I have everything needed for a thorough, well-illustrated answer. Here is the complete structured response:
a) Probable Diagnosis: Chronic Myeloid Leukemia (CML) - Chronic Phase
Clinical Reasoning:
| Feature in this patient | Significance |
|---|
| 50-year-old male | Peak incidence is 5th-6th decade |
| Dragging sensation in abdomen | Classic symptom of massive splenomegaly in CML |
| Massive splenomegaly, no lymphadenopathy | Distinguishes CML from lymphoproliferative disorders (CLL, lymphoma) |
| TLC = 1,60,000/mm³ | Profound leukocytosis - typical of CML chronic phase |
| Platelets = 2 Lakhs/mm³ (normal-elevated) | Thrombocytosis or normal platelets - characteristic of CML; contrast with acute leukemia where platelets fall |
| Pallor | Mild-to-moderate anemia from marrow infiltration |
CML is a myeloproliferative neoplasm (MPN) arising from a pluripotent hematopoietic stem cell (HSC). Because BCR-ABL drives proliferation but does not block differentiation, mature granulocytes accumulate in blood rather than blasts - explaining the clinical picture of extreme leukocytosis with a functioning-appearing smear.
"Sometimes the first symptom is a dragging sensation in the abdomen caused by splenomegaly... The onset is insidious. Mild-to-moderate anemia and hypermetabolism due to increased cell turnover lead to fatigability, weakness, weight loss, and anorexia." - Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 583
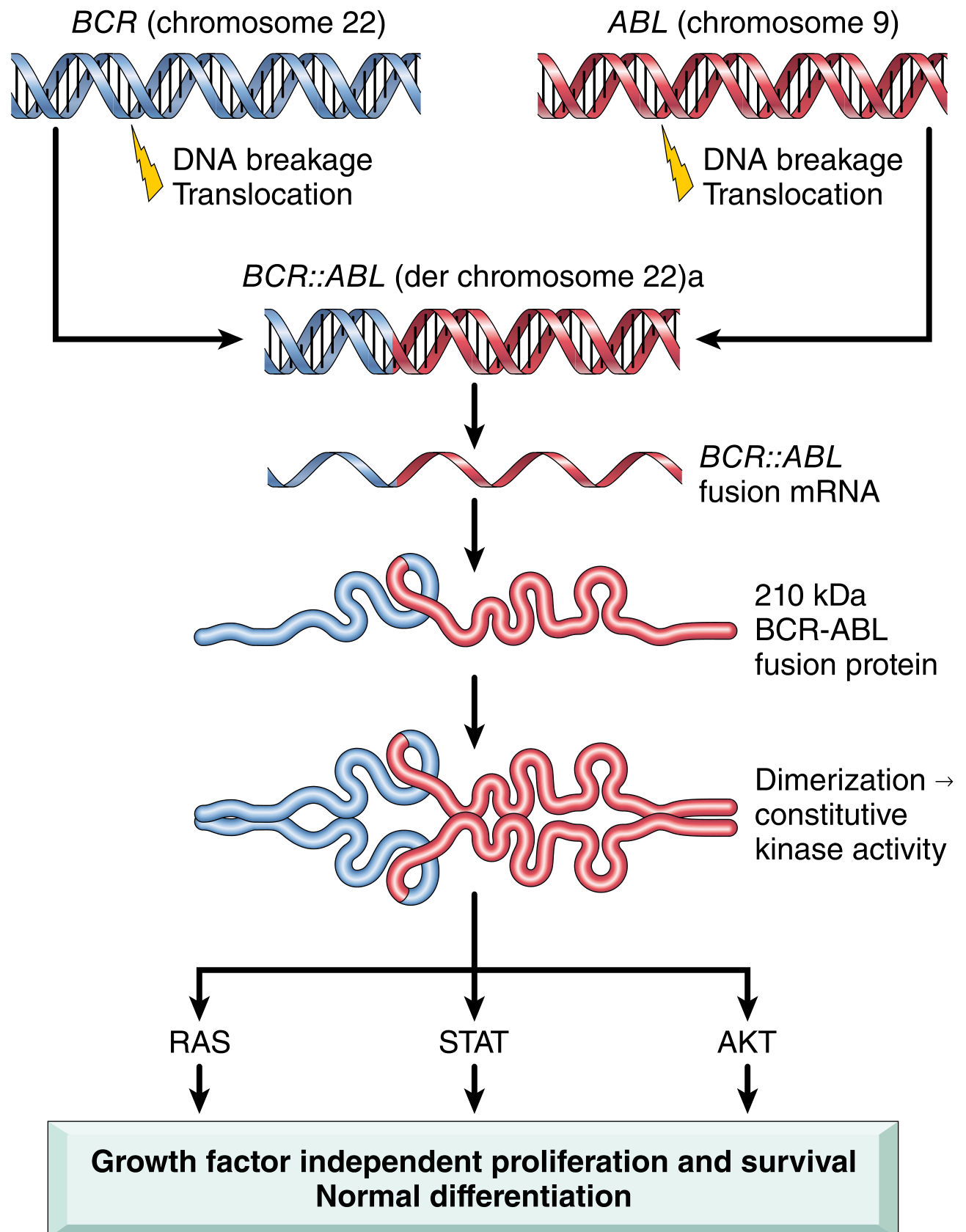
b) Cytogenetic Change: The Philadelphia (Ph) Chromosome
Fig. 13.34 - Robbins Pathology: Pathogenesis of CML - BCR::ABL fusion gene formation and downstream signaling
The Translocation: t(9;22)(q34;q11)
This is a reciprocal translocation between chromosomes 9 and 22:
Chromosome 9 (q34): ABL proto-oncogene (Abelson tyrosine kinase)
+
Chromosome 22 (q11): BCR gene (Breakpoint Cluster Region)
↓
BCR::ABL fusion gene on the shortened derivative chromosome 22
= Philadelphia (Ph) chromosome
Key Details:
| Feature | Detail |
|---|
| Translocation notation | t(9;22)(q34;q11) |
| Genes fused | BCR (chr 22q11) + ABL (chr 9q34) |
| Result | Shortened chromosome 22 = Philadelphia (Ph) chromosome |
| Elongated chromosome 9 | Contains ABL sequences lost from chr 9 (der(9)) |
| Fusion protein | 210 kDa BCR-ABL tyrosine kinase (p210) |
| Mechanism | BCR dimerization domain self-associates → constitutive ABL kinase activation |
| Downstream pathways | RAS, STAT, AKT → growth factor-independent proliferation + survival, with preserved differentiation |
| Frequency | >90-95% of CML cases by conventional karyotype |
Why the Protein is Oncogenic:
Normal ABL kinase is tightly regulated and transiently activated. The BCR moiety provides a dimerization domain causing BCR-ABL to self-associate constitutively, producing a kinase that fires continuously - driving unregulated expansion of myeloid progenitors without arresting maturation.
In the ~5-10% Ph-negative cases:
BCR::ABL fusion still exists but requires FISH or PCR for detection (complex/cryptic rearrangements). There is no true BCR-ABL-negative CML.
Additional cytogenetic abnormalities (disease progression signals):
- Trisomy 8 (+8)
- Isochromosome 17q [i(17q)]
- Duplication of Ph chromosome (+Ph)
- These emerge in the accelerated/blast phase
"In more than 90% of cases, BCR::ABL is created by a reciprocal (9;22)(q34;q11) translocation (the so-called Philadelphia chromosome). The cell of origin is a pluripotent HSC." - Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 583
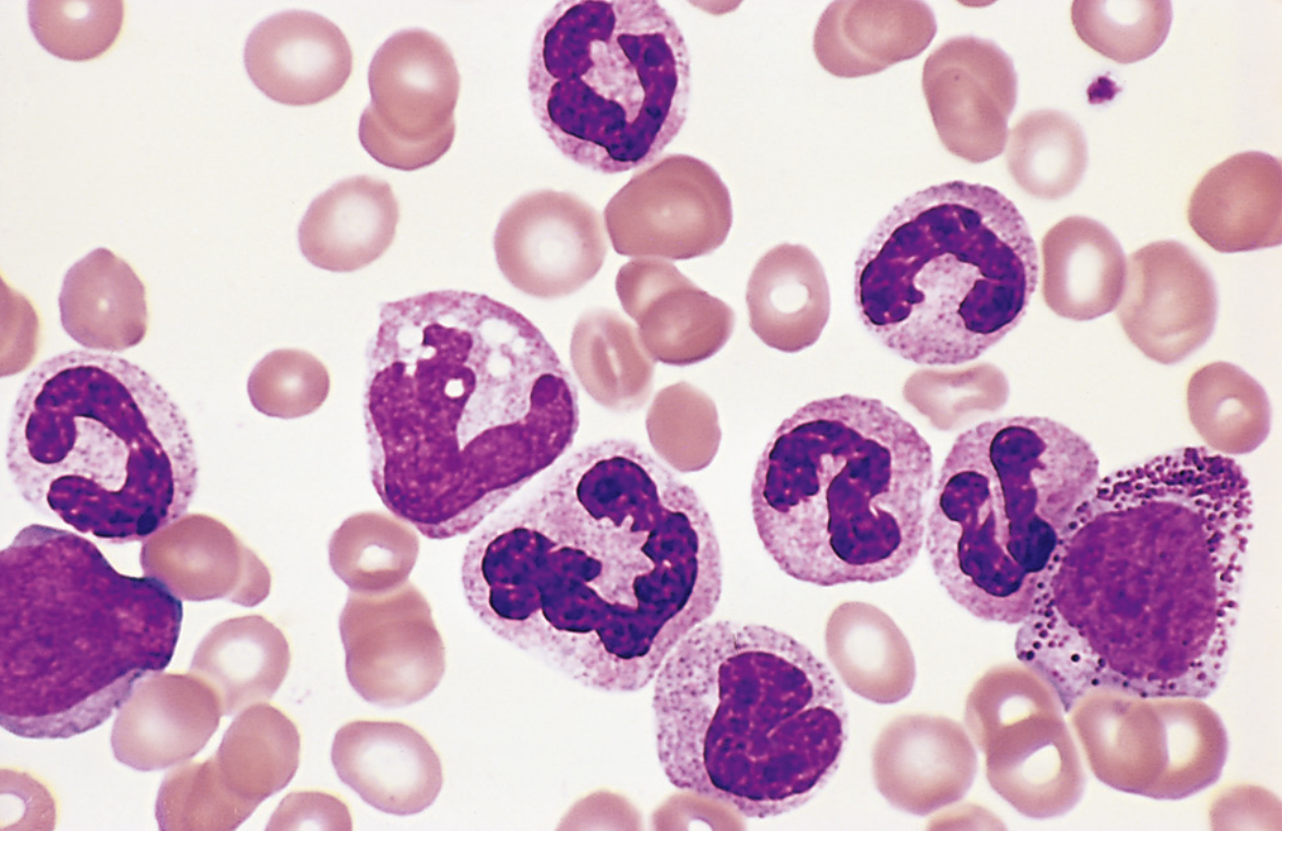
c) Peripheral Blood Smear Findings in CML
Fig. 13.35 - Robbins Pathology: CML peripheral blood smear - mature neutrophils, metamyelocytes, and myelocytes (Dr. Robert W. McKenna, UT Southwestern)
Enumerated Findings:
1. Marked Leukocytosis
- WBC typically 1,00,000-4,00,000/mm³ at presentation
- Composed overwhelmingly of granulocytes at all maturation stages
2. "Myelocyte Bulge" (Myelocyte Peak) - PATHOGNOMONIC
The entire granulocytic maturation series is present on the smear in a spectrum:
| Stage | Proportion |
|---|
| Myeloblasts | <2% (chronic phase) |
| Promyelocytes | Few |
| Myelocytes | Prominent - the "bulge" |
| Metamyelocytes | Present |
| Band forms (stabs) | Present |
| Segmented neutrophils | Predominant (most numerous) |
This "left shift to myelocyte level" with a predominance of mature forms (not blasts) is the hallmark of CML chronic phase.
3. Absolute Basophilia
- Increased basophils - a very characteristic and diagnostically important feature
- Rising basophilia signals progression to accelerated phase
4. Absolute Eosinophilia
- Mild-to-moderate increase in eosinophils
5. Thrombocytosis or Normal Platelets
- Platelets often elevated (as in this case - 2 Lakhs/mm³)
- Large, abnormal platelet morphology may be seen
- Thrombocytopenia in late/accelerated phase signals disease progression
6. Normochromic, Normocytic Anemia
- Mild-to-moderate; reflects marrow replacement and splenic sequestration
7. Occasional Nucleated Red Blood Cells (NRBCs)
- Leukoerythroblastic picture in some cases
8. Low/Absent Leukocyte Alkaline Phosphatase (LAP) Score
- CML neutrophils have markedly reduced LAP (score 0-10; normal 20-100)
- This is the key cytochemical distinction from a leukemoid reaction (which has very high LAP)
9. No Significant Monocytosis or Lymphocytosis
- Distinguishes from CMML (high monocytes) and CLL (lymphocytes)
10. Absence of Toxic Granulation and Döhle Bodies
- These reactive features seen in infective leukocytosis are absent, reflecting a neoplastic rather than reactive process
Summary: CML vs. Leukemoid Reaction
| Feature | CML | Leukemoid Reaction |
|---|
| LAP score | Low/absent | Very high |
| Basophilia | Present | Absent |
| Eosinophilia | Present | Variable |
| Splenomegaly | Massive | Mild |
| Philadelphia chromosome | Present | Absent |
| Blasts on smear | <2% | Absent |
| Toxic granulation | Absent | Present |
Sources: Robbins, Cotran & Kumar - Pathologic Basis of Disease (10th ed.), pp. 582-585 | Goldman-Cecil Medicine, Chapter: Chronic Myeloid Leukemia | Harrison's Principles of Internal Medicine 22E