Beta blockers for angina
"beta blockers" AND "stable angina"
Beta Blockers for Angina
Mechanism of Action
- Increases diastolic filling time (improving coronary perfusion)
- Reduces the rate-pressure product (a key determinant of myocardial O2 demand)
Available Agents and Doses (for Angina)
| Drug | Selectivity | Partial Agonist Activity | Usual Dose for Angina |
|---|---|---|---|
| Atenolol | β₁ | No | 50-200 mg/day |
| Metoprolol | β₁ | No | 50-200 mg twice daily |
| Bisoprolol | β₁ | No | 10 mg/day |
| Betaxolol | β₁ | No | 10-20 mg/day |
| Nebivolol | β₁ (low doses) | No | 5-40 mg/day |
| Acebutolol | β₁ | Yes | 200-600 mg twice daily |
| Propranolol | Non-selective | No | 80-120 mg twice daily |
| Nadolol | Non-selective | No | 40-80 mg/day |
| Timolol | Non-selective | No | 10 mg twice daily |
| Pindolol | Non-selective | Yes | 2.5-7.5 mg three times daily |
| Labetalol (alpha+beta) | None | Yes | 200-600 mg twice daily |
| Esmolol (IV only) | β₁ | No | 50-300 mcg/kg/min |
Clinical Use
- Stable angina as monotherapy or in combination with nitrates
- Post-MI patients with angina - beta blockers improve life expectancy after MI, calcium channel blockers do not
- Angina with concurrent hypertension or tachyarrhythmias
- Angina with LV dysfunction (use carvedilol or bisoprolol)
Contraindications and Adverse Effects
- Bronchial asthma or reversible airway obstruction (even β₁-selective agents can worsen asthma at higher doses)
- Significant AV conduction disturbances or sick-sinus syndrome
- Severe bradycardia
- Raynaud's phenomenon / severe peripheral arterial disease
- Decompensated heart failure (acute)
- History of mental depression
- Fatigue, reduced exercise tolerance, nightmares, impotence
- Cold extremities, worsening intermittent claudication
- Bradycardia, AV block, LV failure
- Potentiation of hypoglycemia from oral hypoglycemic agents/insulin (masks hypoglycemic symptoms)
- Bronchospasm
Special Situations
- Vasospastic (Prinzmetal's) angina: Beta blockers are generally avoided - they can worsen coronary vasospasm by leaving alpha-adrenergic vasoconstriction unopposed. Calcium channel blockers (especially dihydropyridines) are the drug of choice here.
- Nocturnal angina: IV esmolol trial can assess safety of beta blockade in borderline patients. Nocturnal angina may often respond to a long-acting CCB.
- Angina + asthma/COPD: Use a β₁-selective agent (metoprolol, atenolol) at the lowest effective dose, with careful monitoring.
- Angina + diabetes: β₁-selective agents preferred; note they can mask hypoglycemic symptoms.
Place in Therapy
Give answer in flowchart
A clean medical flowchart titled "Beta Blockers for Angina" with the following structure and flow: START box: "Patient with Angina" Arrow down to diamond decision box: "Type of Angina?" Two branches: - Left branch: "Stable (Effort) Angina" - Right branch: "Vasospastic (Prinzmetal's) Angina" → box: "AVOID Beta Blockers → Use Calcium Channel Blockers (Dihydropyridines)" From "Stable Angina" arrow down to box: "MECHANISM OF BETA BLOCKERS • Block β-adrenergic receptors • ↓ Heart rate, contractility, BP • ↓ Myocardial O₂ demand • ↑ Diastolic perfusion time" Arrow down to diamond: "Contraindications present?" Left (YES) branch: box "CONTRAINDICATIONS • Bronchial asthma / COPD • AV block / sick sinus syndrome • Severe bradycardia • Decompensated heart failure • Severe peripheral arterial disease → Use Calcium Channel Blockers instead" Right (NO) branch: box "INITIATE BETA BLOCKER THERAPY Target HR: 55–60 bpm at rest Max exercise HR: <100 bpm" Arrow down to box: "DRUG SELECTION β₁-Selective (Preferred): • Metoprolol 50–200 mg twice daily • Atenolol 50–200 mg/day • Bisoprolol 10 mg/day • Betaxolol 10–20 mg/day Non-Selective: • Propranolol 80–120 mg twice daily • Nadolol 40–80 mg/day" Arrow down to diamond: "Adequate symptom control?" YES branch → box: "CONTINUE THERAPY Monitor HR, BP, symptoms Taper slowly if stopping (over 2 weeks) Never abruptly discontinue" NO branch → box: "ADD COMBINATION THERAPY • + Amlodipine (dihydropyridine CCB) ✓ Safe • + Diltiazem (if normal EF, no AV block) ✓ • + Long-acting nitrates ✓ • AVOID: Verapamil + BB (↑ bradycardia risk) • Consider Ranolazine for refractory angina" Arrow from combination therapy box → "Continue Therapy" box Side note box on the right: "SPECIAL POPULATIONS Post-MI: BB improve survival ✓ Angina + HF: Use Carvedilol / Bisoprolol Angina + Diabetes: Use β₁-selective (masks hypoglycemia) Nocturnal angina: Consider IV Esmolol trial ADVERSE EFFECTS • Fatigue, cold extremities • Bradycardia, AV block • Impotence, nightmares • Worsened claudication" Use a professional medical style with blue and white color scheme, clear arrows showing flow direction, rounded boxes for processes, diamond shapes for decisions, and red highlight for contraindications/avoid boxes.
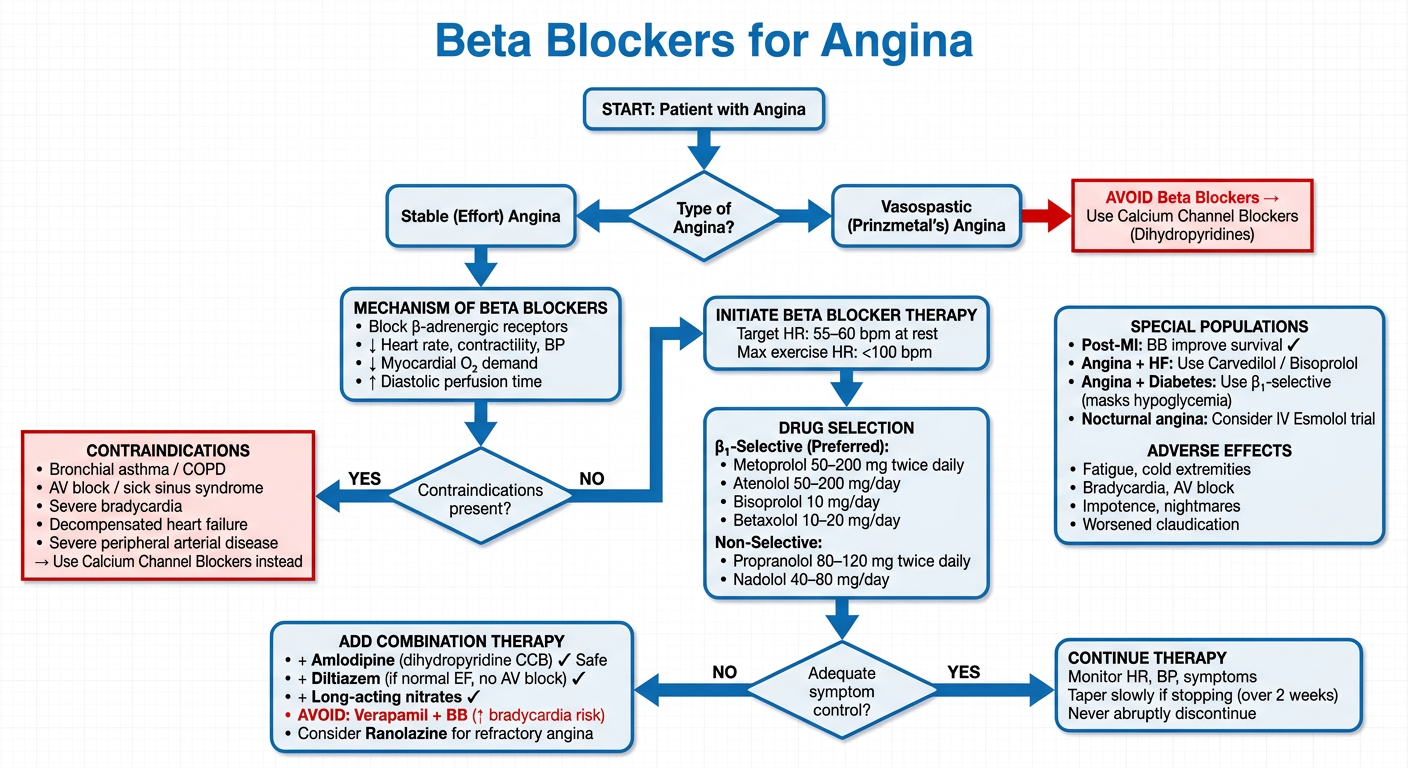
- Angina type - Vasospastic vs. Stable (key branch point, as beta blockers are avoided in Prinzmetal's)
- Mechanism - how beta blockers reduce O₂ demand
- Contraindication screening - before initiating therapy
- Drug selection - β₁-selective agents preferred, with specific doses
- Titration goal - resting HR 55-60 bpm
- Combination therapy - when monotherapy fails (including what to avoid - verapamil + BB)
- Special populations - post-MI, HF, diabetes, nocturnal angina
- Adverse effects and safe discontinuation (always taper over 2 weeks)