Mildly bitter taste in the mouth and mild fever and headache since 3 months without medication what can be caused
Reading File
Searching the Web
chronic bitter taste fever headache 3 months causes differential diagnosis
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Loading Image
Finding Sources
Now I have enough information to compile a thorough, well-organized response. Let me put this together.
Possible Causes of Bitter Taste + Mild Fever + Headache Persisting 3 Months
Having all three symptoms together for 3 months without medication makes this a chronic, systemic process that needs medical evaluation. Here is a systematic breakdown of the most likely causes, from most to least common.
1. Chronic Sinusitis (Most Common)
This is the top suspect when all three symptoms overlap. Chronic sinusitis causes:
- Bitter/bad taste from post-nasal drip - infected mucus drains down the back of the throat, tasting foul or bitter
- Low-grade fever from ongoing bacterial or fungal infection of the sinus cavities
- Headache from sinus pressure, especially frontal or behind the eyes
It can smolder for months, especially if initially undertreated. Look for nasal congestion, facial pressure, or colored nasal discharge alongside your symptoms.
2. Helicobacter pylori (H. pylori) Gastritis
A very common bacterial stomach infection that is frequently silent or causes only mild, vague symptoms:
- The bacteria produce urease, creating ammonia - which gives a distinctly bitter/metallic taste in the mouth
- Can trigger low-grade systemic inflammation and mild fever
- Headache is a reported associated symptom
- Affects roughly half the global population in some regions
3. Liver/Biliary Disease (Hepatitis, Fatty Liver, Cholecystitis)
When the liver is not processing bile properly, bile acids can reflux and cause a persistent bitter taste. Conditions to consider:
- Viral hepatitis B or C - can cause months of low-grade fever, fatigue, headache, and taste changes
- Non-alcoholic fatty liver disease (NAFLD) - increasingly common, causes vague symptoms
- Gallbladder disease or bile duct issues - bile reflux produces a classic bitter taste, especially in the morning
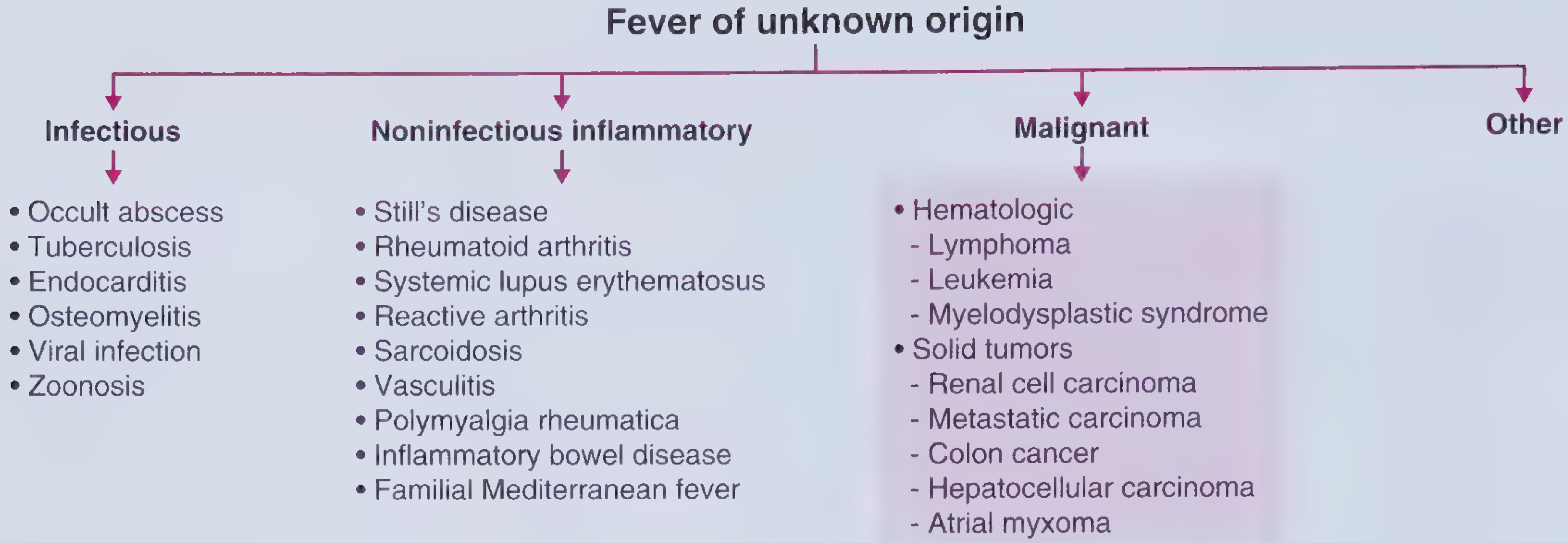
4. Chronic/Occult Infection (Fever of Unknown Origin category)
Per Harrison's Principles of Internal Medicine (2025), when fever persists beyond 3 weeks without a clear source, this enters "fever of unknown origin" (FUO) territory. Infectious causes include:
- Tuberculosis (TB) - a classic cause of chronic low-grade fever + headache; can be pulmonary or extrapulmonary
- Endocarditis - slow-growing bacteria on heart valves cause prolonged low-grade fever
- Occult abscess - a hidden abscess (dental, abdominal) can produce smoldering fever for months
- Viral infections - CMV, EBV (mono), or HIV can produce a protracted illness with fever lasting weeks to months
- Zoonotic infections - brucellosis, Q fever, cat-scratch disease (Bartonella) if relevant animal exposure
- Frameworks for Internal Medicine
5. Dental/Gum Disease (Periodontitis or Dental Abscess)
- A chronic dental abscess or severe gum disease continuously releases bacteria and pus into the mouth, causing a persistent bitter/metallic taste
- Can also cause systemic low-grade fever and referred headache
- Worth checking if you haven't had a dental exam recently
6. Gastroesophageal Reflux Disease (GERD) / Bile Reflux
- Bile or stomach acid reaching the mouth creates a sour-bitter taste
- Can coexist with headache from sleep disruption
- However, GERD alone typically doesn't cause fever - if fever is present, another cause should also be sought
7. Autoimmune / Inflammatory Conditions
As noted in the FUO framework (Frameworks for Internal Medicine), noninfectious inflammatory causes of prolonged fever include:
- Systemic Lupus Erythematosus (SLE) - especially in young women; causes fever, fatigue, headache, and various oral/taste symptoms
- Adult-onset Still's disease - dramatic ferritin elevation, fever, arthralgias
- Sarcoidosis - granulomatous disease affecting multiple organs
- Vasculitis - especially Giant Cell Arteritis in patients over 50 (causes headache + fever)
8. Less Common but Important
| Condition | How it fits |
|---|---|
| Chronic kidney disease | Uremia causes bitter/metallic taste + systemic symptoms |
| Thyroid disease | Hyperthyroidism can cause low-grade fever + headache |
| Medications/supplements | Some vitamins, iron, or herbal remedies cause bitter taste (even if no prescription drugs) |
| Psychological/anxiety | Can amplify taste perception, but wouldn't explain real fever |
Red Flags - Seek Prompt Evaluation if You Have Any of These
- Night sweats or significant weight loss (>2 lbs/week) - raises concern for TB, lymphoma, or other malignancy
- Stiff neck or neck pain with fever and headache - could indicate meningitis
- Yellow skin or eyes (jaundice) - liver involvement
- Swollen lymph nodes
- Fever above 38.5°C (101.3°F)
- Worsening over time rather than staying stable
What Tests to Expect
A doctor will likely order:
- Blood tests: CBC, liver enzymes (ALT, AST), CRP/ESR (inflammation markers), blood cultures
- H. pylori test: breath test, stool antigen, or blood serology
- Imaging: chest X-ray (TB, sarcoidosis), abdominal ultrasound (liver, gallbladder)
- Dental exam: rule out abscess
- Nasal/sinus exam or sinus CT: rule out chronic sinusitis
- Viral serology: hepatitis B/C, EBV, CMV, HIV if risk factors present
Three months without treatment is long enough that this genuinely warrants a proper workup - the symptoms are mild but persistent duration matters. Please see a primary care physician or internist soon.
Disclaimer: This information is for educational purposes only and does not replace a medical consultation. Only a doctor can diagnose and treat your condition.
What is typhoid and what is the cause of the typhoid and what is the statement of typhoid fever?
Reading File
Searching the Web
typhoid fever definition cause symptoms clinical features 2024
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Now I have excellent, authoritative content from Harrison's (2025) and Park's Textbook of Preventive and Social Medicine. Let me compile the full answer.
Typhoid Fever - Complete Overview
What is Typhoid?
Typhoid fever (also called enteric fever) is a serious systemic bacterial infection characterized by prolonged fever and abdominal pain. It was initially called "typhoid" because of its clinical similarity to typhus. In the early 1800s, it was formally defined as a distinct illness based on its association with enlarged Peyer's patches (immune tissue in the intestine) and mesenteric lymph nodes. In 1869, the term "enteric fever" was proposed as an alternative, though both terms are used interchangeably today.
"Enteric (typhoid) fever is a systemic disease characterized by fever and abdominal pain and caused by dissemination of S. Typhi or S. Paratyphi."
- Harrison's Principles of Internal Medicine, 22nd Ed. (2025)
"Typhoid fever is the result of systemic infection mainly by S. typhi... clinically characterized by a typical continuous fever for 3 to 4 weeks, relative bradycardia with involvement of lymphoid tissues and considerable constitutional symptoms."
- Park's Textbook of Preventive and Social Medicine
Cause of Typhoid
The Bacteria
Typhoid is caused by Salmonella enterica serotype Typhi (S. Typhi), a gram-negative rod-shaped bacterium. Paratyphoid fever (a milder form of enteric fever) is caused by S. Paratyphi serotypes A, B, and C.
S. Typhi has three main surface antigens:
- O antigen (somatic/cell wall)
- H antigen (flagellar)
- Vi antigen (capsular - related to virulence)
How It Spreads (Transmission)
Typhoid spreads through the fecal-oral route. The bacteria are shed in the stool and urine of infected people and carriers.
Primary sources of infection:
- Feces and urine of cases or carriers
Secondary (vehicle) sources:
- Contaminated drinking water or ice
- Contaminated food (especially raw fruits and vegetables grown in sewage-fertilized fields)
- Street food and drinks
- Flies (mechanical vectors)
- Unwashed hands (fingers)
Reservoir
Humans are the ONLY known reservoir of S. Typhi - there is no animal source. The bacteria can persist in:
- Chronic carriers: people who continue shedding bacteria for more than a year after infection (2-5% of cases). The bacteria persist in the gallbladder and biliary tract. The famous case of "Typhoid Mary" - who caused over 1,300 cases in her lifetime - is a classic example of a chronic carrier.
Risk Factors
- Poor sanitation and lack of clean drinking water
- Living in or traveling to endemic areas (South Asia, Africa, Latin America)
- Flooding events
- Prior Helicobacter pylori infection (reduces gastric acid, a natural barrier)
- Contact with an infected household member
- No prior vaccination
Problem Statement of Typhoid Fever
Global Burden
Typhoid fever occurs in all parts of the world where water supplies and sanitation are substandard. According to the WHO:
| Statistic | Figure |
|---|---|
| Global annual cases (typhoid) | 11-21 million |
| Global annual deaths | 110,000-280,000 |
| Most affected region | South Asia (India, Pakistan, Bangladesh, Nepal) and Africa |
| Most affected age group | Children 5-19 years |
In some urban areas of endemic countries, incidence exceeds 1,000 cases per 100,000 children. The disease continues to be a major public health problem in developing Asia, Africa, and Latin America.
Drug Resistance - A Growing Crisis
Since the 1980s, multidrug-resistant (MDR) strains have emerged:
- MDR S. Typhi is resistant to the 3 traditional first-line antibiotics: chloramphenicol, ampicillin, and cotrimoxazole
- Extensively drug-resistant (XDR) S. Typhi emerged in Pakistan in 2016 and has spread internationally via air travel
- XDR strains are additionally resistant to fluoroquinolones and third-generation cephalosporins, leaving only azithromycin as an oral option
- Without effective treatment, typhoid fever kills up to 10-20% of infected people
Clinical Course (Symptoms by Week)
The incubation period is typically 10-14 days (range: 5-21 days).
Week 1 - Early Phase
- Gradual onset of fever rising in a "stepladder" pattern, reaching 38.8°-40.5°C (101.8°-104.9°F)
- Headache (reported in ~80% of patients)
- Malaise, anorexia (loss of appetite ~55%)
- Dry cough (~30%), chills (35-45%)
- Constipation is more common early; diarrhea may develop later
- Abdominal pain (30-40%)
Week 2 - Established Disease
- High sustained fever
- Rose spots: a characteristic pink rash appearing on the trunk - pink papules 2-3 mm in diameter that fade on pressure and disappear in 3-4 days
- Relative bradycardia (pulse slower than expected for the degree of fever)
- Enlarged liver (hepatomegaly) and/or spleen (splenomegaly)
- "Typhoid tongue" - white-coated tongue with red edges
Week 3-4 - Complications (in untreated cases ~10%)
- Intestinal hemorrhage - sudden temperature drop, signs of shock, blood in stool
- Intestinal perforation - most dangerous complication, often during week 3
- Pneumonia, myocarditis, nephritis, cholecystitis
- Neuropsychiatric: delirium occurs in ~25% of hospitalized cases; encephalopathy, seizures in children
Diagnosis
| Test | Notes |
|---|---|
| Blood culture | Gold standard; positive in ~80% in week 1, mainstay of diagnosis |
| Bone marrow culture | Most sensitive even after antibiotics started |
| Stool culture | Positive later in disease |
| Widal test (Felix-Widal) | Measures O and H antibodies; only moderate sensitivity/specificity, can be falsely positive in malaria or other infections |
| Typhidot / Typhidot-M | Rapid IgM/IgG test, takes ~3 hours |
| Tubex test | Detects IgM against O9 antigen in minutes |
Treatment
- First line (current): Ceftriaxone (IV), azithromycin (oral), fluoroquinolones (where susceptible)
- Older drugs (now often resistant): Chloramphenicol, ampicillin, cotrimoxazole
- For XDR strains: Azithromycin or carbapenems in severe cases
Prevention
Three lines of defense:
- Safe water and sanitation - the most effective long-term measure
- Food hygiene - safe food handling, avoiding street food in endemic areas, washing hands
- Vaccination - two approved vaccine types:
- Vi polysaccharide vaccine (injectable, for adults and children >2 years)
- Typhoid Conjugate Vaccine (TCV) - newer, more immunogenic, recommended by WHO for children in endemic countries, provides longer-lasting protection
Sources: Harrison's Principles of Internal Medicine 22nd Ed. (2025, McGraw Hill) | Park's Textbook of Preventive and Social Medicine | Tintinalli's Emergency Medicine | MSD Manual Professional Edition
This is a shared conversation. Sign in to Orris to start your own chat.