Dimentia
Reading File
Finding Sources
Searching PubMed
"dementia"[MeSH Terms] AND diagnosis AND management
Searching the Web
dementia types diagnosis management 2025 guidelines
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Loading Image
Reading File
Loading Image
Here is a thorough overview of dementia, synthesized from multiple authoritative medical textbooks.
Dementia (Neurocognitive Disorder)
Definition
Dementia is a clinical syndrome of persistent intellectual decline severe enough to interfere with social or occupational functioning in an alert individual. The DSM-5 now prefers the term "major neurocognitive disorder", defined as significant cognitive impairment and interference with independence that is not caused by delirium or another primary mental disorder. Key cognitive domains affected include:
-
Complex attention
-
Executive function
-
Learning and memory
-
Language
-
Perceptual-motor ability
-
Social cognition
-
Goldman-Cecil Medicine, p. 3861
Epidemiology
-
5-10% of people over age 65 have dementia; this rises to 30-50% of those over age 85
-
Prevalence roughly doubles every 5 years after age 65
-
Alzheimer disease (AD) accounts for 60-80% of all dementia
-
Dementia reduces life expectancy by approximately half compared to non-demented individuals of the same age
-
Textbook of Family Medicine 9e, p. 1339; Goldman-Cecil Medicine, p. 3862
Types and Their Key Features
The four major disease classes causing dementia, and their approximate prevalence:
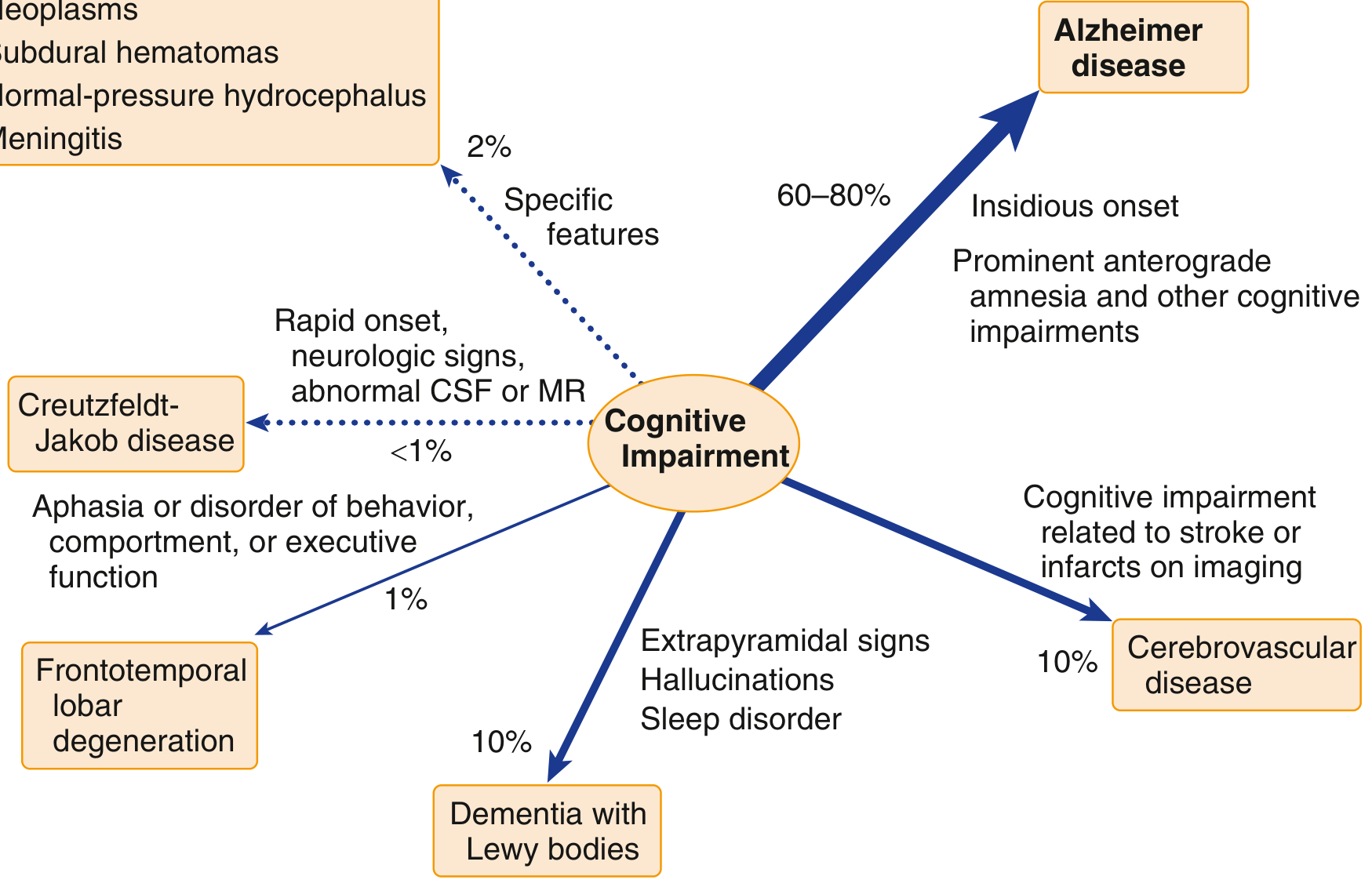
| Type | Prevalence | Key Pathology | Clinical Clues |
|---|---|---|---|
| Alzheimer disease | 60-80% | Beta-amyloid plaques + neurofibrillary tangles (tau) | Insidious onset; anterograde amnesia first; language and visuospatial deficits later |
| Vascular (cerebrovascular) | ~10% | Ischemic neuronal death from hypertension/diabetes | Stepwise decline; stroke history; infarcts on imaging |
| Dementia with Lewy bodies | ~10% | Alpha-synuclein (Lewy body) deposits in cortex | Extrapyramidal signs, visual hallucinations, REM sleep disorder |
| Frontotemporal lobar degeneration | ~1% | Tau and/or TDP-43 abnormalities in frontal/temporal lobes | Aphasia OR behavioral/executive dysfunction; often younger onset |
| Creutzfeldt-Jakob disease | <1% | Prion disease | Rapid onset, myoclonus, abnormal CSF/MRI |
| Secondary causes | ~2% | Reversible (drugs, metabolic, infectious, structural) | Subacute onset; treatable if caught early |
- Goldman-Cecil Medicine, p. 3862; Guyton and Hall Textbook of Medical Physiology
Diagnosis
Step 1 - Establish the syndrome
The key distinction before calling something dementia:
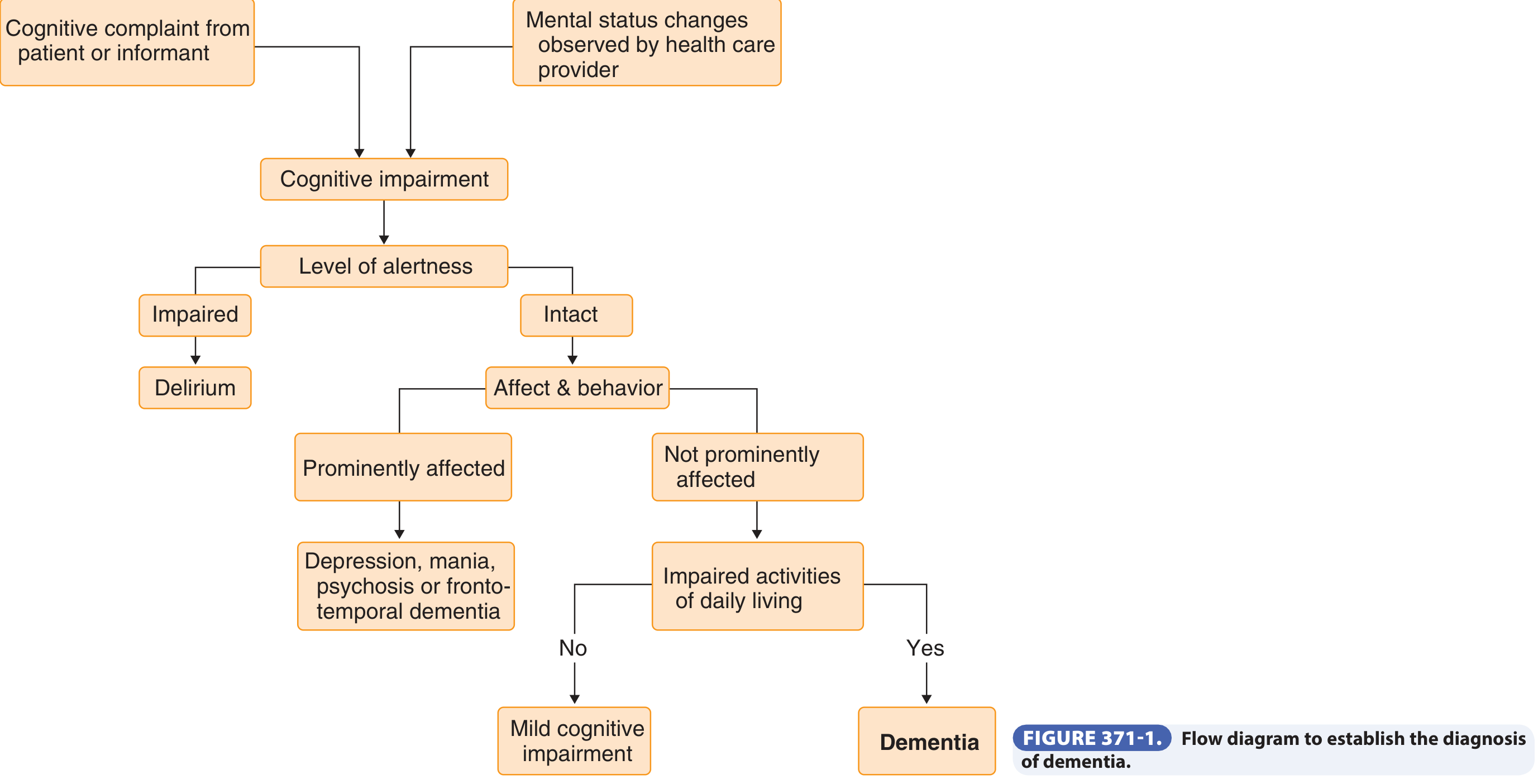
- Delirium - impaired alertness (rules out dementia acutely)
- Depression (pseudodementia) - prominently affected mood/behavior; can mimic dementia; untreated depression independently raises long-term dementia risk
- Mild cognitive impairment (MCI) - impaired IADLs but ADLs intact; 2 SD below norm; significant risk of progression to dementia
- Normal aging (AAMI) - subjective memory concerns but normal on testing
Step 2 - Cognitive testing
- Mini-Cog or MMSE: adequate for moderate-to-severe dementia
- Neuropsychometric testing: required for mild impairment (bedside tests lack sensitivity at the mild end)
- Neurologic exam: look for focal signs (cerebrovascular), extrapyramidal features (Lewy body/Parkinson)
Step 3 - Laboratory workup (rule out reversible causes)
Always exclude:
- Hypothyroidism/hyperthyroidism
- Vitamin B12 deficiency
- Chronic liver/renal failure
- Hypocalcemia/hypercalcemia
- HIV, cryptococcal/TB meningitis, tertiary syphilis
- Sedating drugs (opioids, sedatives, corticosteroids, digoxin)
Step 4 - Neuroimaging
MRI is the modality of choice. Serial coronal MRI in Alzheimer disease demonstrates progressive hippocampal atrophy:
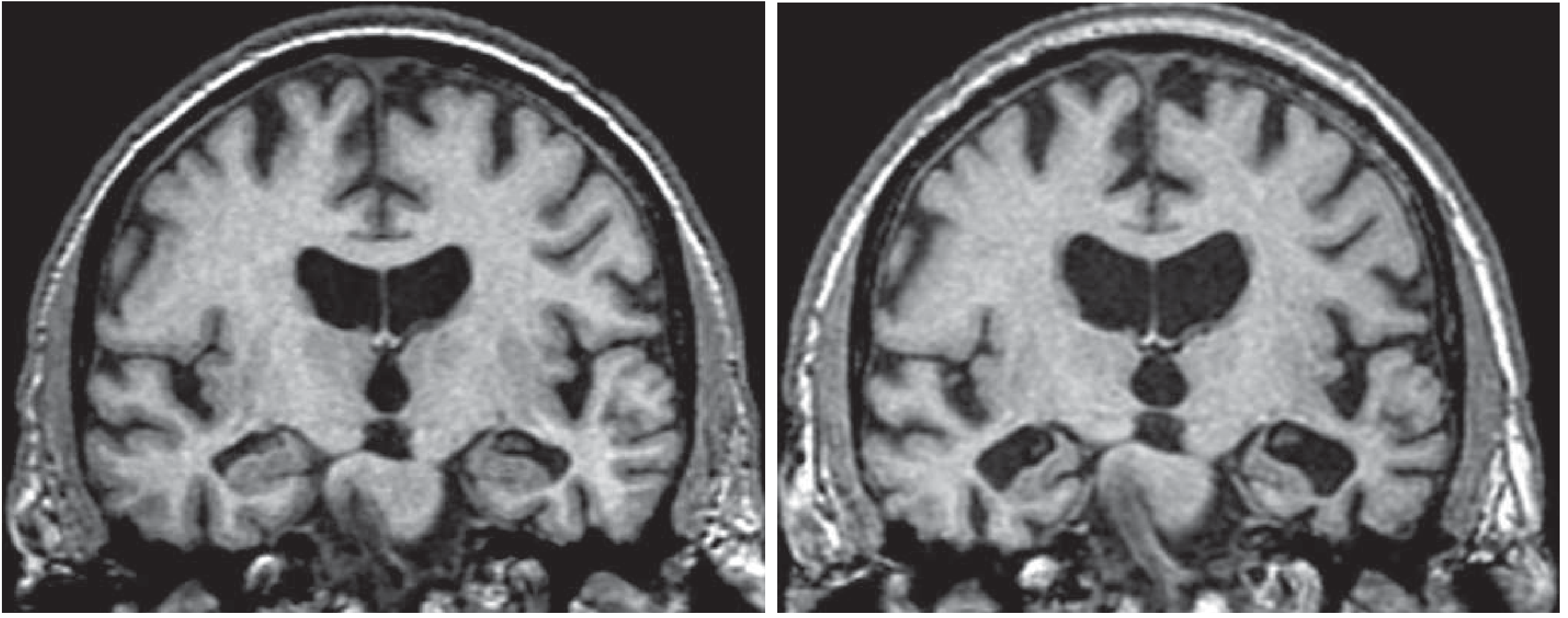
In 2025, the Alzheimer's Association released updated appropriate use criteria recommending blood-based biomarkers and amyloid/tau PET for cognitively impaired individuals as part of the diagnostic workup.
- Goldman-Cecil Medicine, p. 3861-3863
Pathophysiology of Alzheimer Disease (Most Common Type)
-
Beta-amyloidosis begins accumulating in the neocortex up to 20 years before clinical dementia
-
Soluble oligomeric forms of beta-amyloid are the likely key pathogenic molecules
-
Neurofibrillary tangles (hyperphosphorylated tau) spread from medial temporal lobe → association cortices in a predictable pattern; tangle burden closely mirrors clinical severity
-
The most consistent neurotransmitter deficit is cholinergic (nucleus basalis, septum, diagonal band), which is the target for pharmacotherapy
-
Hippocampal atrophy is characteristic and measurable on MRI
-
Goldman-Cecil Medicine, p. 3863-3864
Clinical Stages of Alzheimer Disease
Early:
- Short-term memory difficulty (forgetting names, recent events)
- Depression and apathy common
Middle:
- Disorientation, confusion, impaired judgment
- IADLs then ADLs progressively impaired
Late:
- Difficulty speaking, swallowing
- Failure to recognize loved ones
- Bedridden, requiring total care
Progression from mild to moderate to severe varies among individuals.
- Textbook of Family Medicine 9e, p. 1340
Management
Pharmacologic (Alzheimer Disease)
Symptomatic pharmacotherapy is currently only available for Alzheimer disease dementia. No disease-modifying treatments currently slow or stop neuronal death, though several anti-amyloid agents are under study (lecanemab, donanemab).
| Drug Class | Agents | Indication | Notes |
|---|---|---|---|
| Acetylcholinesterase inhibitors (AChEI) | Donepezil, rivastigmine, galantamine | Mild-to-moderate AD | Modest efficacy; SE: nausea, vomiting, diarrhea, bradyarrhythmia, nightmares, urinary incontinence |
| NMDA receptor antagonist | Memantine | Moderate-to-severe AD | Better SE profile than AChEIs; modest cognitive and QoL benefit |
-
Start AChEIs at low dose, titrate slowly
-
Multiple formulations available (transdermal patch, ODT, liquid) to aid compliance
-
All AChEIs appear equally efficacious
-
Benefit documented at 52 weeks; benefit beyond that is uncertain
-
Textbook of Family Medicine 9e, p. 1340; Goldman-Cecil Medicine, p. 3382
Non-Pharmacologic and General Principles
- Disclose the diagnosis early
- Caregiver education, training, and support groups
- Keep patient mentally active
- Assess functional status and safety (driving, financial management)
- Screen for behavioral/psychiatric symptoms (agitation, wandering)
- Advance care planning - ideally while patient retains capacity
End-Stage/Palliative Care
-
PEG tube feeding is not recommended in advanced dementia - does not reduce aspiration, improve wound healing, or increase survival. Hand feeding and comfort feeding are preferred.
-
Hospice enrollment improves symptom management and reduces unnecessary healthcare utilization
-
Patients with dementia typically die of sepsis, pneumonia, pulmonary embolism, or heart disease - not directly from dementia
-
Bradley and Daroff's Neurology in Clinical Practice; Goldman-Cecil Medicine
Prevention
- Vascular risk factor control (hypertension, diabetes, hyperlipidemia) may lower risk
- Low educational achievement is a consistent risk factor (reduced cognitive reserve)
- A 2025 meta-analysis in Age Ageing found an association between certain vaccinations and reduced dementia risk
- Head injury is a risk factor, primarily through chronic traumatic encephalopathy
Key Clinical Pearls
- Dementia = intact alertness + impaired cognition + functional impairment. If alertness is impaired, think delirium first.
- Always rule out reversible causes before concluding the dementia is degenerative.
- MCI is not dementia - IADLs may be impaired but ADLs are preserved. Close monitoring for progression is warranted.
- "Pseudodementia" (depression mimicking dementia) must be actively excluded; treat depression and reassess cognition.
- Mixed pathology is common at autopsy - pure syndromes are relatively less frequent.
Sources: Goldman-Cecil Medicine International Edition (2-Vol Set), Textbook of Family Medicine 9e, Guyton and Hall Textbook of Medical Physiology, Bradley and Daroff's Neurology in Clinical Practice
Purulent meningitis:
Reading File
Finding Sources
Finding Sources
Searching PubMed
"bacterial meningitis"[MeSH Terms] AND treatment
Searching the Web
purulent bacterial meningitis pathophysiology diagnosis treatment 2025
Reading File
Reading File
Searching PubMed
"bacterial meningitis"[MeSH Terms] AND dexamethasone
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
I now have comprehensive content from multiple authoritative sources. Let me compile the full response.
Purulent (Bacterial) Meningitis
Definition
Purulent meningitis - also called pyogenic or bacterial meningitis - is an acute inflammation of the arachnoid membrane, pia mater, and the intervening CSF. The inflammatory process extends throughout the subarachnoid space around the brain and spinal cord and involves the ventricles. It is distinguished from aseptic/viral meningitis by its characteristic polymorphonuclear (neutrophilic) CSF pleocytosis.
- Goldman-Cecil Medicine, p. 3997
Epidemiology
-
Incidence in developed countries: 0.5-1.5 cases per 100,000 adults - dramatically reduced by vaccination
-
Despite vaccine-related decline in incidence, mortality (~15%) has not changed
-
Since the Haemophilus vaccine, S. pneumoniae now accounts for ~70% of cases and the disease predominantly affects older adults
-
Worldwide, incidence is related to poverty and remains a major cause of morbidity and mortality
-
Goldman-Cecil Medicine, p. 3999
Causative Organisms (Age-Based)
| Age Group | Common Pathogens |
|---|---|
| < 1 month | Group B Streptococcus, E. coli, Listeria monocytogenes, Klebsiella spp. |
| 1-23 months | S. pneumoniae, N. meningitidis, Group B Strep, H. influenzae, E. coli |
| 3 months - 18 years | S. pneumoniae, N. meningitidis, H. influenzae |
| 18-50 years | N. meningitidis, S. pneumoniae |
| > 50 years | S. pneumoniae, L. monocytogenes, aerobic gram-negative bacilli |
| Post-neurosurgery / CSF shunt | Coagulase-negative Staphylococci, S. aureus, Pseudomonas aeruginosa |
| Basilar skull fracture | S. pneumoniae, H. influenzae, Group A beta-hemolytic Strep |
Meningococcal disease (N. meningitidis) is most common in younger individuals living in close proximity (military barracks, college dormitories). Groups A, B, C are the major serogroups.
- Textbook of Family Medicine 9e, p. 1232; Rosen's Emergency Medicine
Pathophysiology
The infection typically follows this sequence:
- Nasopharyngeal colonization - bacteria colonize and invade the mucosa; capsular properties protect them from phagocytosis
- Blood-brain barrier crossing - once in CSF, local host defenses (complement, immunoglobulins) are ineffective
- Bacterial proliferation in CSF - triggers leukocyte recruitment
- Inflammatory cascade - cytokine release into CSF promotes:
- Increased blood-brain barrier permeability
- Cerebral vasculitis
- Cerebral edema
- Raised intracranial pressure (ICP)
- Reduced cerebral blood flow - leading to cerebral hypoxia and neuronal injury
- Rosen's Emergency Medicine, p. 2268
Clinical Features
Classic triad (present in ~85% of adults):
- Fever
- Headache
- Neck stiffness (nuchal rigidity)
Additional symptoms:
- Nausea and vomiting (35%)
- Seizures (30%)
- Cranial nerve palsies, focal neurologic signs (10-20%)
- Meningismus (50%) - assessed by:
- Kernig's sign: resistance to knee extension after hip and knee flexion
- Brudzinski's sign: involuntary knee flexion in response to rapid neck flexion
- Photophobia, confusion, lethargy, sweats, rigors
- Petechial/purpuric rash starting as maculopapular on extremities - strongly suggests meningococcal meningitis
- Papilledema: <1% early; if present, consider brain abscess or mass
Age-specific presentations:
-
Neonates: poor feeding, irritability, vomiting, temperature instability, apnea; nuchal rigidity unreliable; bulging fontanelle (late); seizures in 40%
-
Elderly: insidious presentation, variable meningeal signs, altered mental status, possible absence of fever
-
Textbook of Family Medicine 9e, p. 1232
Predisposing Factors
- Otitis media (most common)
- Sinusitis, mastoiditis
- Closed-head trauma with CSF leak
- Neurosurgery, penetrating trauma
- Immunocompromise, asplenia
- Alcoholism, burns
- Age extremes (neonate, elderly)
Diagnosis
When to do CT before LP
Obtain CT first if any of the following are present:
| Criterion | Notes |
|---|---|
| Immunocompromised state | HIV/AIDS, transplant, immunosuppressive therapy |
| History of CNS disease | Mass lesion, stroke, focal infection |
| New-onset seizure | Within 1 week of presentation |
| Papilledema | Venous pulsations suggest absence of raised ICP |
| Abnormal level of consciousness | - |
| Focal neurologic deficit | Dilated pupil, gaze palsy, arm/leg drift |
If CT is needed before LP, draw blood cultures and start antibiotics + dexamethasone immediately - do not delay treatment for imaging.
CSF Findings - Bacterial vs. Viral Meningitis
| Parameter | Bacterial Meningitis | Viral Meningitis |
|---|---|---|
| Opening pressure (mm H2O) | >180 | Often normal or elevated |
| Leukocyte count (cells/mm3) | 1,000-10,000 (median 1,195; range 100-20,000) | <300 (median 100) |
| Neutrophils (%) | >80% | <20% |
| Glucose (mg/dL) | <45 (or CSF:serum <0.4) | Normal (>45) |
| Protein (mg/dL) | >50 | Normal or mildly elevated |
| Gram stain | Positive in 60-90% (specificity >97%) | Negative |
Other Diagnostic Tests
-
Gram stain: first-line rapid test; sensitivity 60-90% in community-acquired cases
-
Culture: gold standard; sensitivity reduced if antibiotics given first
-
PCR: helpful when Gram stain is negative (especially for meningococcus)
-
Blood cultures: always draw before antibiotics
-
Serum CRP: helpful when Gram stain is equivocal
-
Low-risk criteria (Bacterial Meningitis Score): negative Gram stain + CSF ANC <1,000 + CSF protein <80 mg/dL + peripheral ANC <10,000 cells/mL = very low risk for bacterial meningitis
-
Textbook of Family Medicine 9e, p. 1232-1233; Adams and Victor's Principles of Neurology
Treatment
Empiric Antibiotic Therapy (by age/setting)
| Setting | First-Line Empiric Therapy |
|---|---|
| < 1 month | Ampicillin + cefotaxime OR ampicillin + aminoglycoside |
| 1-23 months | Vancomycin + 3rd-gen cephalosporin (ceftriaxone/cefotaxime) |
| 2-50 years | Vancomycin + 3rd-gen cephalosporin |
| > 50 years | Vancomycin + ampicillin + 3rd-gen cephalosporin |
| Basilar skull fracture | Vancomycin + 3rd-gen cephalosporin |
| Post-neurosurgery/penetrating trauma | Vancomycin + cefepime OR ceftazidime OR meropenem |
| CSF shunt | Vancomycin + cefepime OR ceftazidime OR meropenem |
Pathogen-Directed Therapy
| Organism | Standard Therapy | Alternatives |
|---|---|---|
| S. pneumoniae (pen-sensitive, MIC <0.1) | Penicillin G or ampicillin | 3rd-gen cephalosporin, chloramphenicol |
| S. pneumoniae (pen-resistant, MIC ≥2.0) | Vancomycin + 3rd-gen cephalosporin | Moxifloxacin |
| N. meningitidis | 3rd-gen cephalosporin | Penicillin G, ampicillin |
| L. monocytogenes | Ampicillin (± aminoglycoside) | TMP-SMX |
| H. influenzae | 3rd-gen cephalosporin | Cefepime, chloramphenicol |
Adjunctive Dexamethasone
Goal: minimize meningeal inflammation to reduce brain injury and hearing loss.
-
Adults: 0.15 mg/kg IV every 6 hours x 2-4 days, given 10-20 minutes BEFORE (or at least concomitant with) the first dose of antibiotic
- Strongly indicated for suspected/proven pneumococcal meningitis
- Many experts give it to all adults since etiology is initially unknown
- Do NOT give if antibiotics have already been started (no benefit)
- Continue only if CSF shows gram-positive diplococci or cultures positive for S. pneumoniae
-
Infants and children with Hib meningitis: 0.15 mg/kg q6h x 2-4 days, before first antibiotic dose
- Beneficial for H. influenzae meningitis
- Controversial for pneumococcal meningitis in children (insufficient evidence)
- Not recommended for neonates (insufficient data)
-
Textbook of Family Medicine 9e, p. 1234
Duration of Therapy
Duration is based more on tradition than clinical evidence; varies by pathogen (typically 7-14 days). Repeat LP is not necessary for patients who demonstrate clinical improvement within 24-48 hours.
Prophylaxis
Rifampin chemoprophylaxis - indicated for close contacts of documented meningococcal or Hib meningitis:
- Adults: 600 mg orally twice daily x 2 days
- Children >1 month: 10 mg/kg (max 600 mg) every 12 hours x 2 days
- Children <1 month: 5 mg/kg every 12 hours x 2 days
- Pregnant women: rifampin contraindicated; use ceftriaxone IM as single dose (125 mg if ≤15 years, 250 mg if >15 years)
Vaccines: Hib, pneumococcal (PCV/PPSV23), and meningococcal vaccines (MCV4 for serogroups A/C/Y/W-135; separate vaccine for serogroup B) are the cornerstone of prevention.
- Textbook of Family Medicine 9e, p. 1235
Complications and Prognosis
Mortality
| Organism | Mortality |
|---|---|
| Untreated | Near 100% |
| H. influenzae (treated) | ~5% |
| N. meningitidis (treated) | ~5% |
| S. pneumoniae (treated) | ~15% (higher due to older/sicker population) |
| L. monocytogenes | Up to 27% |
| Neonatal meningitis | 40-75% |
| Waterhouse-Friderichsen syndrome (meningococcemia + adrenal hemorrhage) | Very high |
Poor prognostic factors: bacteremia, coma, seizures, alcoholism, diabetes, multiple myeloma, head trauma, and the "Osler triad" (pneumococcal meningitis + pneumonia + endocarditis).
Neurologic Sequelae
-
Sensorineural hearing loss: occurs early (within 1 day of onset); caused by suppurative cochlear destruction via the cochlear aqueduct
- Pneumococcal: 31% persistent hearing loss
- Meningococcal: 10.5%
- H. influenzae: 6%
-
Hydrocephalus: infrequent complication
-
Cerebral venous/arterial thrombosis: almost one-third of adults with pneumococcal meningitis
-
Seizures: up to 30% during illness; late seizures in some survivors
-
Residual neurologic deficits (motor, cognitive, language): up to 30% with pneumococcal meningitis, 25% with H. influenzae
-
Cranial nerve palsies (other than deafness) typically resolve over weeks to months
-
Adams and Victor's Principles of Neurology, p. 717; Rosen's Emergency Medicine, p. 2268
Key Clinical Pearls
- Do not delay antibiotics waiting for CT or LP - draw blood cultures, then start vancomycin + 3rd-gen cephalosporin ± ampicillin immediately if there are indications for CT first
- Dexamethasone must be given before or with the first antibiotic dose to be effective - it is useless if given after
- A petechial/purpuric rash = meningococcemia until proven otherwise - a medical emergency
- Neonates and elderly may have atypical presentations without the classic triad
- Rifampin may reduce the efficacy of oral contraceptives - counsel contacts accordingly
- Pre-treatment with antibiotics reduces Gram stain and culture yield but does not significantly affect CSF cell counts or protein
Sources: Goldman-Cecil Medicine International Edition; Textbook of Family Medicine 9e; Rosen's Emergency Medicine; Adams and Victor's Principles of Neurology 12th Ed; Henry's Clinical Diagnosis and Management by Laboratory Methods
This is a shared conversation. Sign in to Orris to start your own chat.