Short term regulation of blood pressure
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Reading File
Finding Sources
Loading Image
I now have everything needed for a comprehensive, well-illustrated answer. Here is the full response:
Short-Term Regulation of Blood Pressure
Short-term blood pressure regulation operates over seconds to minutes and relies primarily on neural reflex mechanisms (negative-feedback loops). The core components of every such loop are: a sensor/receptor, afferent neural pathways, a CNS coordinating center, efferent pathways, and effectors (heart, blood vessels, adrenal medulla).
- Medical Physiology (Boron & Boulpaep)
- Guyton and Hall Textbook of Medical Physiology
- Costanzo Physiology 7th Edition
1. The Baroreceptor (Baroreflex) System - Primary Mechanism
Anatomy of Baroreceptors
Baroreceptors are stretch-sensitive mechanoreceptors (spray-type nerve endings) in the walls of major arteries. They are most concentrated at two sites:
- Carotid sinus - the dilation at the origin of the internal carotid artery, just above the bifurcation of the common carotid. These respond to both increases and decreases in pressure.
- Aortic arch - aortic baroreceptors respond primarily to increases in pressure and operate at levels ~30 mmHg higher than carotid receptors.
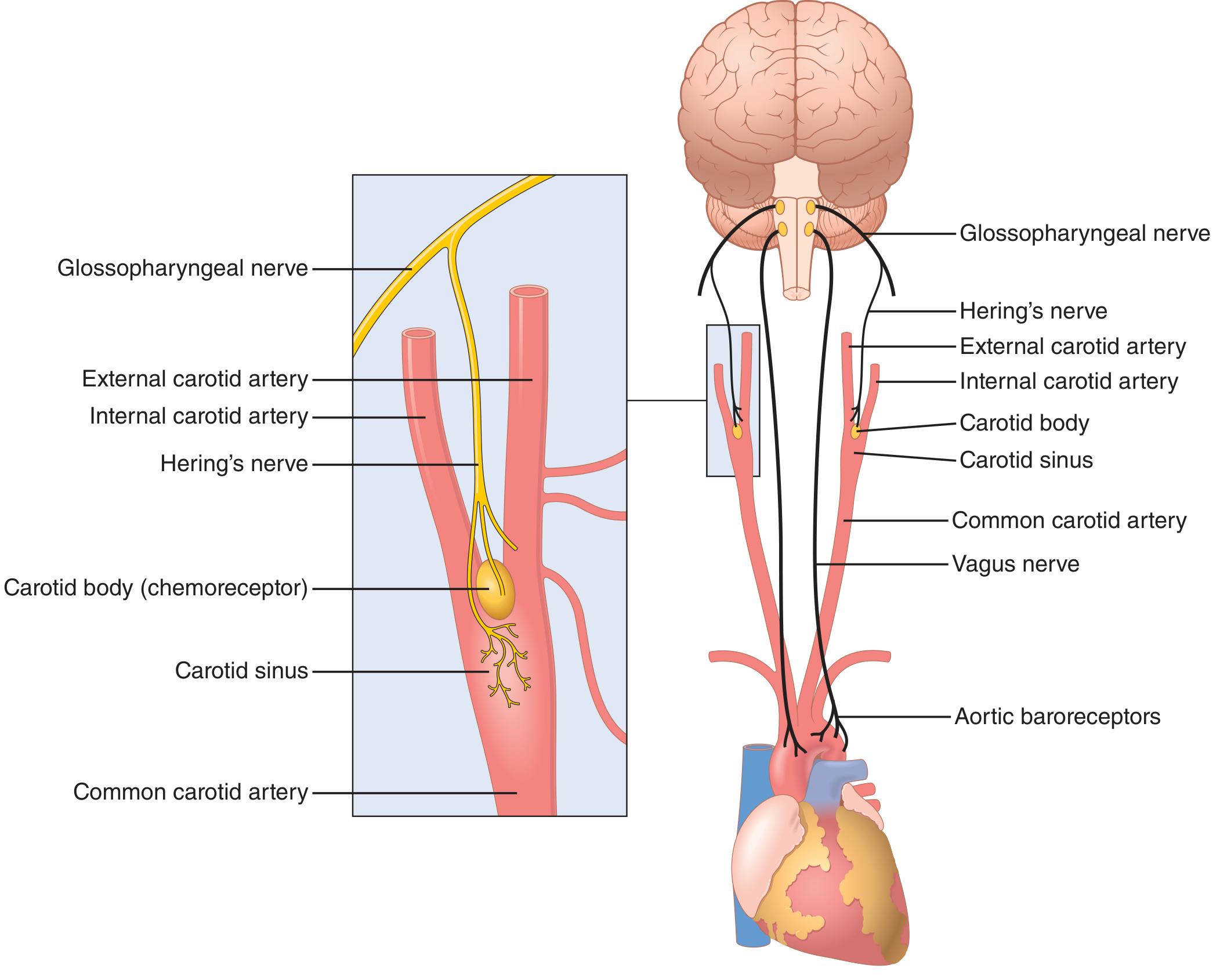
Afferent pathways:
- Carotid sinus baroreceptors → Hering's nerve → Glossopharyngeal nerve (CN IX) → Nucleus tractus solitarius (NTS) in the medulla
- Aortic arch baroreceptors → Vagus nerve (CN X) → NTS
How Baroreceptors Work
When arterial pressure rises, the vessel wall is stretched, generating a depolarizing receptor potential that increases action potential firing frequency in afferent nerves. The baroreceptors are excited above pressures of 50-60 mmHg, respond maximally near 180 mmHg, and are most sensitive in the normal operating range around 100 mmHg - where even a small pressure change produces a large reflex change.
Importantly, baroreceptors are more sensitive to the rate of change of pressure than to static pressure. A rapidly rising pressure produces approximately double the firing rate compared to the same sustained pressure level.
Brain Stem Cardiovascular Centers
The nucleus tractus solitarius (NTS) in the medulla integrates baroreceptor input and coordinates three tonically active cardiovascular centers:
| Center | Division | Effect |
|---|---|---|
| Vasoconstrictor (C1) | Sympathetic | Arteriolar and venular constriction |
| Cardiac accelerator | Sympathetic | ↑ HR, ↑ contractility, ↑ AV conduction |
| Cardiac decelerator | Parasympathetic (vagus) | ↓ HR |
Integrated Baroreceptor Reflex Response
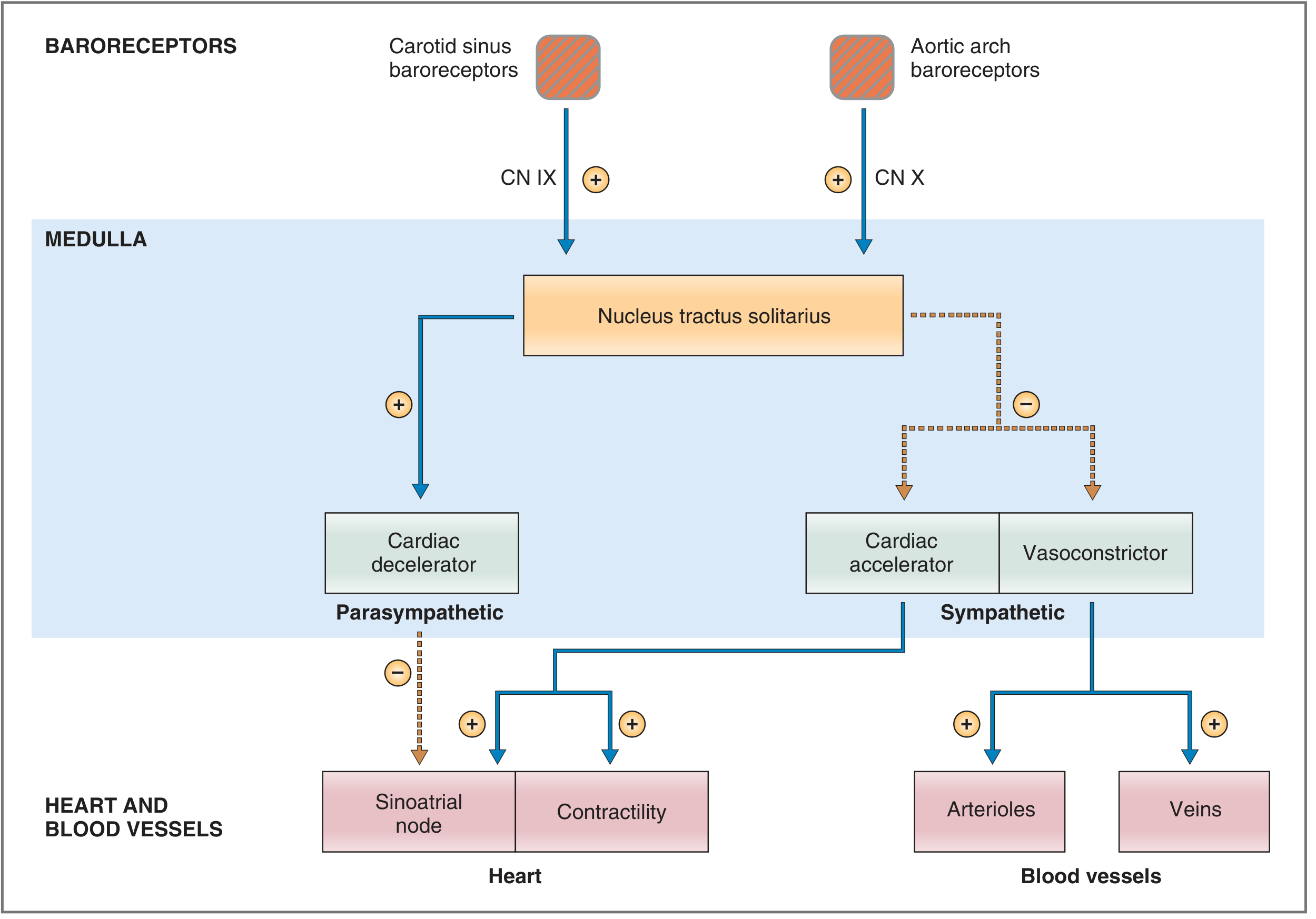
Response to a RISE in arterial pressure:
- Increased baroreceptor firing → NTS activated
- NTS increases parasympathetic outflow → decreased heart rate (cardiac decelerator activated)
- NTS inhibits sympathetic outflow → decreased HR, decreased contractility, decreased cardiac output
- Reduced sympathetic tone to vessels → arteriolar vasodilation (decreased TPR) and venodilation (increased unstressed volume, reduced venous return)
- Net result: BP falls back toward normal
Response to a FALL in arterial pressure (e.g., hemorrhage):
| Parameter | Compensatory Response |
|---|---|
| Carotid sinus nerve firing | ↓ |
| Heart rate | ↑ |
| Contractility | ↑ |
| Cardiac output | ↑ |
| Unstressed venous volume | ↓ (increases venous return) |
| Total peripheral resistance (TPR) | ↑ |
| Adrenal medulla (circulating epinephrine) | ↑ |
Arteriolar constriction is generalized (skin, gut, kidney, skeletal muscle) but spares the coronary and cerebral circulations.
Importance of the Baroreceptor System
Without baroreceptors, arterial pressure fluctuates 2.5-fold more during daily activities. The baroreflex buffers moment-to-moment variability by about two-thirds and operates within seconds. However, it resets over 1-2 days if chronically exposed to a new pressure level - explaining why it does not correct chronic hypertension.
2. Chemoreceptor Reflexes
Peripheral chemoreceptors are located in the carotid and aortic bodies (closely related to baroreceptor anatomy - as seen in the diagram above, the carotid body is adjacent to the carotid sinus). They are stimulated by:
- Low blood PO₂ (hypoxia)
- High PCO₂ (hypercapnia)
- Low pH (acidosis)
Effect on blood pressure: Chemoreceptor stimulation causes sympathetic vasoconstriction and a rise in BP. This is less important for moment-to-moment pressure control under normal conditions, but becomes significant when O₂ delivery falls (e.g., in circulatory shock, asphyxia).
Central chemoreceptors in the medullary vasomotor center respond directly to increased CO₂/H⁺ in the cerebrospinal fluid, powerfully stimulating the vasomotor center and raising BP.
3. CNS Ischemic Response ("Last-Ditch" Mechanism)
When blood flow to the vasomotor center in the medulla falls critically (arterial pressure < 60 mmHg, most potent stimulus at 15-20 mmHg), CO₂ and H⁺ accumulate directly in the vasomotor center, triggering a massive sympathetic discharge:
- Mean arterial pressure can be elevated to as high as 250 mmHg
- Peripheral vasoconstriction so intense that some organs (e.g., kidneys) may transiently cease function
- This is a purely emergency mechanism, not involved in day-to-day regulation
The Cushing Reaction is a variant: when intracranial pressure rises to equal arterial pressure, cerebral blood flow is compromised, triggering the CNS ischemic response. BP rises until it exceeds intracranial pressure and flow is restored. This protects vital brainstem centers from ischemia.
4. Other Short-Term Neural/Reflex Mechanisms
Atrial (Low-Pressure) Receptors
Low-pressure volume receptors (stretch receptors) in the atrial walls and pulmonary vessels sense venous return/blood volume. When atrial stretch increases:
- Heart rate increases (Bainbridge reflex - volume-mediated tachycardia)
- ADH release is inhibited (allows fluid excretion)
Abdominal Compression Reflex
During baroreceptor/chemoreceptor activation, simultaneous skeletal nerve signals to abdominal muscles cause muscular contraction that compresses venous reservoirs, translocating blood back to the heart and increasing venous return and cardiac output.
Pulmonary Inflation Reflex (Bainbridge Reflex)
Lung inflation during inspiration activates stretch receptors that briefly inhibit the cardiac decelerator center, causing mild inspiratory tachycardia (the basis of sinus arrhythmia).
5. Intermediate-Term Mechanisms (Minutes to Hours)
These operate after the initial neural reflexes have acted:
| Mechanism | Onset | Action |
|---|---|---|
| Renin-Angiotensin-Aldosterone | Minutes | Low BP → ↑ renin → ↑ angiotensin II → vasoconstriction + aldosterone → Na/water retention |
| Stress Relaxation of Vessels | Minutes | Vessel walls accommodate to new volume over time (pressure normalization) |
| Capillary Fluid Shift | 10-60 min | High BP → fluid shifts from capillaries into interstitium, reducing blood volume; low BP does the reverse |
| ADH (Vasopressin) | Minutes | Low BP/volume → ↑ ADH → water retention + direct vasoconstriction |
Summary: Timeline of Pressure Control
| Timeframe | Mechanism | Potency |
|---|---|---|
| Seconds | Baroreceptor reflex | Very rapid, ±50 mmHg correction |
| Seconds-minutes | Chemoreceptor reflex | Moderate; mainly low-O₂ states |
| Emergency | CNS ischemic response | Extreme, only when BP < 60 mmHg |
| Minutes | Renin-angiotensin, ADH, capillary shift | Sustained support |
| Hours-days | Renal pressure-diuresis (long-term) | Most powerful long-term regulator |
Short-term regulation is dominated by the baroreceptor reflex, which acts within seconds via the NTS, modulating sympathetic and parasympathetic outflow to the heart (HR and contractility) and vessels (TPR and venous capacitance). The chemoreceptor reflex and CNS ischemic response serve as backup systems for more extreme conditions.
This is a shared conversation. Sign in to Orris to start your own chat.