.what aregram- and gram + bacteria's
Reading File
Finding Sources
Searching the Web
gram positive vs gram negative bacteria differences cell wall examples
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Reading File
Here is a thorough breakdown of Gram-positive and Gram-negative bacteria, backed by medical microbiology textbooks.
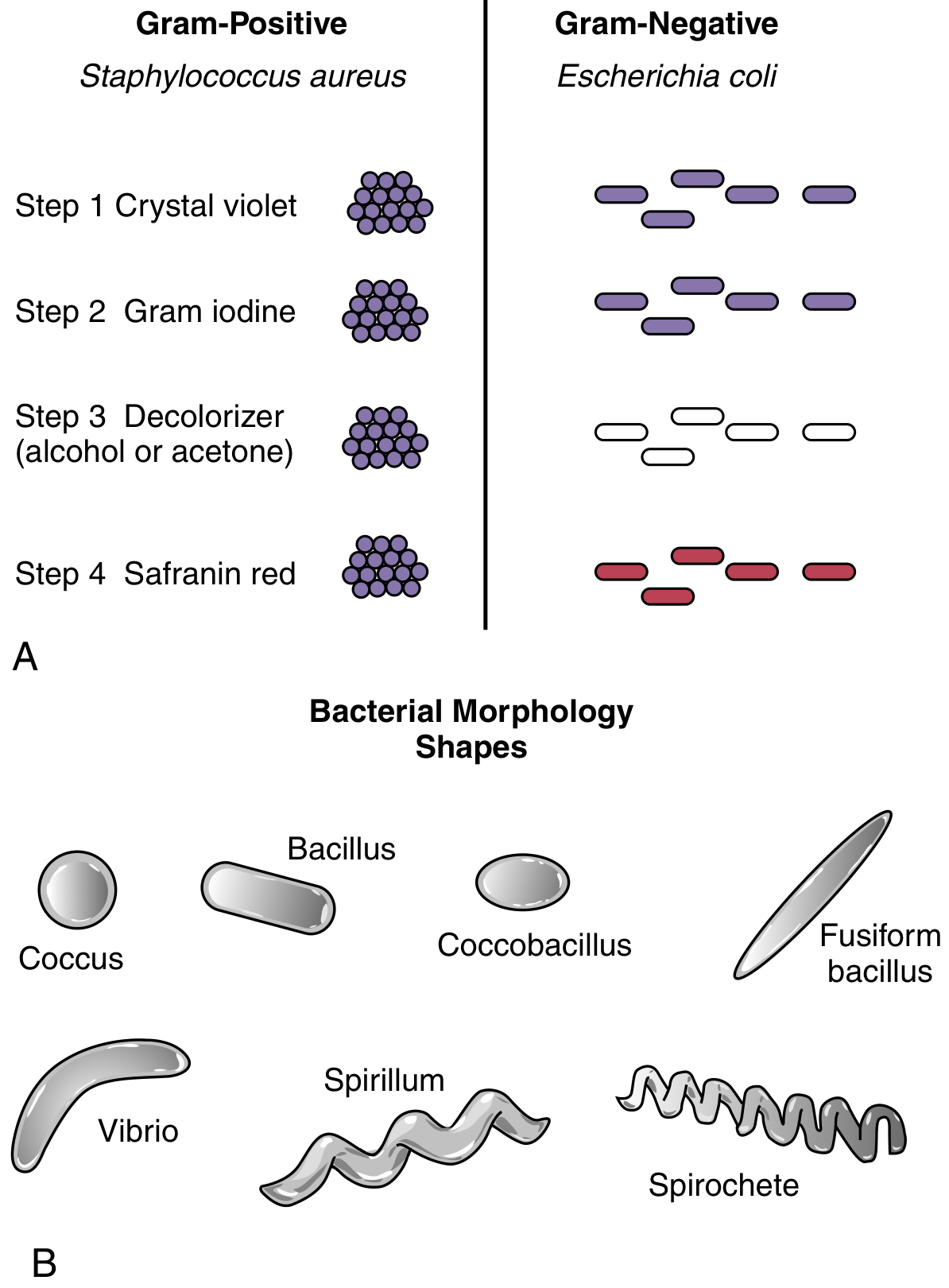
Gram Staining - The Basis of Classification
The Gram stain, developed by Hans Christian Gram, divides bacteria into two major categories based on the chemical and physical properties of their cell walls. The four-step process works as follows:
| Step | Reagent | Gram-Positive | Gram-Negative |
|---|---|---|---|
| 1 | Crystal violet | Stains purple | Stains purple |
| 2 | Gram iodine (mordant) | Crystal violet locked in | Crystal violet locked in |
| 3 | Decolorizer (alcohol/acetone) | Stays purple - thick wall traps dye | Loses color - thin wall washed out |
| 4 | Safranin (counterstain) | Still purple (pink masked) | Turns pink/red |
Cell Wall Structure - The Key Difference
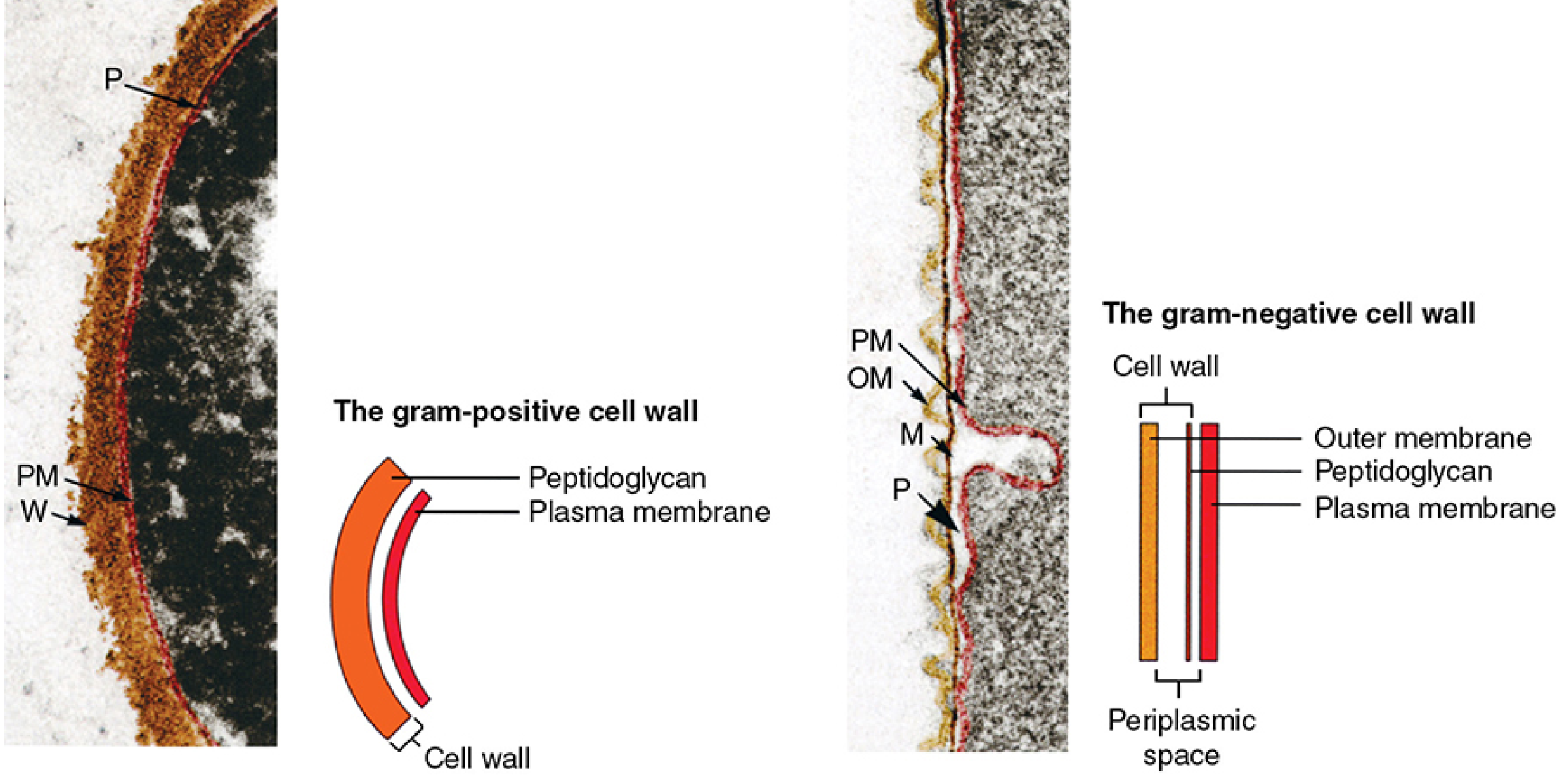
Gram-Positive Bacteria
Structure:
- Thick peptidoglycan layer (20-80 nm, up to ~30 layers)
- Single plasma membrane (monoderm)
- Contains teichoic acids (wall teichoic acid + lipoteichoic acid anchored to plasma membrane)
- NO outer membrane, NO periplasmic space (or minimal)
Peptidoglycan is a rigid, scaffold-like sac made of alternating sugars - N-acetylglucosamine (NAG) and N-acetylmuramic acid (NAM) - cross-linked by peptide chains. This thick layer traps crystal violet and resists decolorization.
- Sherris & Ryan's Medical Microbiology, p. 813-814
Clinical significance:
- Teichoic acids can trigger immune responses
- Peptidoglycan fragments released during infection cause cytokine release and systemic inflammation
- Penicillin targets peptidoglycan synthesis - particularly effective
Common Gram-positive organisms:
| Organism | Type | Disease |
|---|---|---|
| Staphylococcus aureus | Coccus | Skin infections, sepsis, endocarditis |
| Staphylococcus epidermidis | Coccus | Device-related infections |
| Streptococcus pneumoniae | Coccus | Pneumonia, meningitis |
| Streptococcus pyogenes | Coccus | Pharyngitis, rheumatic fever |
| Enterococcus spp. | Coccus | UTI, endocarditis |
| Bacillus anthracis | Rod (bacillus) | Anthrax |
| Clostridium spp. | Rod | Tetanus, botulism, C. diff colitis |
| Corynebacterium diphtheriae | Rod | Diphtheria |
| Listeria monocytogenes | Rod | Listeriosis (meningitis in neonates) |
| Mycobacterium tuberculosis | Rod | Tuberculosis (technically G+ by cell wall, but acid-fast) |
Gram-Negative Bacteria
Structure:
- Thin peptidoglycan layer (2-7 nm, 1-2 layers)
- Two membranes (diderm): inner cytoplasmic membrane + outer membrane (OM)
- Periplasmic space between the two membranes containing enzymes and transport proteins
- Outer membrane contains lipopolysaccharide (LPS) - also called endotoxin
- Outer membrane attached to peptidoglycan via lipoproteins
The outer membrane's LPS (endotoxin) is a major virulence factor - it can trigger septic shock, fever, and multi-organ failure when released into the bloodstream.
- Medical Microbiology 9e, p. 140-141
Clinical significance:
- LPS/endotoxin drives severe inflammatory responses and septic shock
- The outer membrane acts as a permeability barrier - many antibiotics cannot penetrate it
- Beta-lactamases (resistance enzymes) often accumulate in the periplasmic space
- Treatment requires antibiotics that can penetrate the outer membrane (e.g., carbapenems, fluoroquinolones)
Common Gram-negative organisms:
| Organism | Type | Disease |
|---|---|---|
| Escherichia coli | Rod | UTI, sepsis, neonatal meningitis |
| Klebsiella pneumoniae | Rod | Pneumonia, UTI |
| Pseudomonas aeruginosa | Rod | Hospital infections, burns |
| Neisseria meningitidis | Coccus | Bacterial meningitis |
| Neisseria gonorrhoeae | Coccus | Gonorrhea |
| Haemophilus influenzae | Rod | Meningitis, respiratory infections |
| Salmonella typhi | Rod | Typhoid fever |
| Vibrio cholerae | Rod (curved) | Cholera |
| Helicobacter pylori | Rod (curved) | Peptic ulcer, gastric cancer |
| Treponema pallidum | Spirochete | Syphilis |
| Campylobacter spp. | Rod | Food poisoning, diarrhea |
Side-by-Side Comparison
| Feature | Gram-Positive | Gram-Negative |
|---|---|---|
| Gram stain color | Purple/violet | Pink/red |
| Peptidoglycan layer | Thick (20-80 nm) | Thin (2-7 nm) |
| Outer membrane | Absent | Present |
| Teichoic acids | Present | Absent |
| LPS (endotoxin) | Absent | Present |
| Periplasmic space | Minimal/absent | Present |
| Membranes | 1 (monoderm) | 2 (diderm) |
| Susceptibility to penicillin | Generally higher | Generally lower |
| Lysozyme sensitivity | Higher | Lower (outer membrane protects) |
| Toxin type | Exotoxins (secreted proteins) | Endotoxin (LPS) |
Special Notes
- Mycobacteria (e.g., M. tuberculosis): Technically Gram-positive by cell wall chemistry, but their wall is rich in waxy mycolic acids that resist Gram stain uptake - they are identified by the acid-fast (Ziehl-Neelsen) stain instead.
- Mycoplasma: No cell wall at all - not classifiable by Gram stain; naturally resistant to penicillin.
Source: Sherris & Ryan's Medical Microbiology, 8th ed. | Medical Microbiology 9e | Jawetz, Melnick & Adelberg's Medical Microbiology, 28th ed.
What is shock
Finding Sources
Searching the Web
shock pathophysiology types classification medical
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
I now have a thorough base from Harrison's, Robbins & Kumar Pathologic Basis of Disease, and Robbins & Kumar Basic Pathology. Here is the complete answer:
Shock
Definition
Shock is a state of circulatory failure that impairs tissue perfusion and leads to cellular hypoxia. When the delivery of oxygen and nutrients to tissues falls below what cells need for normal metabolism, energy production fails, cellular injury begins, and - if untreated - the process becomes irreversible and fatal.
"Shock is a state of systemic tissue hypoperfusion resulting from reduced cardiac output and/or reduced effective circulating blood volume."
- Robbins, Cotran & Kumar Pathologic Basis of Disease
Types of Shock
There are four major categories, each with a distinct mechanism:
1. Hypovolemic Shock
- Cause: Reduced blood or plasma volume
- Examples: Hemorrhage (trauma, GI bleed), burns, severe vomiting/diarrhea, fluid loss
- Mechanism: Low circulating volume → reduced venous return → reduced cardiac output (CO) → tissue hypoperfusion
- Hemodynamics: ↓CVP, ↓PCWP, ↓CO, ↑SVR (compensatory vasoconstriction)
2. Cardiogenic Shock
- Cause: The heart fails to pump adequately
- Examples: Myocardial infarction, ventricular rupture, severe arrhythmias, cardiac tamponade, pulmonary embolism
- Mechanism: Pump failure → ↓CO → inadequate oxygen delivery despite normal blood volume
- Hemodynamics: ↑CVP, ↑PCWP, ↓CO, ↑SVR
3. Distributive Shock
Vasodilation causes maldistribution of blood flow - blood volume is normal but not reaching tissues effectively. Three subtypes:
| Subtype | Trigger | Mechanism |
|---|---|---|
| Septic | Bacterial/fungal infection | Cytokine storm → vasodilation, endothelial injury, DIC |
| Anaphylactic | IgE-mediated allergen (food, drugs, insect bite) | Histamine release → massive vasodilation + vascular leakage (up to 35% of circulating volume lost in 10 min) |
| Neurogenic | Spinal cord injury, anesthesia | Loss of sympathetic vascular tone → venous pooling → ↓venous return |
- Hemodynamics: ↓CVP, ↓PCWP, ↑CO (early), ↓SVR
4. Obstructive Shock
- Cause: Physical blockage of blood flow in a major circuit
- Examples: Massive pulmonary embolism, cardiac tamponade, tension pneumothorax
- Mechanism: Obstruction prevents adequate cardiac filling or output
- Hemodynamics: ↑CVP, ↓/↑PCWP, ↓CO, ↑SVR
Hemodynamic Summary Table
(from Harrison's Principles of Internal Medicine, 22nd ed.)
| Type | CVP | PCWP | Cardiac Output | SVR |
|---|---|---|---|---|
| Distributive | ↓ | ↓ | ↑ | ↓ |
| Cardiogenic | ↑ | ↑ | ↓ | ↑ |
| Obstructive | ↑ | ↓/↑ | ↓ | ↑ |
| Hypovolemic | ↓ | ↓ | ↓ | ↑ |
Stages of Shock
Regardless of type, shock evolves through three progressive stages:
Stage 1 - Compensated (Non-progressive) Shock
- The body activates compensatory mechanisms to maintain vital organ perfusion
- Baroreceptor reflexes, catecholamines, ADH release, RAAS activation, sympathetic stimulation
- Net result: tachycardia, peripheral vasoconstriction, renal fluid conservation
- Blood is shunted away from skin to the heart and brain
- Skin becomes cool and pale (except in septic shock - skin may initially be warm and flushed)
- No overt organ dysfunction yet; lab may show mild ↑creatinine or ↑lactate
- Reversible with treatment
Stage 2 - Decompensated (Progressive) Shock
- Compensatory mechanisms are overwhelmed
- Widespread tissue hypoxia triggers anaerobic glycolysis → lactic acidosis
- Falling tissue pH causes arteriolar dilation → blood pools in microcirculation
- Worsening CO + endothelial injury → risk of DIC
- Vital organs begin to fail (kidney, lung, brain, gut)
- Still reversible if treated aggressively
Stage 3 - Irreversible Shock
- Widespread cell injury → lysosomal enzyme leakage → further tissue destruction
- Myocardial contractility declines (partly from excess NO synthesis)
- Ischemic gut may release bacteria into the circulation (superimposed bacteremic shock)
- Renal failure from ischemia
- Multi-organ failure and death despite all interventions
Pathophysiology of Septic Shock (in detail)
Septic shock deserves special mention as it is the most complex and one of the most lethal forms:
- Inflammatory mediators: Microbial PAMPs (e.g., LPS from gram-negative bacteria, peptidoglycan from gram-positives) activate Toll-like receptors → release of TNF, IL-1, IL-6, and other cytokines
- Endothelial activation and injury: Cytokines loosen tight junctions → vascular leakage → edema → impaired O₂ delivery. Upregulation of NO → systemic vasodilation and hypotension
- Procoagulant state: Cytokines increase tissue factor → triggers clotting cascade → disseminated intravascular coagulation (DIC) in up to 50% of patients
- Metabolic derangements: Insulin resistance, hyperglycemia, elevated lactate and triglycerides, lactic acidosis
- Organ dysfunction: Hypotension + edema + microvascular thrombosis → multi-organ failure (kidneys, lungs → ARDS, heart, brain)
- Mortality remains 20-40% despite modern intensive care
- Most frequently triggered by gram-positive bacteria, then gram-negatives, then fungi
Morphological Changes in Shock (Organ Effects)
Any organ can be affected, but these are most commonly involved:
| Organ | Changes |
|---|---|
| Brain | Ischemic encephalopathy |
| Heart | Subendocardial hemorrhage and necrosis |
| Kidneys | Acute tubular necrosis (most common cause of acute kidney injury in shock) |
| Lungs | ARDS (diffuse alveolar damage) in septic/traumatic shock |
| Adrenals | Cortical cell lipid depletion; Waterhouse-Friderichsen syndrome in DIC |
| GI tract | Hemorrhagic enteropathy; bacterial translocation in irreversible stage |
| Liver | Centrilobular necrosis ("shock liver") |
Fibrin microthrombi are characteristically found in kidney glomeruli in DIC-associated shock.
Clinical Signs of Shock
- Hypotension (systolic BP <90 mmHg or MAP <65 mmHg) - but not always present early
- Tachycardia
- Cool, clammy, pale skin (or warm/flushed in sepsis/distributive)
- Altered mental status (confusion, agitation)
- Oliguria/anuria (urine output <0.5 mL/kg/hr)
- Elevated serum lactate (marker of tissue hypoperfusion)
- Metabolic acidosis
General Principles of Management
- Recognize shock early - high clinical suspicion in any patient with hypotension or new organ dysfunction
- Identify the type - history, exam, hemodynamic monitoring
- Restore oxygen delivery simultaneously with diagnostic workup - do not delay
- Fluid resuscitation with crystalloids (balanced solutions preferred)
- Vasopressors (norepinephrine first-line) if fluids alone cannot maintain MAP ≥65 mmHg
- Treat the underlying cause (antibiotics for sepsis, PCI for cardiogenic, epinephrine for anaphylaxis, surgery for hemorrhage)
- Involve the multidisciplinary team (ICU, surgery, cardiology as needed)
Sources: Robbins, Cotran & Kumar Pathologic Basis of Disease | Robbins & Kumar Basic Pathology | Harrison's Principles of Internal Medicine, 22nd ed.
This is a shared conversation. Sign in to Orris to start your own chat.