Tkr approach
Tkr all approaches step by step with images and flow chart for pg exam 10 marks
TKR total knee replacement surgical approaches medial parapatellar subvastus midvastus step by step
https://www.orthonebraska.com/resources/total-knee-replaceme…
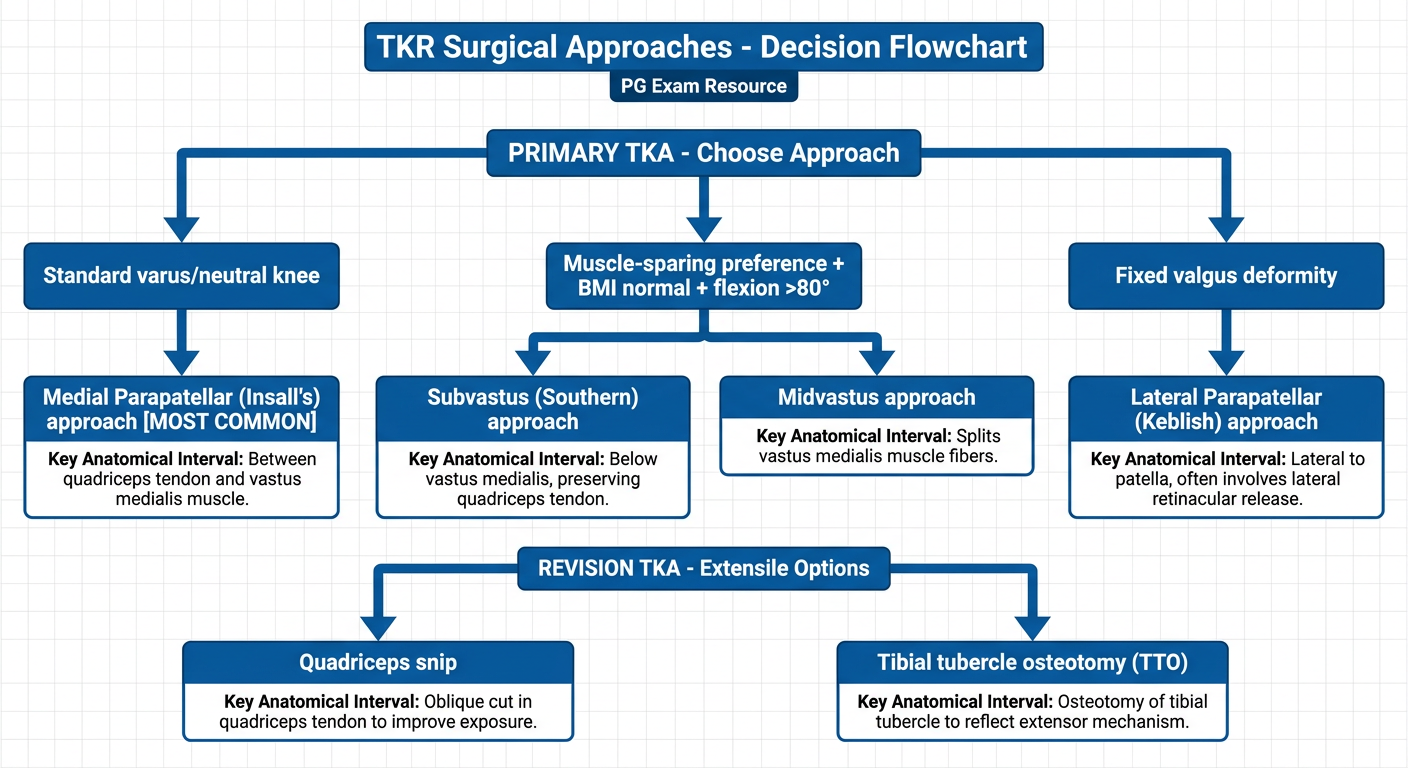
A clean medical educational flowchart titled "TKR Surgical Approaches - Decision Flowchart" for PG exam. The flowchart starts at the top with "PRIMARY TKA - Choose Approach" then branches into: 1) Standard varus/neutral knee → Medial Parapatellar (Insall's) approach [MOST COMMON], 2) Muscle-sparing preference + BMI normal + flexion >80° → Subvastus (Southern) approach OR Midvastus approach, 3) Fixed valgus deformity → Lateral Parapatellar (Keblish) approach. For revision TKA, show extensile options: Quadriceps snip and Tibial tubercle osteotomy (TTO). Each approach box should have a brief note about the key anatomical interval. Use blue and white color scheme with clear arrows and bold labels. Clean academic style.
Total Knee Replacement (TKR) - Surgical Approaches
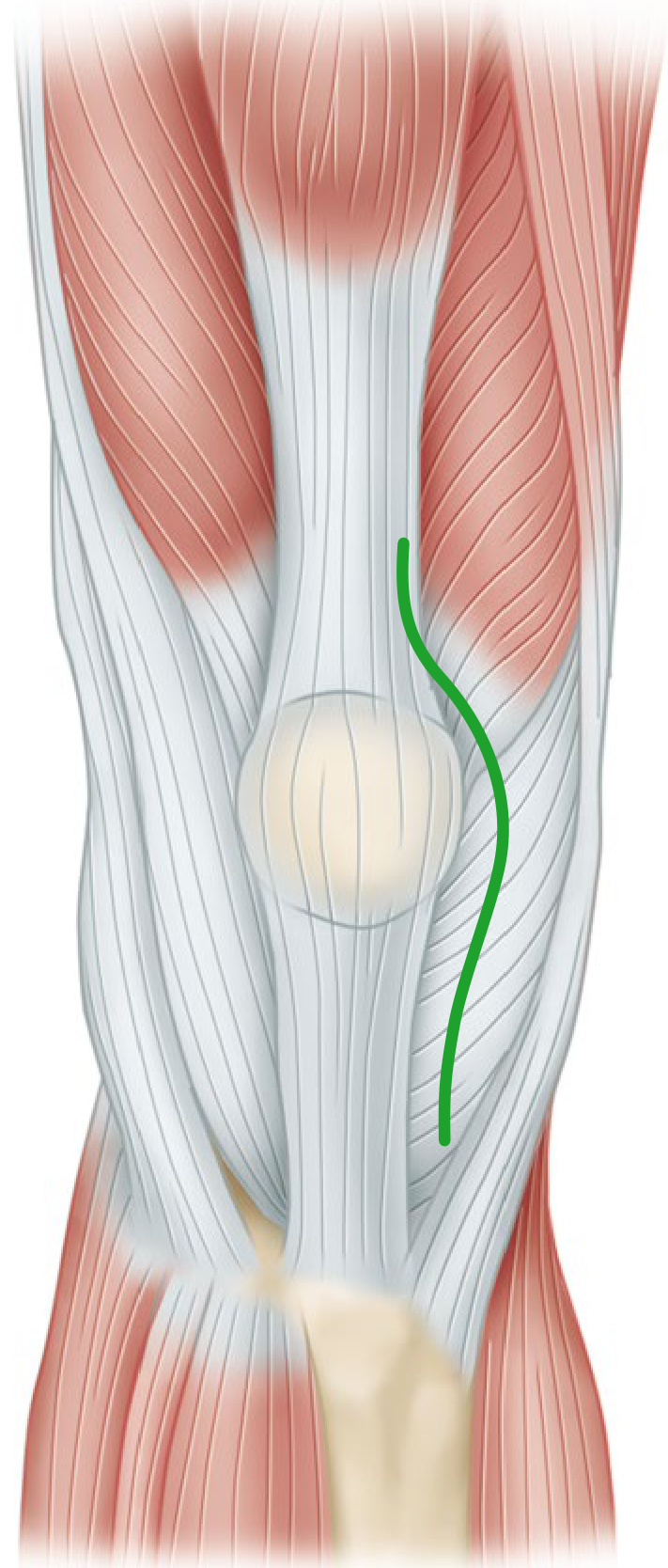
OVERVIEW - Skin Incision (Common to All Approaches)
Key point: If multiple prior scars exist, use the most lateral usable scar - blood supply to anterior knee skin comes predominantly from the medial side.
DECISION FLOWCHART
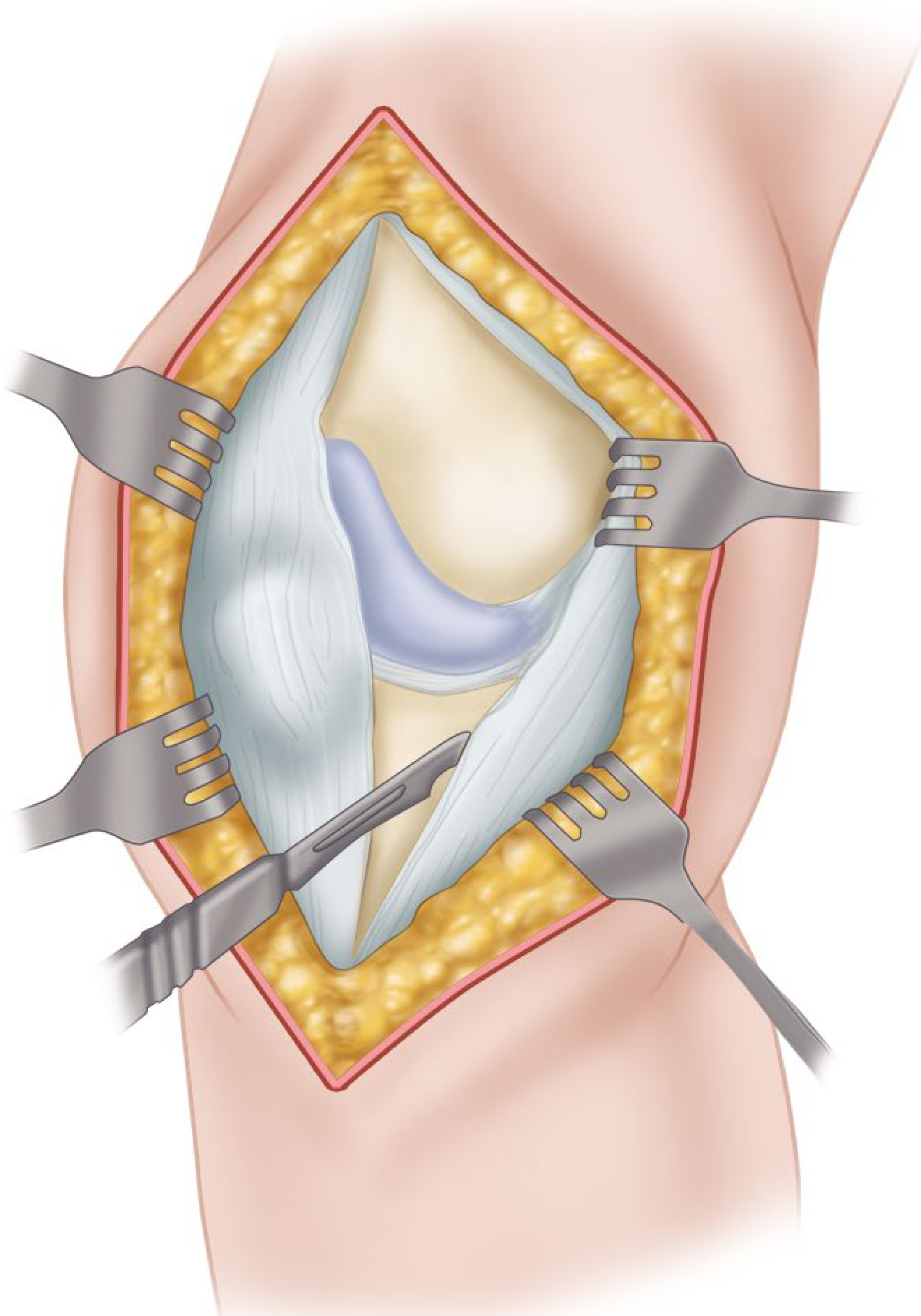
APPROACH 1: MEDIAL PARAPATELLAR (Insall's Approach)
Standard / Most Commonly Used - Gold Standard
Step-by-Step Technique (Campbell's Technique 8.1):
| Step | Action |
|---|---|
| 1 | Anterior midline skin incision with knee in flexion |
| 2 | Create full-thickness medial and lateral skin flaps - keep dissection just superficial to extensor mechanism |
| 3 | Retinacular incision: Medial parapatellar incision, leaving a 3-4 mm cuff of tendon on vastus medialis for closure |
| 4 | Extend incision proximally along quadriceps tendon length; distally 3-4 cm onto anteromedial tibial surface along medial border of patellar tendon |
| 5 | Subperiosteally elevate anteromedial capsule and deep MCL off tibia to posteromedial corner |
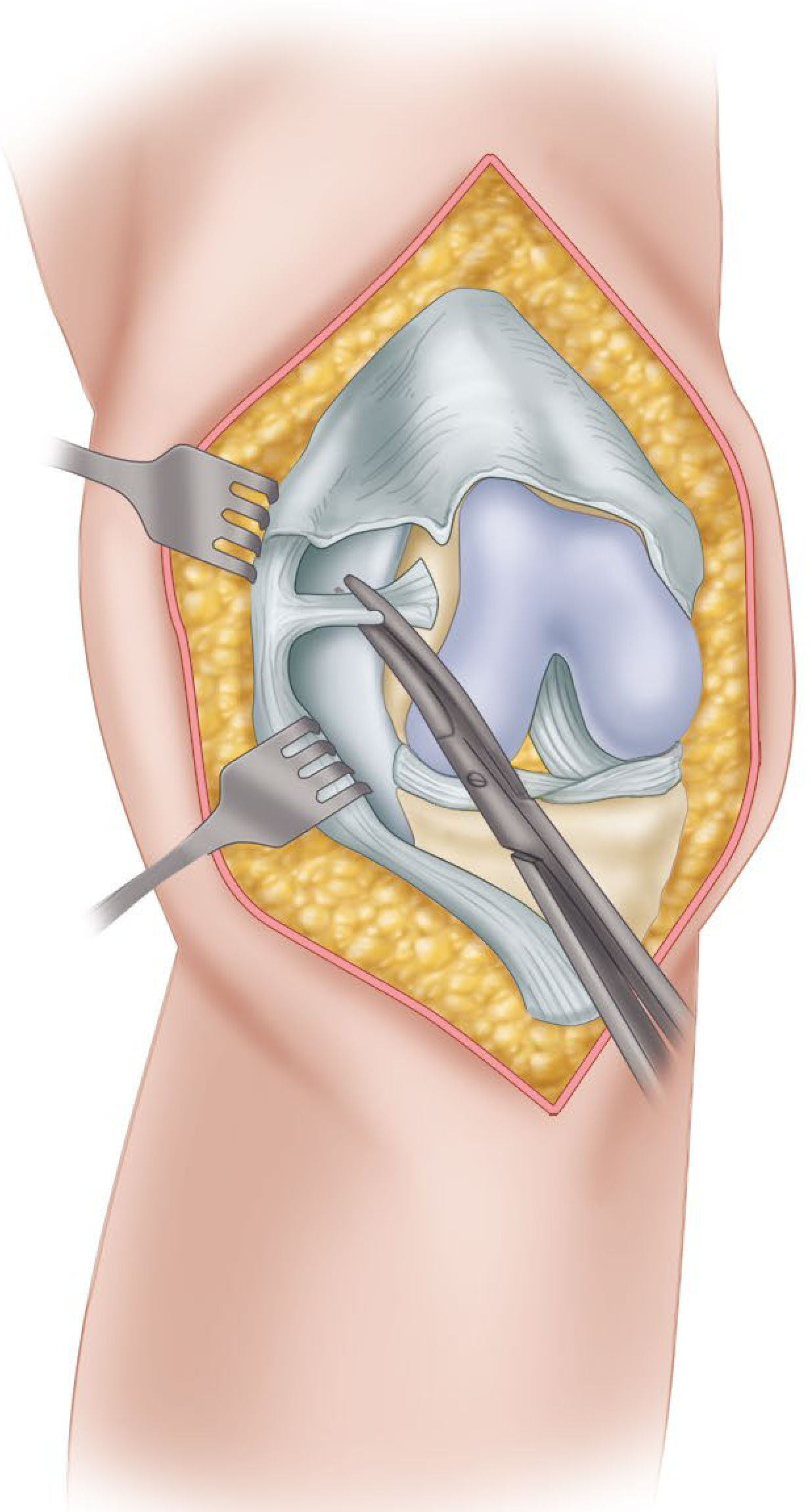
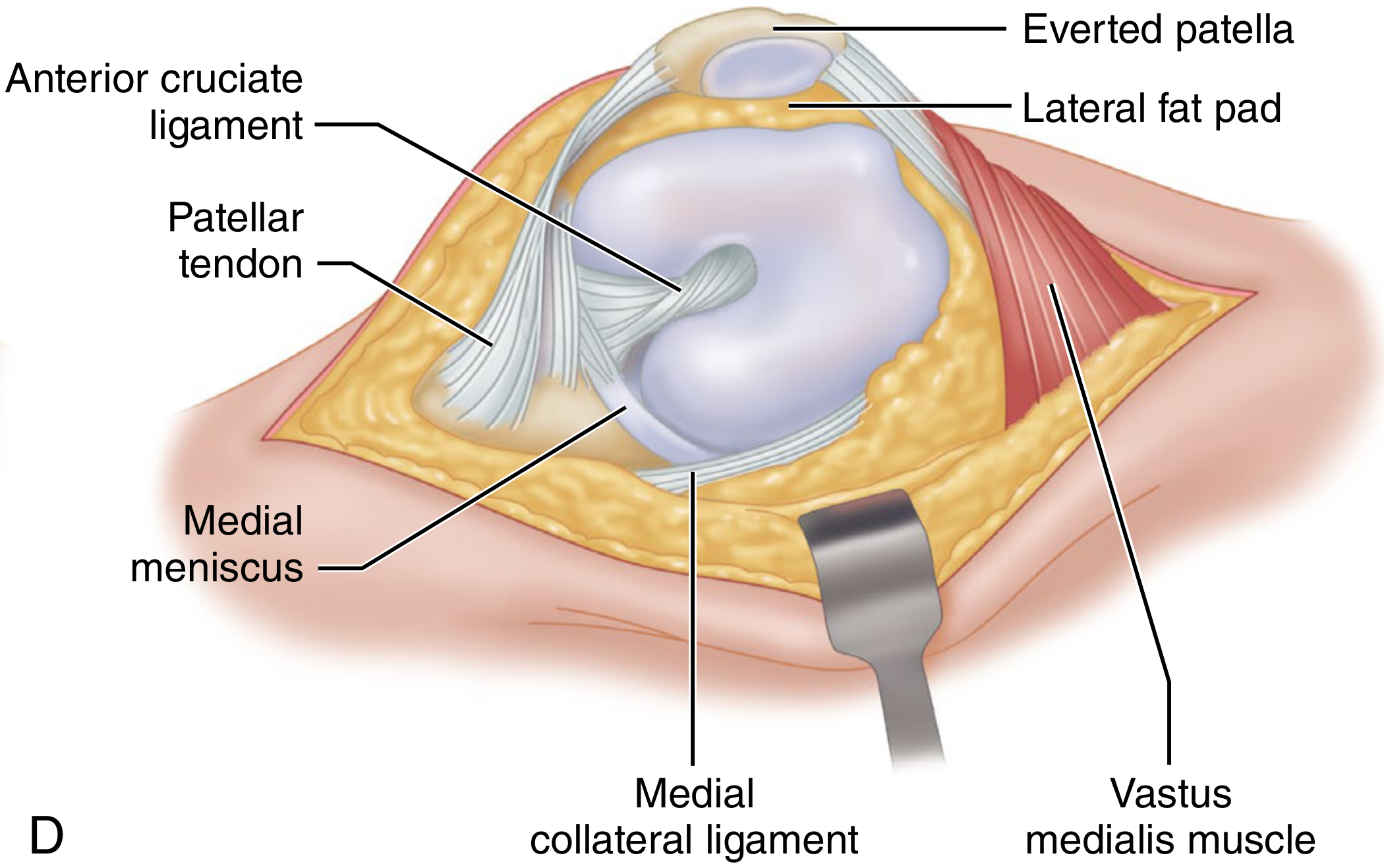
| 6 | Extend knee → evert patella → release lateral patellofemoral plicae |
| 7 | Flex knee → remove ACL and anterior horns of menisci; excise osteophytes |
| 8 | Subluxate and externally rotate tibia (relaxes extensor mechanism, reduces risk of patellar tendon avulsion) |
| 9 | Excise infrapatellar fat pad / retract everted extensor mechanism with levering retractor laterally |
- Maximum exposure of knee joint
- Suitable for primary AND revision TKA
- Usable in obese patients, stiff knees, valgus deformity
- Standard reference approach
- Disrupts quadriceps mechanism (muscle-splitting)
- Potential patellar devascularization
- Slower quadriceps recovery
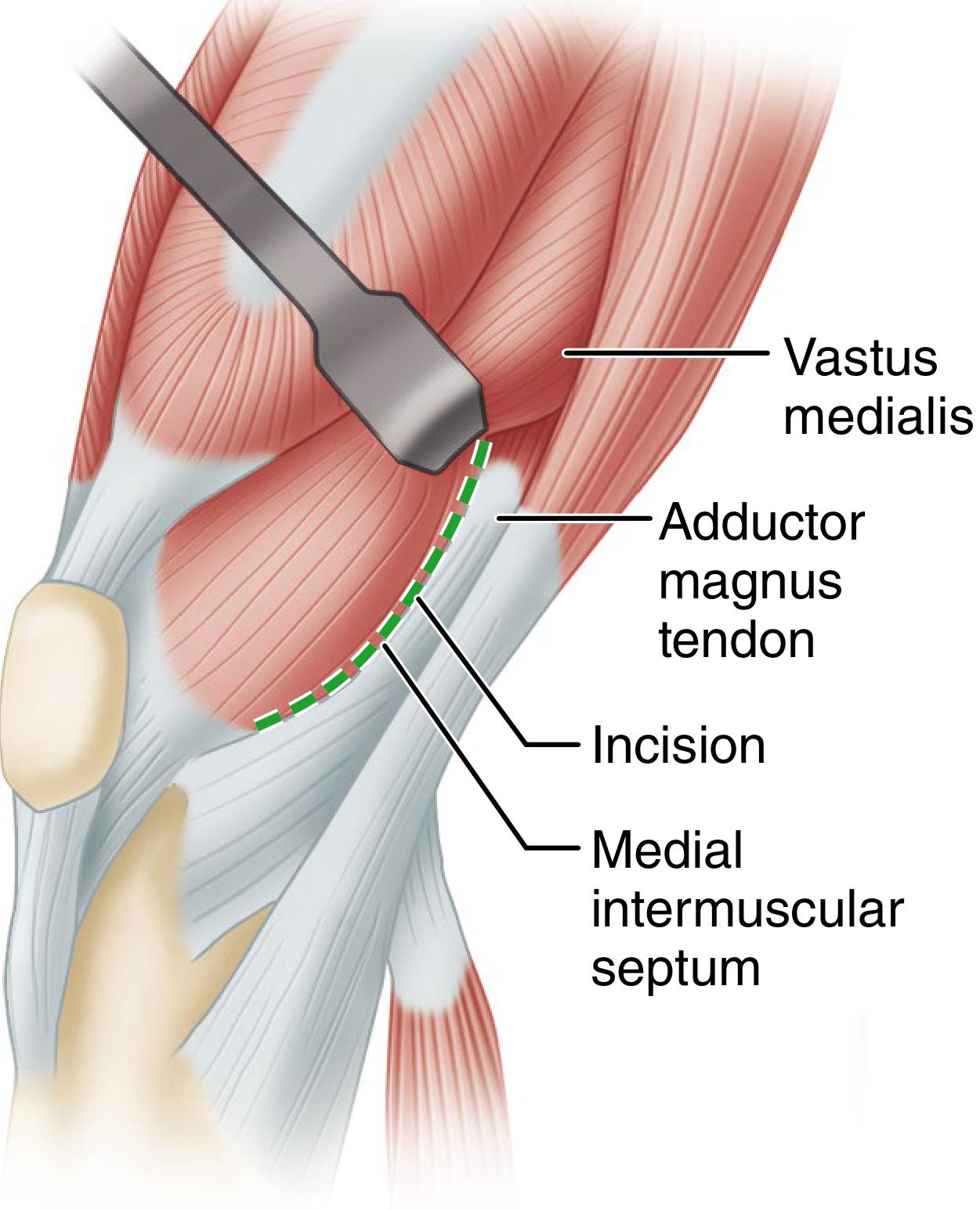
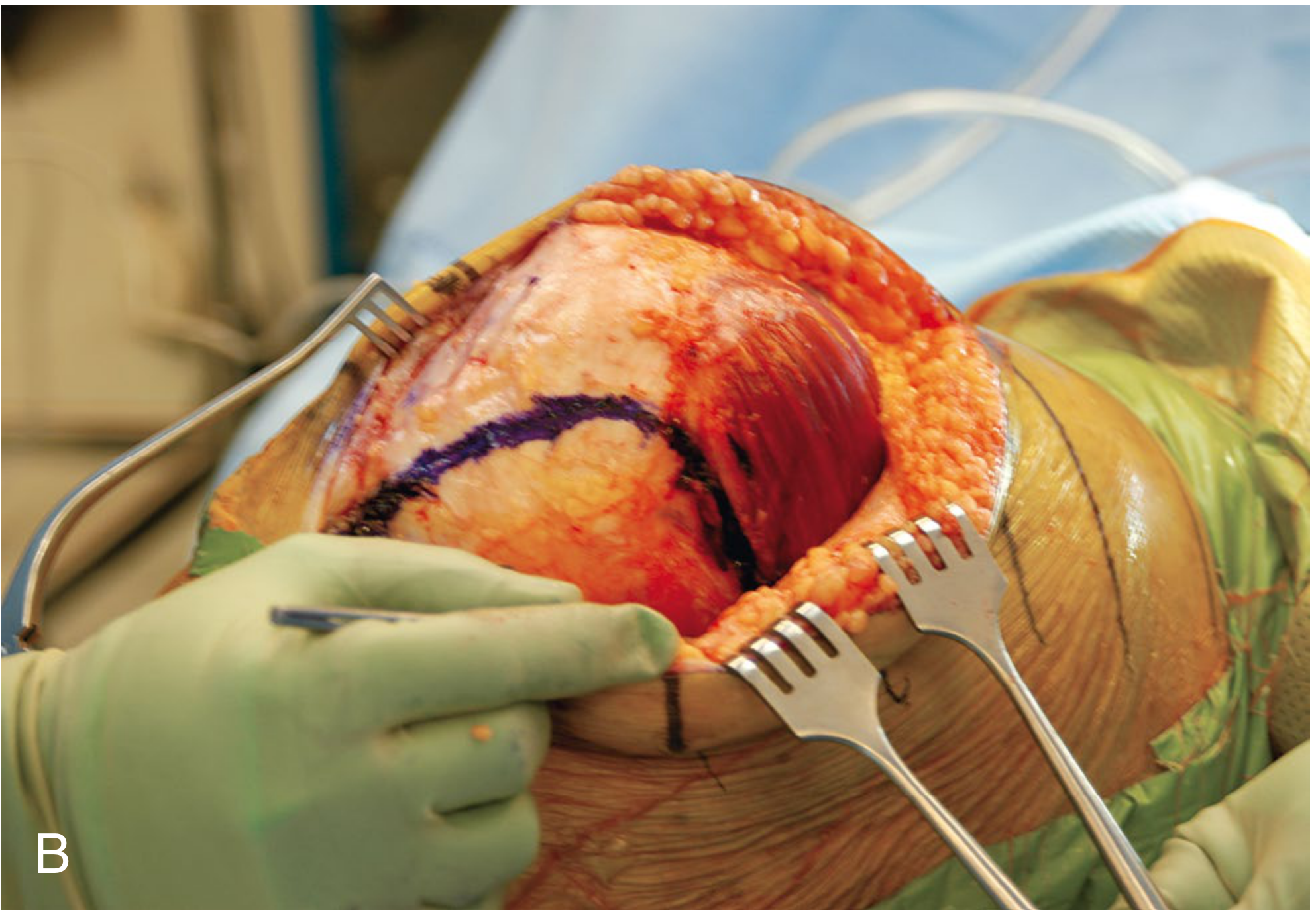
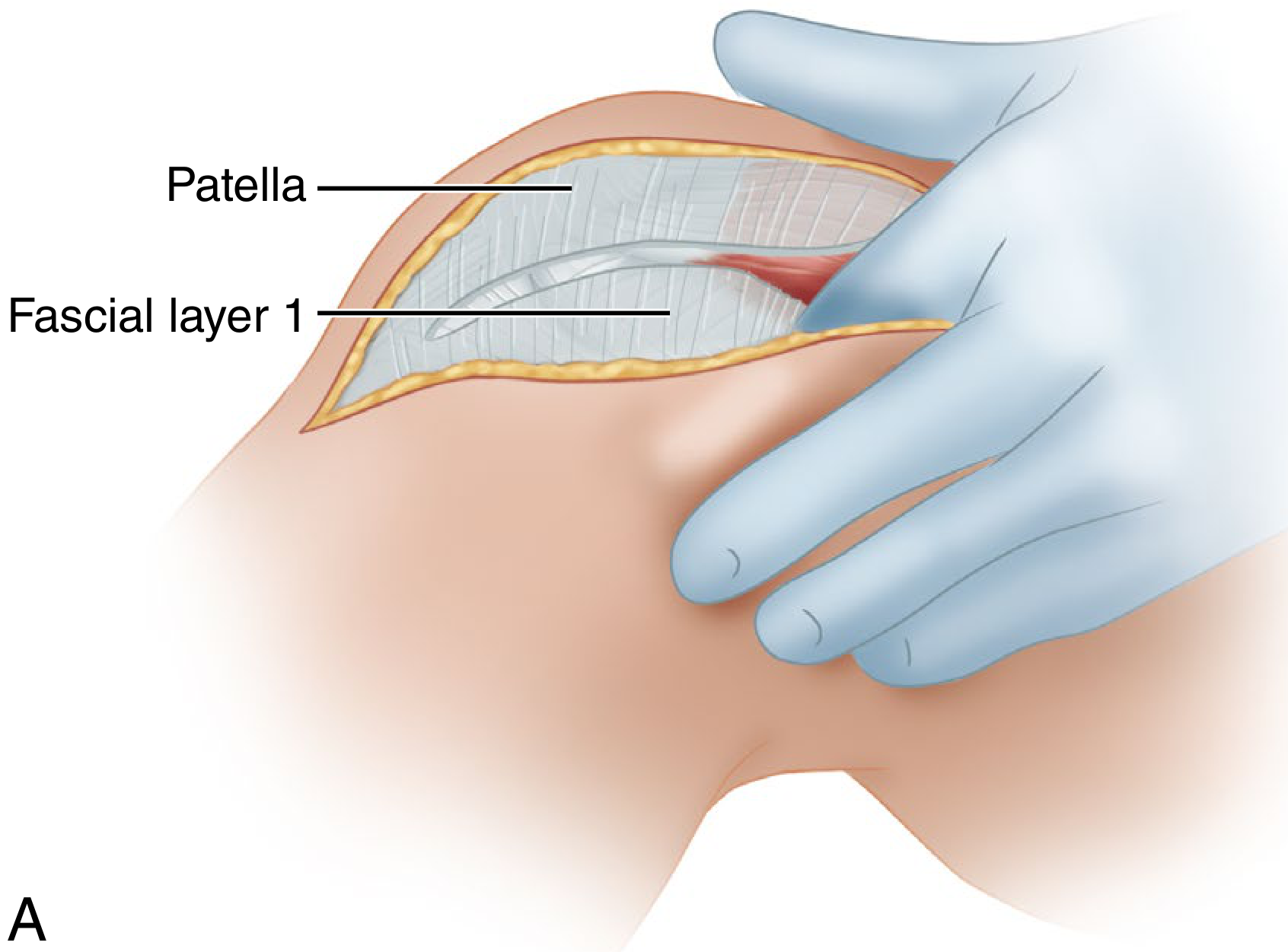
APPROACH 2: SUBVASTUS APPROACH ("Southern Approach")
Muscle-Sparing - Extensor Mechanism Intact
Step-by-Step Technique:
| Step | Action |
|---|---|
| 1 | Same anterior midline skin incision |
| 2 | Create full-thickness medial + lateral subcutaneous flaps (larger lateral flap needed for patellar subluxation pocket) |
| 3 | Incise the superficial fascia overlying vastus medialis - do NOT cut into muscle |
| 4 | Bluntly mobilize distal medial border of vastus medialis posterior to medial intermuscular septum |
| 5 | Lift origin of vastus medialis off medial intermuscular septum up to ~10 cm proximal to adductor tubercle (stay distal to femoral vessel aperture) |
| 6 | Incise synovium → dislocate entire extensor mechanism laterally as a unit |
| 7 | Release synovial-capsular attachments to undersurface of quadriceps tendon from medial to lateral (key maneuver for extensor mechanism mobilization) |
| 8 | Sublux patella into lateral gutter using 90° bent Hohman retractor; flex knee to 90° for full joint exposure |
| 9 | Closure: Simple - no muscle repair needed |
- Extensor mechanism completely intact
- Preserves vascularity to patella (supreme genicular artery intact)
- Faster quadriceps recovery
- Less postoperative pain
- Fewer patellar complications
- Reduced need for lateral release
- Obesity
- Previous upper tibial osteotomy
- Preoperative flexion <80 degrees
- Stiff knee requiring extensile exposure
- Revision TKA
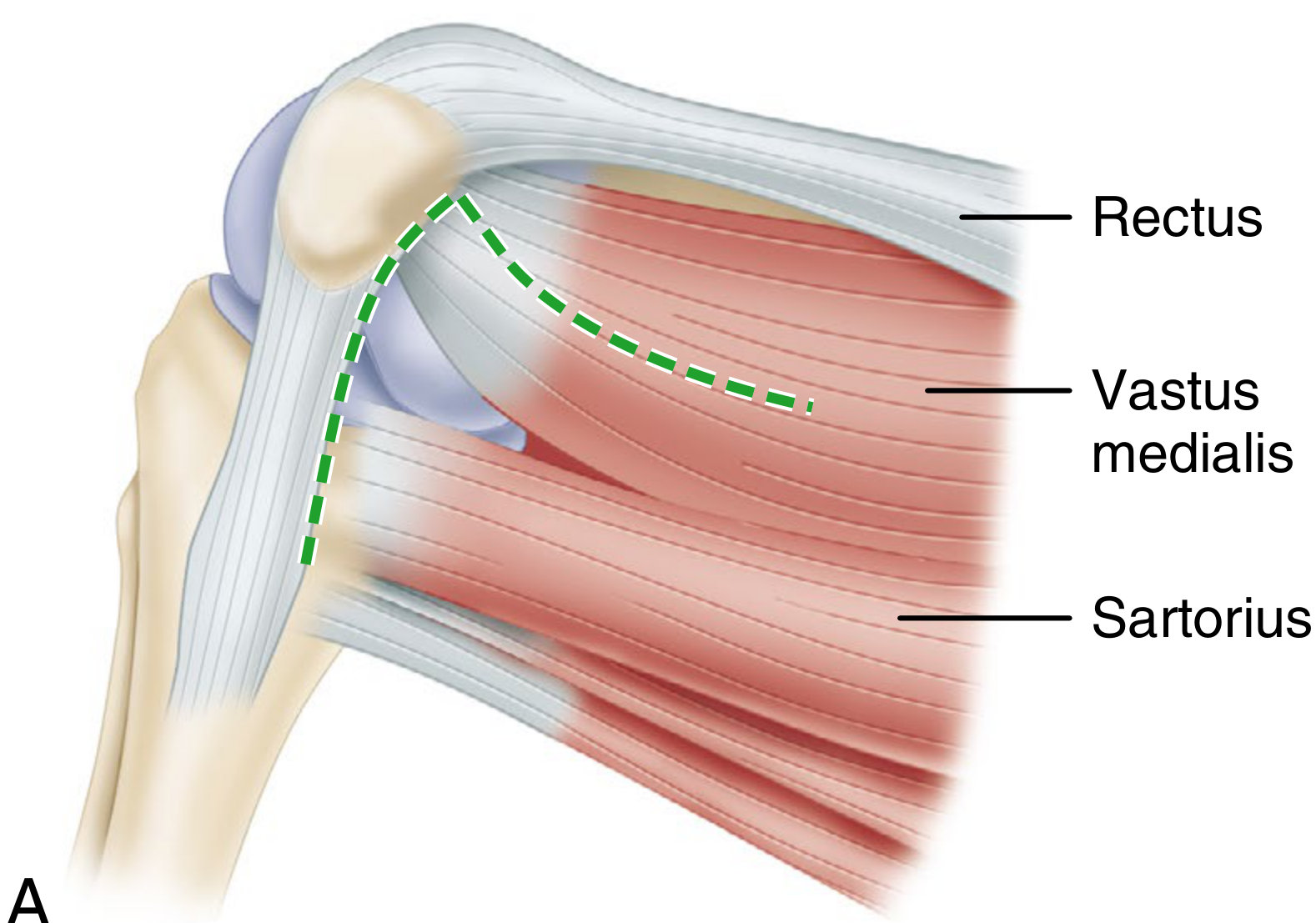
APPROACH 3: MIDVASTUS APPROACH (Engh's Approach)
Muscle-Splitting (Partial) - Moderate Option
Step-by-Step Technique:
| Step | Action |
|---|---|
| 1 | Anterior midline skin incision |
| 2 | The split in vastus medialis begins at the superomedial border of the patella |
| 3 | Extends proximally and medially toward the intermuscular septum, splitting muscle in line with its fibers |
| 4 | Safe zone: 4.5 cm from patella margin can be sharply split; further blunt dissection possible |
| 5 | Patella is subluxated (not everted) laterally for adequate exposure |
| 6 | Proceed with standard tibial and femoral bone cuts |
- Preserves supreme genicular artery
- Preserves quadriceps tendon
- Better early quadriceps function than medial parapatellar
- Intermediate exposure between parapatellar and subvastus
- Obesity
- Previous upper tibial osteotomy
- Preoperative flexion <80 degrees
- Mandatory careful hemostasis - postoperative hematomas reported
APPROACH 4: LATERAL PARAPATELLAR (Keblish Approach)
For Fixed Valgus Deformity
Step-by-Step Technique:
| Step | Action |
|---|---|
| 1 | Anterior midline skin incision |
| 2 | Lateral parapatellar arthrotomy placed 3-7 cm lateral to patella |
| 3 | Lateral retinacular complex separated into two layers: deep (capsule + synovium) and superficial |
| 4 | Deep and superficial layers separated with dissection carried medially toward patella |
| 5 | Superficial layer kept attached to patella; deep layer stays attached to ITB |
| 6 | Patella everted medially |
| 7 | At closure: layers approximated in expanded (Z-plasty) fashion to achieve lateral release simultaneously |
- Achieves lateral release at time of closure
- Avoids separate lateral release procedure
- Ideal for valgus deformity correction
APPROACH 5: EXTENSILE EXPOSURES (for Revision TKA)
A. Quadriceps Snip
- Oblique extension of medial parapatellar incision across quadriceps tendon at 45°
- Does not require modification of rehabilitation
- First choice extensile option
B. V-Y Quadricepsplasty (Coonse-Adams)
- Inverted V incision through quadriceps tendon extended distally as Y
- Used for severely stiff knees
- Requires slower rehabilitation
C. Tibial Tubercle Osteotomy (TTO) (Whiteside's technique)
- Osteotomize tibial tubercle with patellar tendon attached
- Provides maximum distal exposure
- Risk of non-union; requires screw fixation at closure
- Best for complex revision with component removal required
COMPARATIVE SUMMARY TABLE
| Feature | Medial Parapatellar | Subvastus | Midvastus | Lateral Parapatellar |
|---|---|---|---|---|
| VMO status | Cut | Intact (lifted) | Split in line | - |
| Patellar vascularity | Reduced | Preserved | Preserved | - |
| Exposure | Excellent | Good (limited stiff knee) | Moderate | Excellent (valgus) |
| Quad recovery | Slower | Fastest | Fast | - |
| Use in obesity | Yes | No | Limited | Yes |
| Revision use | Yes | No | No | No |
| Best indication | All primary TKA | Thin, flexible, routine | Routine primary | Fixed valgus knee |
| Literature outcome | Equivalent long-term | Equivalent long-term | Equivalent long-term | - |
PG Exam Note: Campbell's states: "Current literature supports no difference in early or long-term outcomes when comparing medial parapatellar, midvastus, and subvastus approaches." The medial parapatellar remains the standard and is used routinely by most surgeons for primary TKA.
HIGH-YIELD PG POINTS
- Most common approach = Medial parapatellar (Insall's) - Gold standard
- Approach for fixed valgus = Lateral parapatellar (Keblish)
- Muscle-sparing approaches = Subvastus (entire VMO intact) and Midvastus (VMO split in line with fibers)
- Subvastus = "Southern approach"; VMO lifted off medial intermuscular septum
- Midvastus safe zone = 4.5 cm from patella margin
- Patellar tendon avulsion - most feared intraoperative complication; avoid by careful attention during flexion/retraction
- Extensile options for revision: Quadriceps snip (easiest) → V-Y Quad → TTO (most extensive)
- Skin incision rule: Multiple scars → use most lateral scar (medial blood supply)
- The infrapatellar branch of the saphenous nerve is nearly always compromised → lateral knee numbness (warn patient preoperatively)
Find latest clinical guidelines on TKR approach selection in special populations
"knee arthroplasty"[MeSH Terms] AND "surgical approach" AND "special populations"
"total knee arthroplasty"[MeSH Terms] AND "obesity" AND "surgical approach"
"total knee arthroplasty" AND "valgus deformity" AND "lateral approach"
TKA TKR approach selection guidelines 2024 2025 special populations obese elderly valgus AAOS
"knee arthroplasty"[MeSH Terms] AND "surgical approach"[MeSH Terms]
"arthroplasty replacement knee"[MeSH Terms] AND "subvastus" AND outcomes
"arthroplasty replacement knee"[MeSH Terms] AND "valgus" AND approach
https://www.cureus.com/articles/413846-a-comprehensive-revie…
"total knee arthroplasty" AND "approach" AND (obesity OR valgus OR elderly OR revision OR stiff)
"knee arthroplasty" AND "medial parapatellar" AND "midvastus" OR "subvastus"
TKA surgical approach obese patients subvastus midvastus medial parapatellar evidence 2024 2025 systematic review
PMID: 37356465
PMID: 35128816
PMID: 41807933
PMID: 34405531
PMID: 37667291
PMID: 40923336
TKA approach revision knee stiff knee tibial tubercle osteotomy quadriceps snip guidelines 2024 2025
TKR Approach Selection in Special Populations: Latest Evidence (2021-2026)
KEY EVIDENCE BASE
| Evidence | Paper | PMID | Year |
|---|---|---|---|
| Network Meta-Analysis (33 RCTs) | Stubnya et al. - Subvastus Supporting Fast-Track TKA | 37356465 | 2023 |
| Network Meta-Analysis (51 RCTs, 4179 knees, 7 approaches) | Zhao et al. - Efficacy/Safety of TKA Approaches | 35128816 | 2022 |
| Network Meta-Analysis (42 RCTs) | Huh et al. - Conventional vs MIS Approaches | 41807933 | 2026 |
| Systematic Review (664 knees) | Slattery et al. - Midline vs Anterolateral incision | 34405531 | 2021 |
| Meta-Analysis (12 RCTs, 788 knees) | Yang et al. - Mini-Midvastus vs Parapatellar | 37667291 | 2023 |
| RCT | Mylonas et al. - Postural sway, PP vs MV in women | 40923336 | 2026 |
| COA Consensus Guideline | Chaudhry et al. - TKR in Obesity | COA 2025 | 2025 |
| Comprehensive Review | Alzarooni et al. - Cureus Operative Considerations | Cureus e94345 | 2025 |
1. OBESE PATIENTS (BMI >30 / >40)
- Functional outcomes in obese patients are similar to, or often better than, those in the average patient - but complication risk is markedly higher (infection, wound healing, DVT)
- The AAOS states BMI <40 as the generally accepted threshold for elective joint replacement; NICE does not impose a BMI cutoff
- The 2025 Cureus comprehensive review explicitly states: "the medial parapatellar approach remains the preferred choice in obese patients" - subvastus and midvastus are not recommended because:
- Adequate surgical visualization is compromised in excess adipose tissue
- Fat pad bulk prevents adequate lateral subluxation of the patella
- Higher hematoma risk from muscle bleeding is compounded
- Shared decision-making with patient; avoid weight bias
- BMI alone should NOT be an absolute exclusion criterion
- Preoperative optimization (nutrition, glucose control) should be offered before surgery
- Referral to tertiary centres with medical + anaesthetic + surgical expertise for high-risk obese patients
2. FAST-TRACK / ENHANCED RECOVERY (ERAS) PROGRAMS
- Subvastus (SV) showed superior ROM on days 1, 3, 4, and 6 vs. medial parapatellar
- Day 1: MD = +6.99° (CI: 1.08-12.89)
- Day 4: MD = +27.01° (CI: 18.09-35.92)
- Mini-SV showed significantly lower pain on days 1, 3, and 7
- Day 1: MD = -1.98 VAS points (CI: -2.93 to -1.03)
- Differences decrease over time; no significant advantage beyond 6 weeks
- Conclusion: Quadriceps-sparing approaches are superior for fast-track programs in appropriately selected patients
Patient selection for SV in ERAS: Normal BMI, flexible subcutaneous tissues, preoperative flexion >80°, no prior tibial osteotomy
3. GENERAL POPULATION: ALL APPROACHES COMPARED (7-Approach Network Meta-Analysis)
| Outcome | Best Approach |
|---|---|
| Shortest tourniquet time | Midvastus (MV) |
| Shortest operation time | Subvastus (SV) |
| Fastest straight leg raise | Mini-Midvastus (Mini-MV) |
| Least postoperative pain | Mini-Medial Parapatellar (Mini-MP) |
| Best ROM improvement | Medial Parapatellar (MP) |
| Shortest hospital stay | Mini-Midvastus (Mini-MV) |
| Blood loss, complications, KSS | No significant difference between any approach (p>0.05) |
Bottom line: No approach is universally superior in long-term outcomes. Choice should be driven by patient-specific factors and surgeon experience.
4. MINIMALLY INVASIVE APPROACHES (MIS-TKA)
- Best for pain: Mini-Midvastus (MMV) - SUCRA 80.0, mean rank 2.2
- Best for ROM: Minimally Invasive Quadriceps-Sparing (MQS) - SUCRA 90.0, mean rank 1.6
- Best for safety (fewest adverse effects): Subvastus (SUCRA 80.0) and conventional Quadriceps-Splitting
- Conclusion: MIS approaches give better short-term pain/ROM but conventional approaches have a better safety profile
- Surgeons must weigh both when selecting approach for individual patients
- MMV superior at 3 months: KSS (+2.89), VAS (-0.22), ROM (+1.08°)
- No significant difference at 6 and 12 months
- MMV takes longer to perform (+8.98 min) but achieves straight leg raise 1.91 days sooner
5. SKIN INCISION - ANTEROLATERAL vs. MIDLINE
| Outcome | Midline Incision | Anterolateral Incision | p-value |
|---|---|---|---|
| Altered sensation | 62% | 15% | <0.0001 |
| Wound dehiscence | 8.3% | 2.5% | 0.153 (NS) |
| Kneeling ability | Lower | Better | - |
6. VALGUS DEFORMITY
7. ELDERLY / FALL RISK PATIENTS
- Both approaches cause postoperative loss of postural sway complexity (fall risk marker)
- At 2 weeks and 1 month: Medial parapatellar group had significantly lower postural sway complexity (more random patterns = higher fall risk) compared to healthy controls
- Midvastus group showed no such significant difference from controls
- Implication for elderly/fall-prone patients: Midvastus approach may confer a postural stability advantage in the early recovery period, particularly in women
SUMMARY: APPROACH SELECTION BY POPULATION (2025-2026 Evidence)
| Population | Recommended Approach | Evidence Level | Key Source |
|---|---|---|---|
| Standard primary TKA | Medial Parapatellar | Institutional standard | Campbell's 15th Ed |
| Obese (BMI >30-40) | Medial Parapatellar | Consensus | COA 2025, Cureus 2025 |
| ERAS / fast-track protocols | Subvastus or Mini-SV | Network Meta-Analysis | Stubnya 2023 |
| Best short-term ROM | MIS Quadriceps-Sparing | Network Meta-Analysis | Huh 2026 |
| Best short-term pain | Mini-Midvastus | Network Meta-Analysis | Huh 2026 / Zhao 2022 |
| Shortest hospital stay | Mini-Midvastus | Network Meta-Analysis | Zhao 2022 |
| Fixed valgus deformity | Lateral Parapatellar (Keblish) | Expert consensus | Campbell's 15th Ed |
| Fall risk / elderly women | Midvastus (MV) | RCT | Mylonas 2026 |
| Sensory preservation (kneeling) | Anterolateral skin incision | Systematic Review | Slattery 2021 |
| Revision TKA / stiff knee | Quadriceps Snip → TTO | Expert consensus | Campbell's 15th Ed |
| Robotic-assisted TKA | Modified Subvastus (MA-MSVA) | Retrospective cohort | Springer 2025 |
CONSENSUS ACROSS ALL EVIDENCE
- No approach is superior for long-term functional outcomes - blood loss, KSS at 1 year, and complication rates are equivalent across all approaches
- Muscle-sparing approaches (SV, MV) offer a genuine early recovery advantage - best suited for ERAS programs in non-obese, flexible patients
- Medial parapatellar remains the default for complex knees - obesity, stiffness, valgus (combined with lateral release), revision
- The trend is shifting - a 2025 Cureus review notes the field is moving toward muscle-sparing and infrapatellar fat-pad (IFFP)-preserving techniques, supported by short-term evidence of faster rehabilitation
- Surgeon experience trumps approach - the 2022 Zhao network meta-analysis found no difference in safety or long-term KSS; choosing a familiar approach is still defensible