I now have comprehensive material from Park's textbook. Let me compile the full NEET PG epidemiology notes.
📚 EPIDEMIOLOGY - NEET PG Complete Notes
(Based on Park's Textbook of Preventive & Social Medicine)
1. DEFINITION & SCOPE
Definition (Last, 1988): "The study of the distribution and determinants of health-related states or events in specified populations, and the application of this study to control of health problems."
Key Words:
- Distribution = Who, where, when gets the disease (Descriptive epidemiology)
- Determinants = Why and how (Analytical epidemiology)
- Population = Unit of study (not individual - that's clinical medicine)
Epidemiology vs Clinical Medicine:
| Feature | Epidemiology | Clinical Medicine |
|---|
| Unit of study | Defined population | Individual patient |
| Concern | Both sick and healthy | Sick patient |
| Output | Rates | Diagnosis/treatment |
| Approach | Investigator goes to community | Patient comes to doctor |
2. AIMS OF EPIDEMIOLOGY (IEA - Three Main Aims)
- Describe the distribution and magnitude of health/disease problems in human populations
- Identify aetiological factors (risk factors) in pathogenesis of disease
- Provide data for planning, implementation and evaluation of health services
Ultimate aim: Eliminate/reduce the health problem + promote health and well-being of society.
3. EPIDEMIOLOGICAL TRIAD (Triangle of Epidemiology)
Three components:
- Host - human susceptibility
- Agent - causative factor
- Environment - external conditions
All three must interact for disease to occur. This is the classic model for infectious diseases.
4. BASIC MEASUREMENTS IN EPIDEMIOLOGY
A. Rate vs Ratio vs Proportion
| Term | Definition | Example |
|---|
| Rate | Change per unit time; numerator included in denominator | Incidence rate |
| Ratio | Comparison of two quantities; numerator NOT in denominator | Sex ratio |
| Proportion | Numerator IS part of denominator; no time element | Prevalence |
B. INCIDENCE RATE
Definition: Number of NEW cases occurring in a defined population during a specified period of time.
Formula:
$$\text{Incidence} = \frac{\text{No. of new cases during given time period}}{\text{Population at-risk during that period}} \times 1000$$
Key features:
- Only NEW cases
- Must include unit of time (e.g., per 1000 per year)
- Not influenced by duration of disease
- Generally used for acute conditions
Special Incidence Rates:
Attack Rate (Case Rate)
- Incidence rate during an epidemic (expressed as %)
- Used when population is exposed for a limited period
- Formula: (New cases / Population at risk) × 100
Secondary Attack Rate (SAR)
- Number of cases that occur in a household within the maximum incubation period following exposure to a primary case
- Formula: (New cases among contacts / Total susceptible contacts) × 100
- Reflects infectivity of an agent
- Excludes the primary case from denominator
C. PREVALENCE RATE
Definition: All current cases (old + new) existing at a given point in time or over a period of time.
Note: Prevalence is technically a ratio, not a true rate (no time element in numerator)
Types:
| Type | Definition | Formula |
|---|
| Point Prevalence | All cases at one point in time | (All current cases / Population at that time) × 100 |
| Period Prevalence | All cases during a defined period | (All cases during period / Mid-period population) × 100 |
When "prevalence" is used without qualification = Point prevalence
D. Relationship: Incidence & Prevalence
$$P = I \times D$$
Where P = Prevalence, I = Incidence, D = Mean duration of disease
- Prevalence increases when: incidence ↑ OR duration ↑ (better treatment keeps patients alive longer)
- Prevalence decreases when: incidence ↓ OR patients recover/die quickly
Incidence vs Prevalence:
| Feature | Incidence | Prevalence |
|---|
| Cases | New only | Old + New |
| Time element | Yes | No (ratio) |
| Best for | Acute diseases, aetiology | Chronic diseases, planning |
| Use | Identifying risk factors | Manpower/bed planning |
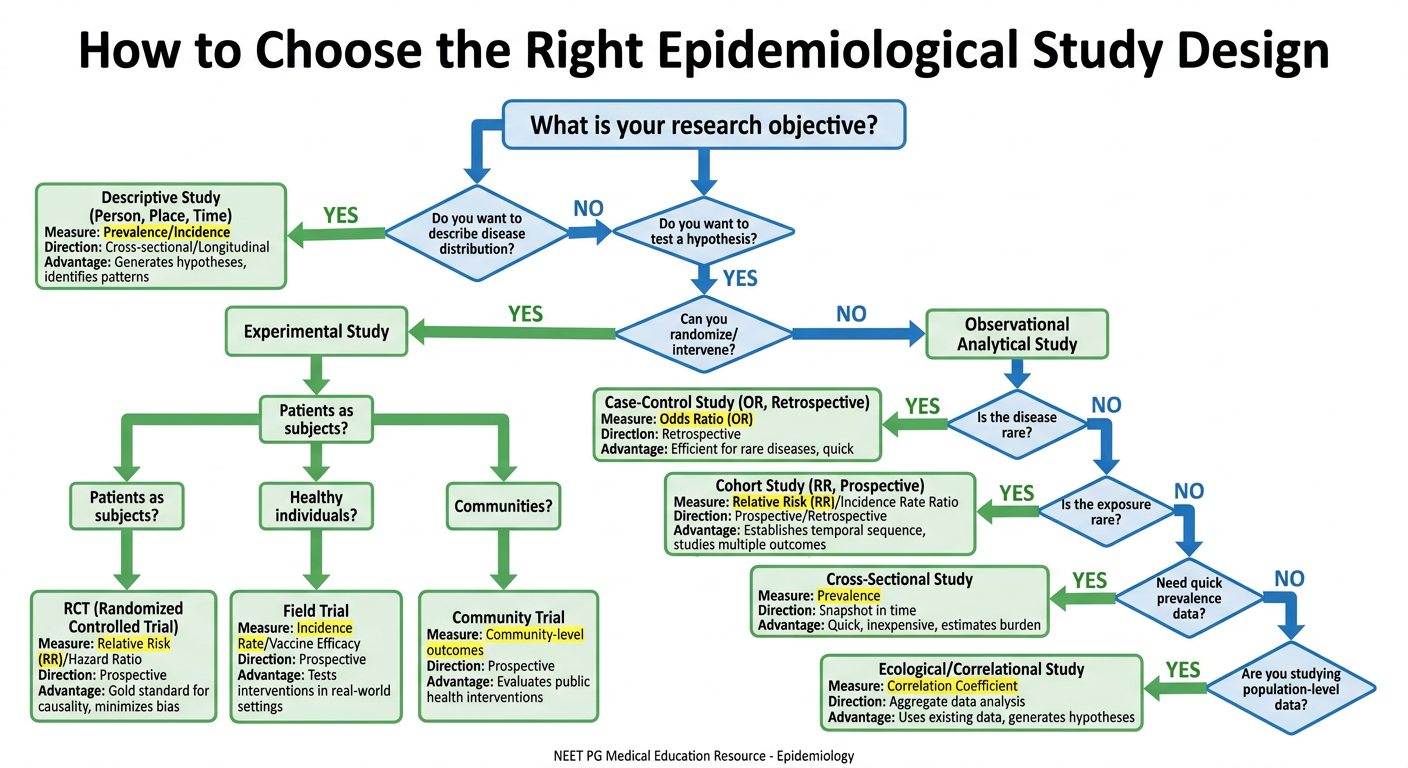
5. EPIDEMIOLOGICAL METHODS (Study Designs)
Epidemiological Studies
├── Observational
│ ├── Descriptive
│ └── Analytical
│ ├── Ecological/Correlational (unit = population)
│ ├── Cross-sectional/Prevalence (unit = individual)
│ ├── Case-control/Retrospective (unit = individual)
│ └── Cohort/Follow-up (unit = individual)
└── Experimental (Intervention)
├── Randomized Controlled Trial (unit = patients)
├── Field Trial (unit = healthy individuals)
└── Community Trial (unit = communities)
A. DESCRIPTIVE EPIDEMIOLOGY
Studies disease distribution by Person, Place, Time (PPT).
- Person: Age, sex, race, occupation, marital status, habits
- Place: Country, urban/rural, geographic distribution
- Time: Secular trends, cyclic changes, seasonal variation, point epidemics
Uses:
- Provides clues for formulating aetiological hypotheses
- Describes variation in disease by time, place, person
- Provides background data for planning health services
- Contributes to research
B. CASE-CONTROL STUDY (Retrospective Study)
Direction: Starts from effect → cause (backward)
Design: Select CASES (with disease) and CONTROLS (without disease) → look backward for exposure
2×2 Table:
| Cases (Disease +) | Controls (Disease -) |
|---|
| Exposed | a | b |
| Not Exposed | c | d |
Measure of association: Odds Ratio (OR)
$$\text{OR} = \frac{ad}{bc}$$
OR Interpretation:
- OR = 1 → No association
- OR > 1 → Positive association (risk factor)
- OR < 1 → Protective factor
Uses OR because you cannot calculate incidence from case-control studies (sample not representative of whole population).
Selection of Controls:
- Hospital controls (risk: Berkesonian bias)
- Relatives (siblings unsuitable for genetic studies)
- Neighbourhood controls
- General population controls
Biases in Case-Control:
- Recall/Memory bias - Cases remember exposures better than controls
- Selection bias - Cases/controls not representative of population
- Berkesonian bias - Different hospital admission rates for different diseases
- Interviewer bias - Eliminated by double-blinding
- Confounding bias - Third variable related to both exposure and disease
Advantages:
- Quick, inexpensive
- Good for rare diseases and chronic diseases
- Can study multiple exposures for one disease
- Small sample needed
Disadvantages:
- Recall bias
- Selection of appropriate controls is difficult
- Cannot calculate incidence or relative risk directly
- Not suitable for rare exposures
C. COHORT STUDY (Prospective/Follow-up Study)
Direction: Starts from cause → effect (forward)
Design: Select exposed and non-exposed persons (free of disease) → follow up → observe who develops disease
Framework:
| Disease + | Disease - | Total |
|---|
| Exposed | a | b | a+b |
| Non-Exposed | c | d | c+d |
Measure of association: Relative Risk (RR)
$$\text{RR} = \frac{\text{Incidence in exposed}}{\text{Incidence in non-exposed}} = \frac{a/(a+b)}{c/(c+d)}$$
Attributable Risk (AR):
$$\text{AR} = \text{Incidence (exposed)} - \text{Incidence (non-exposed)}$$
Attributable Risk %:
$$\text{AR%} = \frac{I_E - I_{NE}}{I_E} \times 100$$
Population Attributable Risk (PAR):
$$\text{PAR} = \text{Incidence (total population)} - \text{Incidence (non-exposed)}$$
Types of Cohort Studies:
- Prospective (concurrent): Exposure status identified now, followed into future (most common)
- Retrospective (historical/non-concurrent): Both exposure and disease occurred in past; data from records
Advantages:
- Can calculate incidence and RR directly
- Establishes temporal sequence (cause before effect)
- Can study multiple outcomes from one exposure
- No recall bias
- Best for common exposures
Disadvantages:
- Expensive and time-consuming
- Loss to follow-up (attrition bias)
- Not suitable for rare diseases
- Changes may occur in study population over time
COMPARISON: Case-Control vs Cohort
| Feature | Case-Control | Cohort |
|---|
| Direction | Retrospective (effect→cause) | Prospective (cause→effect) |
| Starts with | Disease status | Exposure status |
| Measure | Odds Ratio (OR) | Relative Risk (RR) |
| Rare disease | Yes | No |
| Rare exposure | No | Yes |
| Time/Cost | Short/Cheap | Long/Expensive |
| Incidence | Cannot calculate | Can calculate |
| Bias | Recall, Berkesonian | Attrition/loss to follow-up |
| Best example | Cancer + carcinogen | Framingham Heart Study |
D. RANDOMIZED CONTROLLED TRIAL (RCT)
- Gold standard experimental study
- Patients randomized into experimental and control groups
- Investigator manipulates an intervention
Steps:
- Draw up a protocol
- Select reference and experimental populations
- Randomization
- Manipulation/intervention
- Follow-up
- Assessment of outcome
Blinding:
- Single blind - Only patient is unaware of group allocation
- Double blind - Both patient and investigator are unaware (eliminates interviewer and patient bias)
- Triple blind - Patient, investigator, and data analyst are unaware
Crossover trial: Each subject acts as own control - both treatments given, separated by washout period.
6. RELATIVE RISK vs ODDS RATIO
| Measure | Study | Formula | When OR ≈ RR |
|---|
| RR (Relative Risk) | Cohort | Incidence(exposed) / Incidence(non-exposed) | - |
| OR (Odds Ratio) | Case-control | ad/bc | When disease is rare (<10%) |
- RR = 1 → No association
- RR > 1 → Positive association
- RR < 1 → Protective (e.g., vaccine)
7. ASSOCIATION AND CAUSATION (Bradford Hill Criteria)
Types of association:
- Spurious association - Due to bias/chance (e.g., hospital perinatal mortality paradox)
- Indirect association - Due to confounding variable
- Direct/Causal association - True cause-effect relationship
Bradford Hill's Criteria for Causation (9 Criteria):
| # | Criterion | Meaning |
|---|
| 1 | Temporal association | Cause must precede effect - most important/essential |
| 2 | Strength of association | Higher RR = stronger evidence |
| 3 | Dose-response | More exposure → more disease |
| 4 | Consistency | Same finding in different populations/settings |
| 5 | Specificity | One cause → one disease |
| 6 | Biological plausibility | Makes biological sense |
| 7 | Coherence | Does not conflict with known facts |
| 8 | Experimental evidence | Removal of factor reduces disease |
| 9 | Analogy | Similar associations exist elsewhere |
Mnemonic: Truly Strong Dose Consistently Specific Biology Coherently Experiments Analogize = TS-DC-SB-CEA
Only temporal association is ESSENTIAL. The others support causation but none is individually sufficient.
8. SCREENING
Definition (WHO): "The presumptive identification of unrecognized disease or defect by means of tests, examinations or other procedures which can be applied rapidly."
Screening vs Diagnostic Test:
| Feature | Screening | Diagnostic |
|---|
| Applied to | Apparently healthy | Sick/symptomatic |
| Applied in | Groups | Individual patients |
| Cost | Less expensive | More expensive |
| Accuracy | Less accurate | More accurate |
| Basis for treatment | No | Yes |
| Initiative | From investigator | From patient |
Validity of Screening Test:
Using 2×2 table (Disease = Gold Standard):
| Disease + | Disease - |
|---|
| Test + | TP (a) | FP (b) |
| Test - | FN (c) | TN (d) |
$$\text{Sensitivity} = \frac{a}{a+c} \times 100 \quad (\text{True Positives / All with disease})$$
$$\text{Specificity} = \frac{d}{b+d} \times 100 \quad (\text{True Negatives / All without disease})$$
$$\text{PPV} = \frac{a}{a+b} \times 100 \quad (\text{True Positives / All positive tests})$$
$$\text{NPV} = \frac{d}{c+d} \times 100 \quad (\text{True Negatives / All negative tests})$$
Key relationships:
- Sensitivity and specificity are inversely related
- High sensitivity = Few false negatives (good for ruling OUT disease - SnNOUT)
- High specificity = Few false positives (good for ruling IN disease - SpPIN)
- PPV and NPV depend on prevalence of disease
- Sensitivity and specificity are independent of prevalence
Lead time: The period between detection by screening and usual clinical presentation. Screening benefit must exceed lead time bias.
9. HERD IMMUNITY
Definition: The resistance of a group/community to invasion and spread of an infectious agent, based on the immunity of a high proportion of members.
$$\text{Herd Immunity Threshold (HIT)} = 1 - \frac{1}{R_0}$$
- R₀ = Basic reproduction number (average cases generated by one case)
- Higher R₀ → Higher HIT needed
| Disease | R₀ | HIT Required |
|---|
| Measles | 12-18 | 92-95% |
| Polio | 5-7 | 80-85% |
| Smallpox | 5-7 | 80-85% |
| COVID-19 | 2-3 | 50-67% |
10. GENERATION TIME vs SERIAL INTERVAL
- Generation time: Time interval between receipt of infection by a host and maximal infectivity of that host
- Serial interval: Time between onset of symptoms in primary case and onset in secondary case
- Incubation period: Time between exposure and onset of symptoms
11. QUICK REVISION TABLE: Study Designs
| Study | Type | Direction | Measure | Rare Disease | Time |
|---|
| Cross-sectional | Observational | No time element | Prevalence | No | Quickest |
| Ecological | Observational | Population level | Correlation | - | Quick |
| Case-control | Analytical | Retrospective | OR | Yes | Short |
| Cohort | Analytical | Prospective | RR, AR | No | Long |
| RCT | Experimental | Prospective | RR | No | Long |
| Field trial | Experimental | Prospective | - | No | Long |
12. HIGH-YIELD NEET PG ONE-LINERS
- Epidemiology unit of study = Defined population (not individual)
- Incidence = NEW cases; requires time in expression
- Prevalence = ALL current cases; is a ratio (not a rate)
- P = I × D (Prevalence = Incidence × Duration)
- Attack rate = Incidence during epidemic (%)
- SAR excludes primary case from denominator
- OR used in case-control studies; RR in cohort studies
- OR ≈ RR when disease is rare (<10%)
- Bradford Hill - temporal association is the only essential criterion
- Recall bias is the main bias of case-control studies
- Attrition/loss to follow-up is main problem in cohort studies
- Berkesonian bias = hospital admission rate bias in case-control
- Sensitivity = detects true cases = rules OUT disease (SnNOUT)
- Specificity = detects true non-cases = rules IN disease (SpPIN)
- PPV and NPV depend on prevalence; sensitivity and specificity do not
- Framingham study = most famous prospective cohort study
- RCT = gold standard for intervention/therapy evaluation
- Double blind RCT = eliminates interviewer + patient bias
- Screening is not a diagnostic test; just an initial examination
- Lead time = period gained by early detection through screening
- Herd immunity - Measles requires highest coverage (~95%)
- Web of causation = MacMahon's model for multifactorial disease
- Ecological fallacy = applying group-level findings to individuals
- Cross-sectional study = cannot establish temporal association (chicken-and-egg problem)
- Field trial = experimental study in healthy individuals (e.g., vaccine trials)
Source: Park's Textbook of Preventive and Social Medicine, 24th Edition
This covers all the core epidemiology topics tested in NEET PG/NEXT. Focus especially on:
- Study design comparison (very frequently tested)
- OR vs RR formulas and interpretation
- Sensitivity/specificity/PPV/NPV calculations
- Bradford Hill criteria (temporal association = essential)
- Incidence vs Prevalence relationship
- Types of bias in each study design