" style="margin:0 auto;"></div></div>
</div>
<div class="danger-item">
<div class="d-letter">E</div>
<span class="d-word">Eclamptic Fits</span>
<div class="d-desc">Convulsions<br>→ Eclampsia</div>
<div style="margin-top:4px;"><div class="chk-box" style="margin:0 auto;"></div></div>
</div>
<div class="danger-item">
<div class="d-letter">L</div>
<span class="d-word">Liquor Leaking</span>
<div class="d-desc">PV fluid loss<br>→ PROM</div>
<div style="margin-top:4px;"><div class="chk-box" style="margin:0 auto;"></div></div>
</div>
<div class="danger-item">
<div class="d-letter">F</div>
<span class="d-word">Fetal Mvmts ↓</span>
<div class="d-desc">Reduced/absent<br>→ Fetal distress</div>
<div style="margin-top:4px;"><div class="chk-box" style="margin:0 auto;"></div></div>
</div>
</div>
</div>
</div>
</div>
<!-- ══════════ ROW 5: Previous Pregnancies ══════════ -->
<div class="grid-1">
<div class="card navy">
<div class="card-header">
<div class="icon">📚</div>
<div class="title">Previous Obstetric History — Detail Each Pregnancy</div>
<div class="subtitle">Start with oldest → most recent</div>
</div>
<div class="card-body">
<div style="overflow-x:auto;">
<table class="prev-preg-table">
<thead>
<tr>
<th style="width:30px;">#</th>
<th>Year</th>
<th>GA at delivery</th>
<th>Mode of delivery</th>
<th>Sex</th>
<th>Birth Wt</th>
<th>Outcome<br>(Live/Still/NND)</th>
<th>Complications<br>(mother)</th>
<th>Complications<br>(baby/SCBU)</th>
<th>Place of delivery</th>
</tr>
</thead>
<tbody>
<tr><td>1</td><td></td><td></td><td></td><td></td><td></td><td></td><td></td><td></td><td></td></tr>
<tr><td>2</td><td></td><td></td><td></td><td></td><td></td><td></td><td></td><td></td><td></td></tr>
<tr><td>3</td><td></td><td></td><td></td><td></td><td></td><td></td><td></td><td></td><td></td></tr>
<tr><td>4</td><td></td><td></td><td></td><td></td><td></td><td></td><td></td><td></td><td></td></tr>
<tr><td>5</td><td></td><td></td><td></td><td></td><td></td><td></td><td></td><td></td><td></td></tr>
</tbody>
</table>
</div>
<div style="display:flex;gap:6px;flex-wrap:wrap;margin-top:8px;font-size:10px;">
<div style="background:#f7fafc;border:1px solid #e2e8f0;border-radius:5px;padding:4px 8px;"><strong>Mode codes:</strong> SVD = Spontaneous Vaginal | IOL = Induced | LSCS = Lower Segment CS | ECS = Emergency CS | F = Forceps | V = Ventouse</div>
<div style="background:#fff5f5;border:1px solid #feb2b2;border-radius:5px;padding:4px 8px;"><span style="color:#c53030;">⚠️ Red flags:</span> Previous LSCS → VBAC vs repeat CS | PPH → alert team | Pre-eclampsia → 20% recurrence | GDM → 50% recurrence</div>
</div>
</div>
</div>
</div>
<!-- ══════════ ROW 6: PMH + Drugs + Family ══════════ -->
<div class="grid-3">
<!-- PMH -->
<div class="card orange">
<div class="card-header">
<div class="icon">🩺</div>
<div class="title">Past Medical & Surgical Hx</div>
<div class="subtitle">MJ THREADS</div>
</div>
<div class="card-body">
<div class="mbox">
<div class="mbox-item" style="background:#fffaf0;border:1.5px solid #fbd38d;">
<span class="letter" style="color:#744210;">M</span>
<span class="word" style="color:#7b341e;">MI/Cardiac</span>
</div>
<div class="mbox-item" style="background:#fffaf0;border:1.5px solid #fbd38d;">
<span class="letter" style="color:#744210;">J</span>
<span class="word" style="color:#7b341e;">Jaundice</span>
</div>
<div class="mbox-item" style="background:#fffaf0;border:1.5px solid #fbd38d;">
<span class="letter" style="color:#744210;">T</span>
<span class="word" style="color:#7b341e;">Thyroid</span>
</div>
<div class="mbox-item" style="background:#fffaf0;border:1.5px solid #fbd38d;">
<span class="letter" style="color:#744210;">H</span>
<span class="word" style="color:#7b341e;">Hypertension</span>
</div>
<div class="mbox-item" style="background:#fffaf0;border:1.5px solid #fbd38d;">
<span class="letter" style="color:#744210;">R</span>
<span class="word" style="color:#7b341e;">Rheumatol</span>
</div>
<div class="mbox-item" style="background:#fffaf0;border:1.5px solid #fbd38d;">
<span class="letter" style="color:#744210;">E</span>
<span class="word" style="color:#7b341e;">Epilepsy</span>
</div>
<div class="mbox-item" style="background:#fffaf0;border:1.5px solid #fbd38d;">
<span class="letter" style="color:#744210;">A</span>
<span class="word" style="color:#7b341e;">Anaemia</span>
</div>
<div class="mbox-item" style="background:#fffaf0;border:1.5px solid #fbd38d;">
<span class="letter" style="color:#744210;">D</span>
<span class="word" style="color:#7b341e;">Diabetes</span>
</div>
<div class="mbox-item" style="background:#fffaf0;border:1.5px solid #fbd38d;">
<span class="letter" style="color:#744210;">S</span>
<span class="word" style="color:#7b341e;">Surgery</span>
</div>
</div>
<div class="chk-list cols-3" style="margin-top:6px;">
<div class="chk-item"><div class="chk-box"></div> Hypertension</div>
<div class="chk-item"><div class="chk-box"></div> Diabetes</div>
<div class="chk-item"><div class="chk-box"></div> Anaemia</div>
<div class="chk-item"><div class="chk-box"></div> Sickle cell</div>
<div class="chk-item"><div class="chk-box"></div> Thalassaemia</div>
<div class="chk-item"><div class="chk-box"></div> Cardiac disease</div>
<div class="chk-item"><div class="chk-box"></div> Epilepsy</div>
<div class="chk-item"><div class="chk-box"></div> Thyroid</div>
<div class="chk-item"><div class="chk-box"></div> HIV / TB</div>
<div class="chk-item"><div class="chk-box"></div> Malaria</div>
<div class="chk-item"><div class="chk-box"></div> Renal disease</div>
<div class="chk-item"><div class="chk-box"></div> Asthma</div>
<div class="chk-item"><div class="chk-box"></div> SLE</div>
<div class="chk-item"><div class="chk-box"></div> DVT/PE</div>
<div class="chk-item"><div class="chk-box"></div> Previous surgery</div>
</div>
<div class="sec-heading" style="margin-top:8px;">Details</div>
<div class="write-lines">
<div class="wl"></div><div class="wl"></div><div class="wl"></div>
</div>
</div>
</div>
<!-- Drugs + Allergies -->
<div class="card pink">
<div class="card-header">
<div class="icon">💊</div>
<div class="title">Drug History & Allergies</div>
</div>
<div class="card-body">
<div class="sec-heading">Current Medications</div>
<table class="mini-table">
<tr><th>Drug Name</th><th>Dose</th><th>Route</th><th>Duration</th></tr>
<tr><td></td><td></td><td></td><td></td></tr>
<tr><td></td><td></td><td></td><td></td></tr>
<tr><td></td><td></td><td></td><td></td></tr>
<tr><td></td><td></td><td></td><td></td></tr>
</table>
<div class="sec-heading">⚠️ Teratogenic Drugs — Screen for</div>
<div class="chk-list">
<div class="chk-item"><div class="chk-box"></div> Methotrexate</div>
<div class="chk-item"><div class="chk-box"></div> Warfarin</div>
<div class="chk-item"><div class="chk-box"></div> Sodium valproate</div>
<div class="chk-item"><div class="chk-box"></div> Retinoids (Vit A)</div>
<div class="chk-item"><div class="chk-box"></div> ACE inhibitors</div>
<div class="chk-item"><div class="chk-box"></div> Lithium</div>
<div class="chk-item"><div class="chk-box"></div> Thalidomide</div>
<div class="chk-item"><div class="chk-box"></div> Tetracyclines</div>
</div>
<div class="sec-heading">Folic Acid</div>
<div style="display:flex;gap:6px;font-size:10px;margin:4px 0;">
<div style="flex:1;background:#f0fff4;border:1px solid #c6f6d5;border-radius:5px;padding:5px 7px;">
<strong style="color:#276749;">Standard</strong><br>400 mcg/day<br>Pre-conception → 12 wks
</div>
<div style="flex:1;background:#fff5f5;border:1px solid #feb2b2;border-radius:5px;padding:5px 7px;">
<strong style="color:#c53030;">High-risk*</strong><br>5 mg/day<br>Epilepsy/DM/BMI>30<br>Previous NTD
</div>
</div>
<div class="sec-heading">🚫 Allergies</div>
<table class="mini-table">
<tr><th>Drug / Substance</th><th>Type of Reaction</th><th>Severity</th></tr>
<tr><td></td><td></td><td></td></tr>
<tr><td></td><td></td><td></td></tr>
</table>
</div>
</div>
<!-- Family + Social Hx -->
<div class="card brown">
<div class="card-header">
<div class="icon">👨👩👧</div>
<div class="title">Family & Social History</div>
<div class="subtitle">HEADS-SS</div>
</div>
<div class="card-body">
<div class="sec-heading">Family History</div>
<div class="chk-list">
<div class="chk-item"><div class="chk-box"></div> Hypertension</div>
<div class="chk-item"><div class="chk-box"></div> Diabetes</div>
<div class="chk-item"><div class="chk-box"></div> Pre-eclampsia</div>
<div class="chk-item"><div class="chk-box"></div> Multiple gestation</div>
<div class="chk-item"><div class="chk-box"></div> Sickle cell / thalassaemia</div>
<div class="chk-item"><div class="chk-box"></div> Congenital anomalies</div>
<div class="chk-item"><div class="chk-box"></div> DVT / thrombophilia</div>
<div class="chk-item"><div class="chk-box"></div> Breast/ovarian cancer</div>
</div>
<div class="item" style="margin-top:6px;"><div class="item-dot" style="background:#d69e2e;"></div><div class="item-label">Details:</div><div class="item-line"></div></div>
<div class="sec-heading">Social History — HEADS-SS</div>
<div class="mbox">
<div class="mbox-item" style="background:#fffff0;border:1.5px solid #f6e05e;">
<span class="letter" style="color:#744210;">H</span>
<span class="word" style="color:#7b341e;">Home</span>
</div>
<div class="mbox-item" style="background:#fffff0;border:1.5px solid #f6e05e;">
<span class="letter" style="color:#744210;">E</span>
<span class="word" style="color:#7b341e;">Employment</span>
</div>
<div class="mbox-item" style="background:#fffff0;border:1.5px solid #f6e05e;">
<span class="letter" style="color:#744210;">A</span>
<span class="word" style="color:#7b341e;">Alcohol</span>
</div>
<div class="mbox-item" style="background:#fffff0;border:1.5px solid #f6e05e;">
<span class="letter" style="color:#744210;">D</span>
<span class="word" style="color:#7b341e;">Drugs</span>
</div>
<div class="mbox-item" style="background:#fffff0;border:1.5px solid #f6e05e;">
<span class="letter" style="color:#744210;">S</span>
<span class="word" style="color:#7b341e;">Smoking</span>
</div>
<div class="mbox-item" style="background:#fffff0;border:1.5px solid #f6e05e;">
<span class="letter" style="color:#744210;">S</span>
<span class="word" style="color:#7b341e;">Support</span>
</div>
<div class="mbox-item" style="background:#fffff0;border:1.5px solid #f6e05e;">
<span class="letter" style="color:#744210;">S</span>
<span class="word" style="color:#7b341e;">Stress / MH</span>
</div>
</div>
<div class="item"><div class="item-dot" style="background:#d69e2e;"></div><div class="item-label">Home/Support:</div><div class="item-line"></div></div>
<div class="item"><div class="item-dot" style="background:#d69e2e;"></div><div class="item-label">Occupation:</div><div class="item-line"></div></div>
<div class="item"><div class="item-dot" style="background:#d69e2e;"></div>
<div style="font-size:11px;font-weight:600;min-width:100px;">Smoking:</div>
<div style="display:flex;gap:6px;align-items:center;flex:1;">
<div class="chk-item"><div class="chk-box"></div> Yes</div>
<div class="chk-item"><div class="chk-box"></div> No</div>
<div class="chk-item"><div class="chk-box"></div> Ex</div>
<div style="flex:1;border-bottom:1px solid #e2e8f0;height:18px;"></div>
</div>
</div>
<div class="item"><div class="item-dot" style="background:#d69e2e;"></div>
<div style="font-size:11px;font-weight:600;min-width:100px;">Alcohol:</div>
<div style="display:flex;gap:6px;align-items:center;flex:1;">
<div class="chk-item"><div class="chk-box"></div> None</div>
<div class="chk-item"><div class="chk-box"></div> Occasional</div>
<div class="chk-item"><div class="chk-box"></div> Regular</div>
</div>
</div>
<div class="item"><div class="item-dot" style="background:#d69e2e;"></div><div class="item-label">Rec. drugs:</div><div class="item-line"></div></div>
<div class="item"><div class="item-dot" style="background:#d69e2e;"></div><div class="item-label">Mental health:</div><div class="item-line"></div></div>
<div style="background:#fffbeb;border:1px solid #f6e05e;border-radius:5px;padding:5px 8px;font-size:10px;color:#744210;margin-top:4px;">
⚠️ Screen for <strong>domestic violence</strong> in private: "Are you safe at home?"
</div>
</div>
</div>
</div>
<!-- ══════════ ROW 7: Systems Review + Summary ══════════ -->
<div class="grid-2">
<!-- Systems Review -->
<div class="card teal">
<div class="card-header">
<div class="icon">🔍</div>
<div class="title">Systems Review (Obstetric Relevant)</div>
</div>
<div class="card-body">
<div class="grid-2" style="gap:6px;margin-bottom:0;">
<div>
<div class="sec-heading">Cardiovascular</div>
<div class="chk-list">
<div class="chk-item"><div class="chk-box"></div> Palpitations</div>
<div class="chk-item"><div class="chk-box"></div> Chest pain</div>
<div class="chk-item"><div class="chk-box"></div> SOB</div>
<div class="chk-item"><div class="chk-box"></div> Ankle swelling</div>
</div>
<div class="sec-heading">Respiratory</div>
<div class="chk-list">
<div class="chk-item"><div class="chk-box"></div> Cough</div>
<div class="chk-item"><div class="chk-box"></div> Wheeze</div>
<div class="chk-item"><div class="chk-box"></div> Haemoptysis</div>
<div class="chk-item"><div class="chk-box"></div> Dyspnoea</div>
</div>
<div class="sec-heading">GI / Hepatic</div>
<div class="chk-list">
<div class="chk-item"><div class="chk-box"></div> Nausea / vomiting</div>
<div class="chk-item"><div class="chk-box"></div> Heartburn/GORD</div>
<div class="chk-item"><div class="chk-box"></div> Constipation</div>
<div class="chk-item"><div class="chk-box"></div> Jaundice</div>
<div class="chk-item"><div class="chk-box"></div> Pruritus (itching)</div>
<div class="chk-item"><div class="chk-box"></div> RUQ pain</div>
</div>
</div>
<div>
<div class="sec-heading">Urinary</div>
<div class="chk-list">
<div class="chk-item"><div class="chk-box"></div> Dysuria</div>
<div class="chk-item"><div class="chk-box"></div> Frequency</div>
<div class="chk-item"><div class="chk-box"></div> Haematuria</div>
<div class="chk-item"><div class="chk-box"></div> Incontinence</div>
</div>
<div class="sec-heading">Neurological</div>
<div class="chk-list">
<div class="chk-item"><div class="chk-box"></div> Headache</div>
<div class="chk-item"><div class="chk-box"></div> Visual change</div>
<div class="chk-item"><div class="chk-box"></div> Fits/seizures</div>
<div class="chk-item"><div class="chk-box"></div> Dizziness</div>
</div>
<div class="sec-heading">MSK / Other</div>
<div class="chk-list">
<div class="chk-item"><div class="chk-box"></div> Pelvic girdle pain</div>
<div class="chk-item"><div class="chk-box"></div> Back pain</div>
<div class="chk-item"><div class="chk-box"></div> Leg cramps</div>
<div class="chk-item"><div class="chk-box"></div> Calf pain/DVT</div>
</div>
</div>
</div>
</div>
</div>
<!-- Clinical Summary + Plan -->
<div class="card blue">
<div class="card-header">
<div class="icon">📝</div>
<div class="title">Clinical Summary & Management Plan</div>
</div>
<div class="card-body">
<div class="sec-heading">Summary Statement</div>
<div style="font-size:11px;color:#4a5568;margin-bottom:5px;background:#ebf8ff;padding:5px 8px;border-radius:6px;border:1px solid #bee3f8;">
<em>"Mrs ___, a ___-year-old G__P__+__, at ___ weeks gestation by LMP/USS, presenting with ___"</em>
</div>
<div class="write-lines">
<div class="wl"></div><div class="wl"></div><div class="wl"></div>
</div>
<div class="sec-heading">Risk Stratification</div>
<div style="display:flex;gap:6px;margin-bottom:6px;">
<div style="flex:1;background:#f0fff4;border:2px solid #68d391;border-radius:7px;padding:6px;text-align:center;font-size:11px;">
<div style="font-weight:700;color:#276749;">LOW RISK</div>
<div class="chk-box" style="margin:4px auto;"></div>
</div>
<div style="flex:1;background:#fffbeb;border:2px solid #f6e05e;border-radius:7px;padding:6px;text-align:center;font-size:11px;">
<div style="font-weight:700;color:#744210;">MODERATE</div>
<div class="chk-box" style="margin:4px auto;"></div>
</div>
<div style="flex:1;background:#fff5f5;border:2px solid #fc8181;border-radius:7px;padding:6px;text-align:center;font-size:11px;">
<div style="font-weight:700;color:#c53030;">HIGH RISK</div>
<div class="chk-box" style="margin:4px auto;"></div>
</div>
</div>
<div class="sec-heading">Investigations Ordered</div>
<div class="chk-list cols-3">
<div class="chk-item"><div class="chk-box"></div> FBC</div>
<div class="chk-item"><div class="chk-box"></div> USS</div>
<div class="chk-item"><div class="chk-box"></div> Blood group</div>
<div class="chk-item"><div class="chk-box"></div> LFTs</div>
<div class="chk-item"><div class="chk-box"></div> RFTs</div>
<div class="chk-item"><div class="chk-box"></div> Urine dip</div>
<div class="chk-item"><div class="chk-box"></div> CTG</div>
<div class="chk-item"><div class="chk-box"></div> OGTT/BSL</div>
<div class="chk-item"><div class="chk-box"></div> HIV/VDRL</div>
</div>
<div class="sec-heading">Management Plan</div>
<div class="write-lines">
<div class="wl"></div><div class="wl"></div><div class="wl"></div><div class="wl"></div>
</div>
<div class="sec-heading">Next Review</div>
<div class="item"><div class="item-dot" style="background:#4299e1;"></div><div class="item-label">Date/Time:</div><div class="item-line"></div></div>
<div class="item"><div class="item-dot" style="background:#4299e1;"></div><div class="item-label">Clinician:</div><div class="item-line"></div></div>
<div class="item"><div class="item-dot" style="background:#4299e1;"></div><div class="item-label">Signature:</div><div class="item-line"></div></div>
</div>
</div>
</div>
<!-- ══════════ FOOTER ══════════ -->
<div class="footer">
<strong>Obstetric History Taking — Smart Memory Aid</strong> |
Based on RCOG, WHO ANC Framework, Berek & Novak's Gynecology, Harriet Lane Handbook |
For educational use | Print this sheet for clinical clerkship
</div>
</div>
</body>
</html>
1. How to clerk an obstetrics patient, questions to ask during obstetrics history taking detailed smart made easy
How to clerk an obstetrics patient, questions to ask during obstetrics history taking detailed smart made easy
Write me full obstetrics history with examples scenarios and explanations and tablets where appropriate
Medicine : respiratory system made easy detailed exam oriented
Generate a detailed exam-focused respiratory medicine summary as a Word document
Generate a comprehensive respiratory medicine Word document when your credits reset
Clinical pathology: respiratory system upper and lower comprehensive exam oriented
Notes
Hi
Create a study guide on common obstetric presentations
Create a Word document with common obstetric presentations
Discuss different types of pain based on duration,location,course,intensity and pathophysiology
Discuss different types of pain based on duration,location,course,intensity and pathophysiology
Pharmacology and therapeutics: comprehensive notes on autocoids on Pharmacological basis as a pptx in clean visible structured
Prepare exam-focused autocoid pharmacology with drug tables and mnemonics
Generate a comprehensive notes on pediatric pneumonia with guidelines, classification, and protocols...exam oriented detailed made easy, mnemonics
Hi
our setting medical surgical nursing contains this units 1.med surge itself 2.cardiovascular system 3pulmonary nursing4.Gud 5.haematology