Macular hole
Reading File
Finding Sources
Searching PubMed
"macular hole" AND surgery
Reading File
Reading File
Reading File
Searching Images
macular hole OCT fundus
Reading File
Finding Sources
Reading File
I now have comprehensive information. Let me compile the full response.
Full-Thickness Macular Hole (FTMH)
Definition & Epidemiology
A macular hole is a full-thickness defect involving all retinal layers at the fovea. It is a relatively common cause of central visual loss, with a prevalence of ~3:1000. It predominantly affects females aged 60–70 and is bilateral on presentation in ~30% of cases.
Pathophysiology
The primary mechanism is vitreomacular traction (VMT). In early VMA/VMT, the vitreous cortex remains adherent to the fovea while detaching from the perifoveal region, creating anteroposterior traction. This leads to:
- Detachment of inner retinal layers from photoreceptors
- Cyst-like schisis cavity formation
- Centrifugal displacement of photoreceptors
- Progressive full-thickness dehiscence
Other causes include high myopia (can also cause macular retinal detachment) and blunt ocular trauma.
Classification
IVTS (OCT-Based) Classification — Current Standard
| Category | Size | VMT |
|---|---|---|
| VMT (no hole) | — | Present, distorts foveal contour |
| Small FTMH | < 250 μm (narrowest point) | ± VMT |
| Medium FTMH | 250–400 μm | ± VMT |
| Large FTMH | > 400 μm | ± VMT |
Gass Clinical Staging — Historical (Still Widely Referenced)
| Stage | Description |
|---|---|
| Stage 1 | Impending hole — yellow spot or ring at fovea, no full-thickness defect |
| Stage 2 | Small full-thickness hole (< 400 μm), inner retinal dehiscence, vitreous still attached |
| Stage 3 | Full-thickness hole (> 400 μm) + cuff of subretinal fluid, no PVD |
| Stage 4 | Full-thickness hole + cuff of SRF + complete PVD (Weiss ring present) |
A new OCT-based classification (IVTS) has replaced Gass staging as the clinical standard but Gass stages remain embedded in clinical practice and exams.
Clinical Features
Symptoms:
- Central visual loss (often first noticed when the fellow eye is covered)
- Metamorphopsia
- Stage 1 may be asymptomatic
Signs (slit-lamp biomicroscopy + OCT):
- Stage 3/4: round red defect at fovea, yellow-white dots at base, grey cuff of subretinal fluid
- Stage 4: operculum (pseudo-operculum) may be visible suspended in vitreous — composed primarily of glial tissue + condensed vitreous (40% contain photoreceptor elements)
- VA commonly reduced to 6/60 in large holes
OCT findings: Full-thickness foveal defect, everted hole edges, intraretinal cystic spaces, subretinal fluid cuff, disruption of ellipsoid zone (EZ) and external limiting membrane (ELM).
OCT Images
Traumatic macular hole — fundus + OCT progression (Stage 3 → Stage 4):
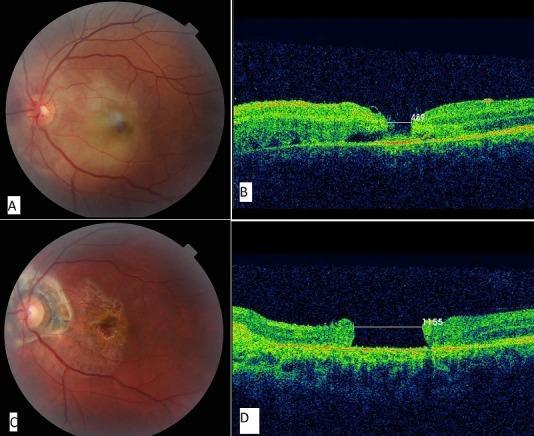
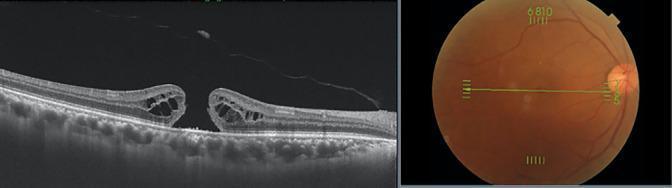
Stage 3 macular hole — classic OCT features (operculum, subretinal fluid, PVD):
Differential Diagnosis
| Condition | Key Distinguishing Feature |
|---|---|
| Pseudohole (ERM) | No loss of foveal tissue; ERM sheen visible; Watzke-Allen test shows distortion, not break |
| Lamellar macular hole | Partial thickness; less red; no grey halo; OCT confirms |
| Cystoid macular edema | Intraretinal cysts; associated with underlying disease |
| Solar retinopathy | Small yellow/red foveal lesion; history of sun gazing |
Watzke–Allen Test: A thin slit beam directed across the fovea — a broken line = true FTMH; a distorted but unbroken line = pseudohole/lamellar hole.
Workup
- History — trauma, myopia, prior eye surgery, sun exposure
- Slit-lamp biomicroscopy with 60/90D or fundus contact lens
- Watzke–Allen test
- OCT — gold standard for staging, distinguishing FTMH from lamellar/pseudohole, evaluating vitreoretinal interface
- IVFA — if vascular etiology (DR, RVO, CME) suspected
Treatment
Stage 1 (Impending)
- Observation — ~50% resolve spontaneously
Pharmacological — Ocriplasmin
- Recombinant truncated plasmin (acts on fibronectin and laminin at vitreoretinal interface)
- FDA-approved for symptomatic VMA, VMT, and small macular holes
- Limited uptake due to inconsistent efficacy and side effects: ERG changes, lens subluxation, dyschromatopsia
Surgery — Gold Standard for Symptomatic FTMH (Stage 2+)
Pars plana vitrectomy (PPV) with:
- (a) ILM peeling facilitated by vital dye (e.g., brilliant blue)
- (b) Relief of VMT (induction of PVD if not present, or removal of perifoveal vitreous)
- (c) Gas tamponade (SF₆ or C₃F₈)
- Postoperative face-down positioning (8 hours/day × 5 days) — improves closure rates; not required for as long with modern techniques
Outcomes:
- Hole closure: majority of cases
- Visual improvement: 80–90% over months
- Final VA ≥ 6/12: ~65%
- Worsening of VA: up to 10%
- Residual OCT abnormality (IS/OS defect) common even after successful closure
Timing matters: Symptom duration strongly correlates with outcome. Operating within 6 months of onset gives the best visual recovery.
Complications: Same as vitrectomy generally — cataract progression (near-universal in phakic patients), retinal detachment, endophthalmitis.
Emerging — Intravitreal gas injection
Preliminary studies suggest that injection of a small bolus of gas alone (without full vitrectomy) may achieve hole closure — still under investigation.
Fellow Eye
- Risk of fellow eye involvement within 5 years: ~10%
- Risk is lower if a PVD is already present in the fellow eye
Recent Evidence (2024–2025)
Three high-quality meta-analyses have recently addressed key surgical controversies:
- ILM flap vs. ILM peeling — A 2025 systematic review and meta-analysis found ILM flap techniques may offer advantages for larger holes (PMID: 40197272)
- ILM flap — individual participant data meta-analysis — Further supports ILM flap benefit, particularly for large/refractory holes (PMID: 39923898)
- Face-down positioning — A 2025 individual participant data meta-analysis questions the necessity of strict face-down positioning in modern surgery (PMID: 39147105)
Sources: Kanski's Clinical Ophthalmology 10th Ed., p. 626–629 | Wills Eye Manual, p. 868–870
This is a shared conversation. Sign in to Orris to start your own chat.