

It's a ayurvedic topic of vega dharnam but in given image can you teach me in simple and detailed physiology and patho of urine suppression that i provide you
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Finding Sources
Reading File
I now have comprehensive information from Guyton & Hall, Costanzo, and Brenner & Rector. Let me compile a thorough, simple explanation.
Mootra Vega Dharana — Physiology & Pathology of Urine Suppression
Your notes cover Micturation (micturition) under the Ayurvedic concept of Vega Dharana (suppression of natural urges). Here is a complete, simple explanation of the physiology and pathology.
🧠 PART 1: NORMAL PHYSIOLOGY OF URINATION (Micturation)
How the Bladder Fills — Storage Phase
Think of the bladder like a balloon with a controlled valve.
| Phase | What Happens | Nerve Controlling It |
|---|---|---|
| Filling | Detrusor muscle relaxes | Sympathetic (L1–L3) via β₂ receptors |
| Filling | Internal sphincter contracts (stays closed) | Sympathetic (L1–L3) via α₁ receptors |
| Filling | External sphincter contracts voluntarily | Voluntary (pudendal nerve, S2–S4) |
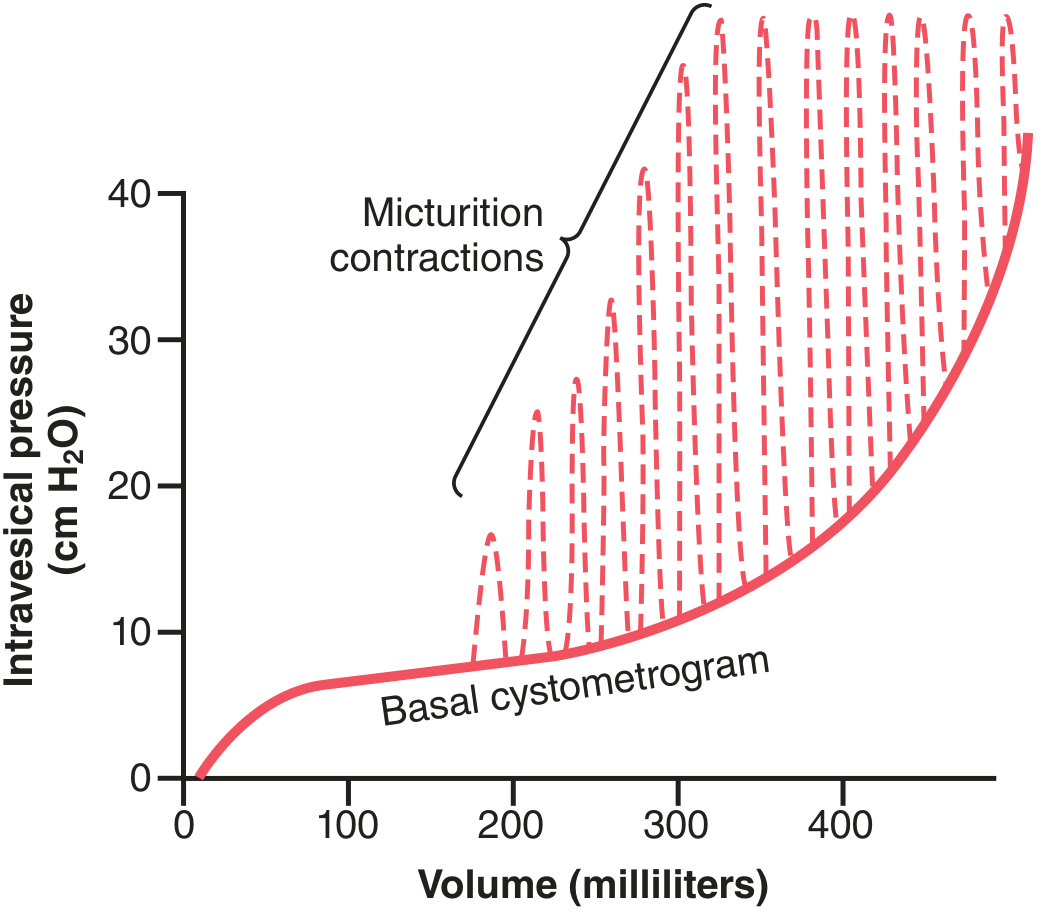
- Kidneys produce ~1.5–2 L of urine per day
- An empty bladder has ~0 cm H₂O pressure
- At 30–50 mL: pressure rises to 5–10 cm H₂O
- At 200–300 mL: pressure stays relatively flat (bladder wall is compliant)
- Beyond 300–400 mL: pressure rises sharply
The Micturition Reflex — How Urge Begins
Step-by-step reflex arc:
Bladder fills beyond ~200–300 mL
↓
Stretch receptors in bladder wall + posterior urethra activated
↓
Afferent signals travel via PELVIC NERVES → Sacral spinal cord (S2–S4)
↓
Parasympathetic efferent signals return → Detrusor muscle CONTRACTS
↓
Self-regenerating cycle: contraction → more stretch → more contraction
↓
Signal sent to PONS (pontine micturition center) + cerebral cortex
↓
"Urge to urinate" perceived consciously
This is a spinal cord autonomic reflex but is modified by higher brain centers (pons, cerebral cortex).
Role of Higher Brain Centers
Your notes say: "Reflex of micturation occurs in the spinal cord and modified by higher centers like pons and cerebrum of brain."
| Brain Center | Role |
|---|---|
| Cerebral cortex | Mainly inhibitory — keeps reflex suppressed until appropriate time |
| Pons (pontine micturition center) | Strong facilitatory center — coordinates actual voiding |
| Hypothalamus | Modulates urge perception |
In simple words: Your spinal cord says "bladder is full, let it go." Your brain says "not yet, wait." This is exactly Vega Dharana — the voluntary cortical inhibition of a natural reflex.
Voluntary Urination — How it Actually Happens
- You voluntarily contract abdominal muscles → raises bladder pressure
- Urine enters the bladder neck and posterior urethra → stretches walls
- This fires stretch receptors → triggers full micturition reflex
- Simultaneously, cortex inhibits the external sphincter → urine flows out
- Bladder normally empties completely — only 5–10 mL residual urine remains
⚠️ PART 2: PATHOPHYSIOLOGY OF URINE SUPPRESSION (Mootra Vega Dharana)
Your notes describe consequences of holding urine. Here is the modern physiological explanation:
What happens when you voluntarily suppress the urge?
When you repeatedly ignore the urge to urinate:
Short-term (habitual holding):
- The pontine micturition center receives constant inhibitory signals from the cortex
- External sphincter remains contracted (voluntary tonic contraction)
- The micturition reflex fires but gets overridden and fatigued
- The bladder continues to fill → intravesical pressure increases sharply
Long-term (structural problems):
Your notes mention: "Structural problems are like increased bladder pressure which results in retrograde pressure to kidneys." This maps exactly to what happens:
Habitual urine suppression
↓
Bladder overdistension (>400–500 mL)
↓
Intravesical pressure rises dramatically
↓
Retrograde pressure transmitted BACKWARDS:
Bladder → Ureter → Renal Pelvis → Kidney
↓
HYDRONEPHROSIS (dilation of renal pelvis and calyces)
↓
Compression of renal parenchyma → Reduced GFR
↓
Obstructive nephropathy → Irreversible kidney damage if prolonged
"Any obstruction of urinary flow at any point may cause retention of urine and increased retrograde hydrostatic pressure, leading to kidney damage and interference with waste and water excretion." — Brenner & Rector's The Kidney
Functional Problems (also mentioned in your notes)
Your notes mention: "Functional problems: Altered filtration"
| Consequence | Mechanism |
|---|---|
| Reduced GFR | Back pressure opposes glomerular filtration pressure |
| Impaired concentration/dilution | Tubular transporter proteins (Na⁺, H⁺, HCO₃⁻ transporters) are downregulated |
| Azotemia | Waste products accumulate when GFR drops |
| Electrolyte imbalance | Na⁺, K⁺, acid-base disturbances |
| Dysuria / pain | Overdistended bladder triggers pain fibers |
| Headache | Raised intra-abdominal/pelvic pressure, autonomic response |
The Two Types of Problems (Your Notes: Point 1 & 2)
Your notes state two problems from suppressing micturition — here is the physiology:
1. Structural problems (anatomical):
- Bladder wall overdistension → loss of smooth muscle elasticity
- Chronic back-pressure → hydronephrosis → cortical atrophy of kidney
- Ureteric reflux — urine flows backward into ureters
2. Functional problems (physiological):
- Loss of bladder wall compliance (becomes stiff)
- Detrusor overactivity or underactivity
- Altered albumin clearance (proteinuria from glomerular damage)
- Loss of blood proteins in urine (mentioned in your notes: "dysuria, headache, pain in bladder & sides, increased albumin clearance and loss of blood proteins")
🔄 Summary Flow Chart
Normal Urge → Cortical Inhibition → Vega Dharana (Suppression)
↓
Bladder overdistends chronically
┌──────────────┴───────────────┐
STRUCTURAL FUNCTIONAL
(Hydronephrosis, (Reduced GFR, impaired
ureteric dilation, concentration, azotemia,
renal cortical atrophy) electrolyte disturbances)
└──────────────┬───────────────┘
↓
Irreversible kidney damage
if not treated promptly
🔑 Key Points to Remember for Exams
| Aspect | Key Fact |
|---|---|
| Filling nerve | Sympathetic (L1–L3) → relaxes detrusor, closes sphincter |
| Voiding nerve | Parasympathetic (S2–S4) → contracts detrusor, opens sphincter |
| Reflex center | Sacral cord (S2–S4) |
| Higher control | Pons (facilitates), Cerebral cortex (inhibits) |
| Voluntary control | External sphincter via pudendal nerve |
| Suppression → structural | Hydronephrosis, back pressure, renal atrophy |
| Suppression → functional | Reduced GFR, azotemia, electrolyte imbalance |
| Normal adult capacity | 400 mL (your notes confirm this) |
| Residual urine normally | 5–10 mL |
Sources: Guyton & Hall Textbook of Medical Physiology; Costanzo Physiology 7th ed.; Brenner & Rector's The Kidney
Create a summary document comparing Ayurvedic Vega Dharana with modern urology
Asking for Preferences
Reading File
Running Command
Running Command
Writing File
Running Command
Running Command
Your PDF is ready:
Mootra Vega Dharana vs Modern Urology
PDF Document · PDF
Here's what's inside the document (7 sections, study notes format):
| Section | Content |
|---|---|
| 1. What is Vega Dharana | Ayurvedic definition + symptom table mapping Sanskrit terms to modern equivalents |
| 2. Normal Physiology | Filling/voiding phases, reflex arc steps, brain centers table |
| 3. Pathophysiology | Cascade of structural (hydronephrosis) and functional (GFR, azotemia) damage |
| 4. Side-by-Side Comparison | 12-row table — every key aspect compared Ayurveda vs. Modern |
| 5. Apana Vata vs. ANS | Deep parallel between Apana Vata and pelvic autonomic nervous system |
| 6. Exam Flash Points | 16 quick Q&A points for revision |
| 7. Pathology Flowchart + References | Visual flow from suppression → renal damage, with full citations |
This is a shared conversation. Sign in to Orris to start your own chat.