I now have all the content needed. Let me compile the complete, comprehensive answer:
LIVER PATHOLOGY - MUHS 2nd MBBS EXAM NOTES
(Harsh Mohan Textbook of Pathology, Chapter 19)
1. JAUNDICE - Definition, Classification & Causes
DEFINITION:
Jaundice (Icterus) = Yellow discoloration of skin, sclerae, and mucous membranes due to deposition of bilirubin secondary to raised bilirubin levels in blood (>1.5 mg/dL clinically apparent; normal total serum bilirubin = 0.2–1.0 mg/dL).
Latent/Pre-jaundice: Bilirubin 1.0–1.5 mg/dL - not clinically visible
Frank jaundice: Bilirubin >1.5–2.0 mg/dL - visible yellowing
BILIRUBIN METABOLISM (Quick Review - Draw in Exam):
Senescent RBCs (120 days)
↓ Reticuloendothelial System (spleen, liver, bone marrow)
Haemoglobin → Heme + Globin
Heme → Biliverdin → UNCONJUGATED BILIRUBIN (indirect, fat-soluble)
↓ binds albumin in blood
Liver: uptake → conjugation with glucuronic acid (UDP-glucuronosyltransferase)
↓
CONJUGATED BILIRUBIN (direct, water-soluble)
↓ excreted into bile canaliculi → bile → duodenum
In gut: bacteria → UROBILINOGEN
↓ reabsorbed → enterohepatic circulation → re-excreted in bile
↓ ~5% reaches kidneys → excreted as UROBILIN (in urine)
In colon: → STERCOBILINOGEN/STERCOBILIN → excreted in stool (brown color)
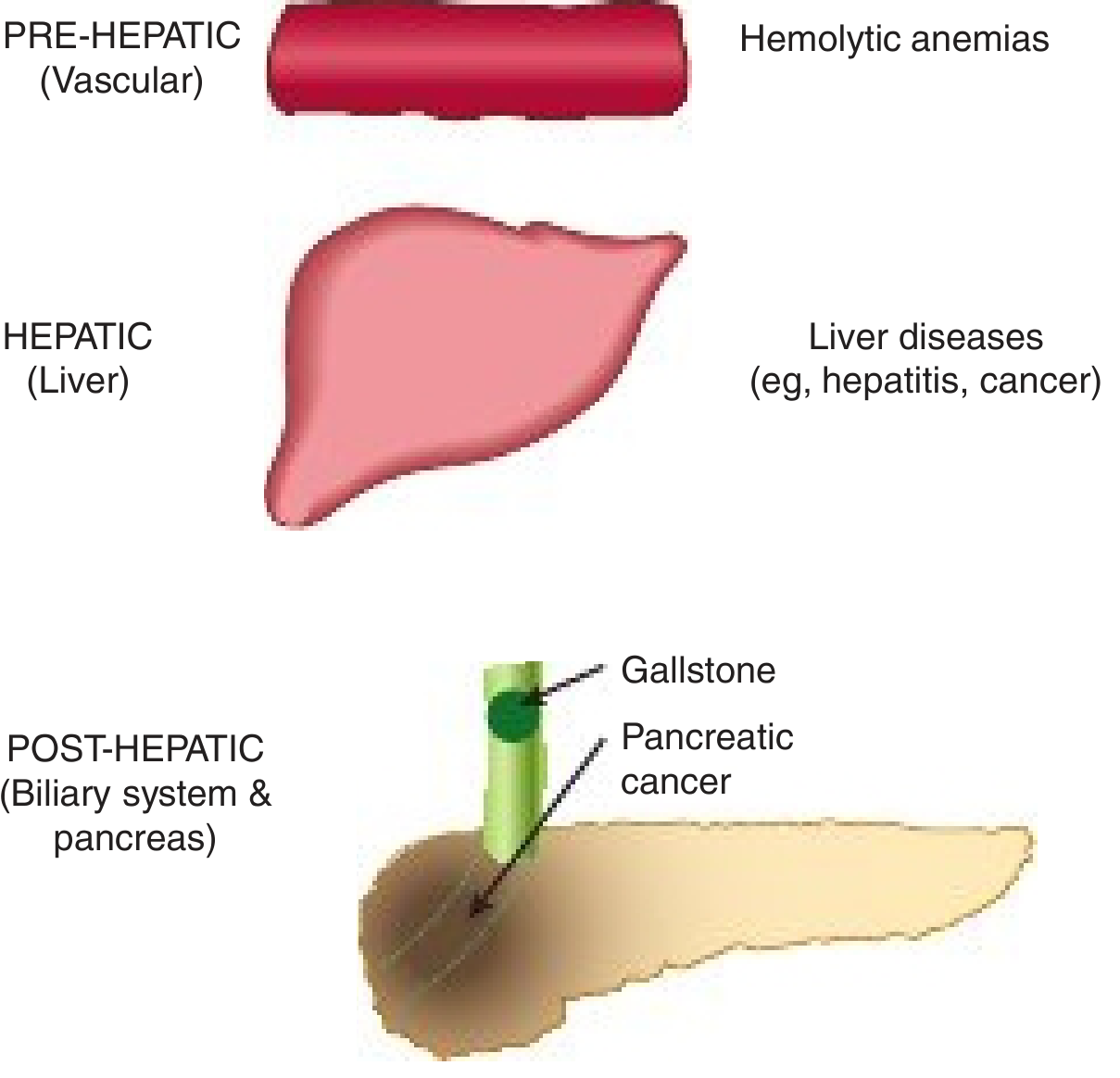
CLASSIFICATION OF JAUNDICE:
Classification of jaundice by level: Pre-hepatic, Hepatic, Post-hepatic (Harper's Illustrated Biochemistry)
Harsh Mohan classifies jaundice into 3 types:
TYPE 1: HEMOLYTIC (PRE-HEPATIC) JAUNDICE
- Unconjugated (indirect) hyperbilirubinemia
- Liver function intact, but overwhelmed by excessive bilirubin load
Causes:
- Congenital hemolytic anemias: Hereditary spherocytosis, Sickle cell disease, Thalassemia, G6PD deficiency
- Acquired hemolytic anemias: Autoimmune hemolytic anemia, Malaria, Blackwater fever, Mismatched blood transfusion
- Neonatal jaundice (physiological and pathological)
- Ineffective erythropoiesis (Megaloblastic anemia, Thalassemia)
TYPE 2: HEPATOCELLULAR (HEPATIC) JAUNDICE
- Both conjugated + unconjugated elevated (mixed)
- Primary liver cell damage
Causes:
| Subtype | Examples |
|---|
| Infective | Viral hepatitis (A, B, C, D, E), Infectious mononucleosis, Leptospirosis, Malaria |
| Toxic/Drug | Alcohol, Paracetamol, Isoniazid, Halothane, CCl₄, Amanita mushroom |
| Metabolic | Wilson's disease, Haemochromatosis, α1-antitrypsin deficiency |
| Autoimmune | Autoimmune hepatitis |
| Intrahepatic cholestasis | Intrahepatic cholestasis of pregnancy, Drug-induced (e.g., chlorpromazine) |
| Cirrhosis | End-stage liver disease |
TYPE 3: OBSTRUCTIVE (POST-HEPATIC/CHOLESTATIC) JAUNDICE
- Conjugated (direct) hyperbilirubinemia
- Impaired excretion of bile
Causes:
| Level | Causes |
|---|
| Intrahepatic | Primary biliary cirrhosis, Primary sclerosing cholangitis, Intrahepatic cholestasis |
| Extrahepatic | Choledocholithiasis (gallstone in CBD), Carcinoma head of pancreas, Cholangiocarcinoma, Stricture of CBD, Chronic pancreatitis, External compression by lymph nodes |
LABORATORY DIAGNOSIS OF OBSTRUCTIVE JAUNDICE:
| Investigation | Finding | Mechanism |
|---|
| Serum total bilirubin | ↑↑↑ (may be >20 mg/dL) | Regurgitation of conjugated bilirubin |
| Serum direct (conjugated) bilirubin | ↑↑↑ (predominantly) | Conjugated bilirubin regurgitates |
| Serum indirect bilirubin | Normal or mildly ↑ | Conjugation intact |
| Urine bilirubin (bilirubinuria) | Present (3+/4+) | Conjugated is water-soluble, filtered by kidneys |
| Urine color | Dark yellow/tea-colored | Bilirubinuria |
| Foam test | Yellow foam (Gmelin's test +) | Bilirubin in urine |
| Urine urobilinogen | ABSENT | No bile reaches intestine → no urobilinogen formed |
| Stool color | Clay/Pale/Acholic | No stercobilinogen (absent bile in gut) |
| Serum ALP | ↑↑↑ (markedly raised) | Induced by biliary epithelium under cholestatic pressure |
| Serum GGT | ↑↑↑ | Confirms biliary origin of raised ALP |
| 5'-Nucleotidase | ↑ | Biliary marker |
| Serum ALT/AST | Normal or mildly ↑ | No primary hepatocyte necrosis (early) |
| Serum cholesterol | ↑↑ | Impaired biliary excretion; Lipoprotein X appears |
| Serum bile acids | ↑↑↑ | Retention (cause pruritus) |
| Prothrombin time (PT) | Prolonged | Vit K malabsorption (fat-soluble, needs bile) |
| PT corrects with IV Vit K? | YES - corrects within 24-48 h | Distinguishes from hepatocellular failure |
| Serum proteins | Normal early | Liver cells not primarily damaged |
Causes of raised ALP in obstructive jaundice: Bile acids act as detergents on liver cell membranes, releasing ALP. Also, ALP synthesis by biliary epithelium is induced by bile acid accumulation.
LABORATORY APPROACH IN A CASE OF JAUNDICE (Stepwise):
Step 1: Is it hemolytic, hepatocellular or obstructive?
| Parameter | Hemolytic | Hepatocellular | Obstructive |
|---|
| Serum bilirubin | ↑ Indirect | ↑ Both | ↑ Direct |
| Urine bilirubin | Absent | Present | Present |
| Urine urobilinogen | ↑↑↑ | Variable | Absent |
| Stool color | Dark | Pale | Clay-colored |
| AST/ALT | Normal | ↑↑↑ | Normal/mild ↑ |
| ALP | Normal | ↑ | ↑↑↑ |
| PT | Normal | Prolonged (NO Vit K correction) | Prolonged (Vit K corrects) |
| Blood picture | Anemia, reticulocytosis | Normal | Normal |
Step 2: Further investigations based on type:
- Hemolytic: PBS (peripheral blood smear), Hb electrophoresis, Coombs test, osmotic fragility, G6PD levels
- Hepatocellular: Liver biopsy, viral serology (HBsAg, Anti-HCV), autoimmune markers (ANA, ASMA), serum ceruloplasmin, α1-AT levels, LFTs
- Obstructive: USG abdomen (dilated CBD, gallstone, mass), MRCP, ERCP, CT scan, tumor markers (CA 19-9, CEA for cholangiocarcinoma; AFP for HCC)
2. ALCOHOLIC LIVER DISEASE (ALD)
PATHOGENESIS (MOST IMPORTANT FOR MUHS):
Alcohol (ethanol) is metabolized primarily in the liver by three pathways:
1. Alcohol Dehydrogenase (ADH) pathway - main route at low-moderate doses
2. Microsomal Ethanol Oxidizing System (MEOS) - CYP2E1 - induced at high doses
3. Catalase - minor role
ETHANOL → (ADH/MEOS) → ACETALDEHYDE → (Acetaldehyde DH) → ACETATE
Key Biochemical Disturbance: ↑ NADH : NAD+ Ratio
ALCOHOL OXIDATION
↓ ↑↑ NADH generated
┌─────────────────────────────────────────────────────┐
│ ↑ NADH : NAD+ ratio causes: │
│ 1. ↓ β-oxidation of fatty acids (needs NAD+) │
│ 2. ↑ Fatty acid synthesis │
│ 3. ↑ Esterification of FAs to triglycerides │
│ 4. ↓ Gluconeogenesis → hypoglycemia │
│ 5. ↑ Lactate → lactic acidosis │
└─────────────────────────────────────────────────────┘
↓
FAT ACCUMULATES IN HEPATOCYTES = FATTY LIVER
Direct toxic effects of Acetaldehyde:
- Inhibits microtubule function → impairs VLDL export from hepatocytes → fat retention
- Forms protein adducts → neo-antigens → immune-mediated hepatocyte damage
- Stimulates collagen synthesis by hepatic stellate cells → fibrosis
- Generates reactive oxygen species (ROS) → oxidative stress → lipid peroxidation → membrane damage
- Increases intestinal permeability → endotoxin (LPS) enters portal blood → Kupffer cell activation → release of TNF-α, IL-1, IL-6, IL-8 → hepatocyte apoptosis/necrosis
Six mechanisms of fat accumulation:
- ↑ Fatty acid synthesis
- ↓ Fatty acid β-oxidation
- ↑ Esterification to TG
- ↓ VLDL secretion (impaired apolipoprotein synthesis)
- ↑ Peripheral mobilization of fat from adipose tissue
- Direct toxic effect on mitochondrial function
MORPHOLOGY / HISTOLOGY OF ALD:
ALD presents as a SPECTRUM of three lesions (may co-exist):
A. ALCOHOLIC FATTY LIVER (Steatosis) - Most Common, Earliest
Gross:
- Liver enlarged (up to 4-6 kg; normal ~1.5 kg), soft, yellow, greasy
- Smooth surface, rounded edges
- Cut surface: yellow, oily appearance
- Reversible with abstinence
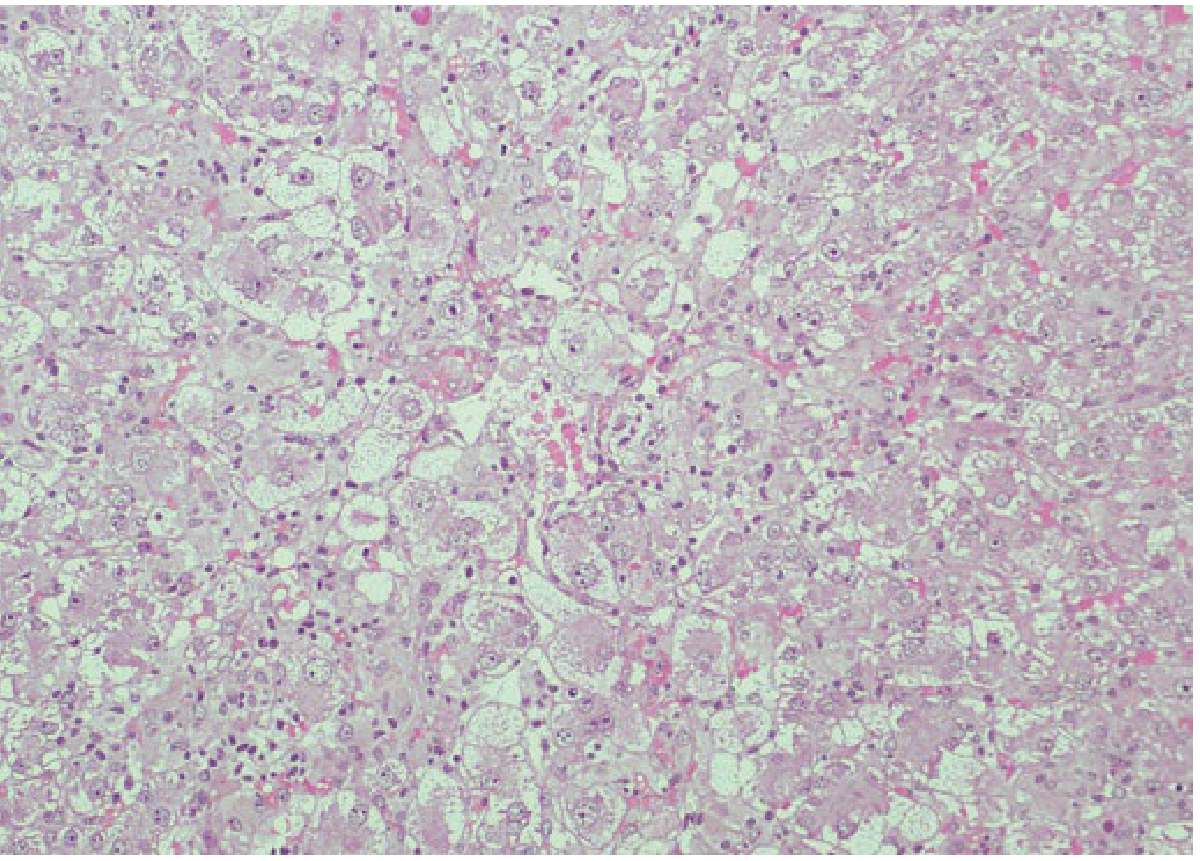
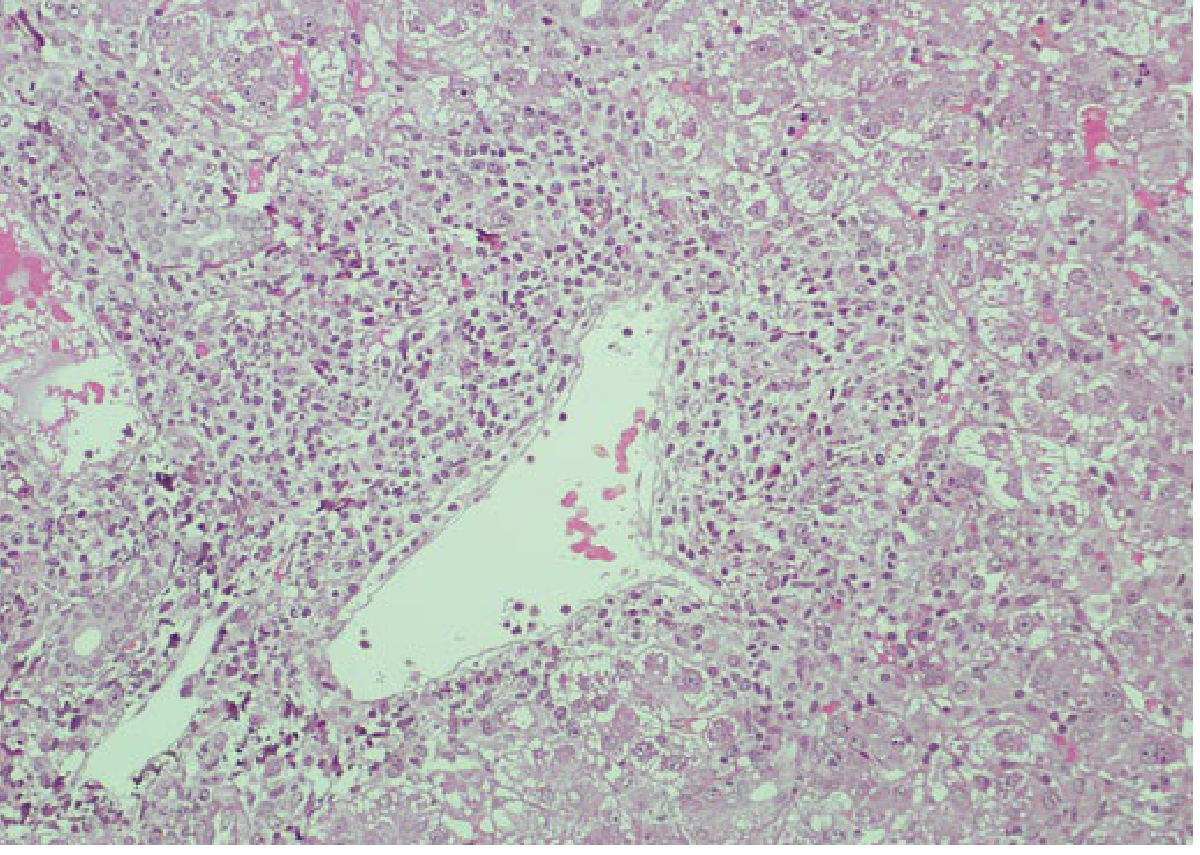
Microscopy (H&E):
- Macrovesicular steatosis: LARGE fat vacuoles push nucleus to periphery - "signet ring" hepatocytes
- Predominantly Zone 3 (centrilobular/perivenular) → with progression, entire lobule involved
- Occasional cholestasis and sinusoidal fibrosis
Special stain: Oil Red O (frozen section) for neutral fat - Orange-red droplets
B. ALCOHOLIC HEPATITIS - More Serious
Gross:
- Liver enlarged, tender, bile-stained (cholestasis)
- May have fine granular surface
Microscopy - The 5 Hallmarks (MUST MEMORIZE):
| Feature | Description |
|---|
| 1. Hepatocyte ballooning degeneration | Swollen hepatocytes with pale, clear, watery cytoplasm (most characteristic) |
| 2. Mallory-Denk bodies (Mallory's hyaline) | Eosinophilic, rope-like/spider-web cytoplasmic inclusions of ubiquitinated cytokeratin 8/18 intermediate filaments - PATHOGNOMONIC |
| 3. Neutrophilic satellitosis | Neutrophils surround hepatocytes with Mallory bodies (PMN infiltration) |
| 4. Hepatocyte necrosis | Zone 3 necrosis, hepatocyte dropout |
| 5. Perivenular/sinusoidal fibrosis | Collagen around central vein and in Space of Disse ("chicken wire" fibrosis) |
Additional features:
- Cholestasis (bile plugs in canaliculi)
- Giant mitochondria = eosinophilic round bodies = "cherry bodies" in perivenular cells
- Acute foamy fatty change (FFC): microvesicular fat variant with central nucleus (more severe)
- Portal tracts: neutrophilic infiltrate without bile duct orientation + "arachnoid fibrosis"
C. ALCOHOLIC CIRRHOSIS - Final, Irreversible Stage
Gross:
- Early: Liver enlarged, yellow-tan, uniform small nodules (<3 mm) = MICRONODULAR ("hobnail" surface)
- Late: Liver shrunken (may be 500-700 g), hard, irregular surface with larger nodules = MACRONODULAR (after abstinence, regeneration)
- Laennec's cirrhosis = classical term for alcoholic micronodular cirrhosis
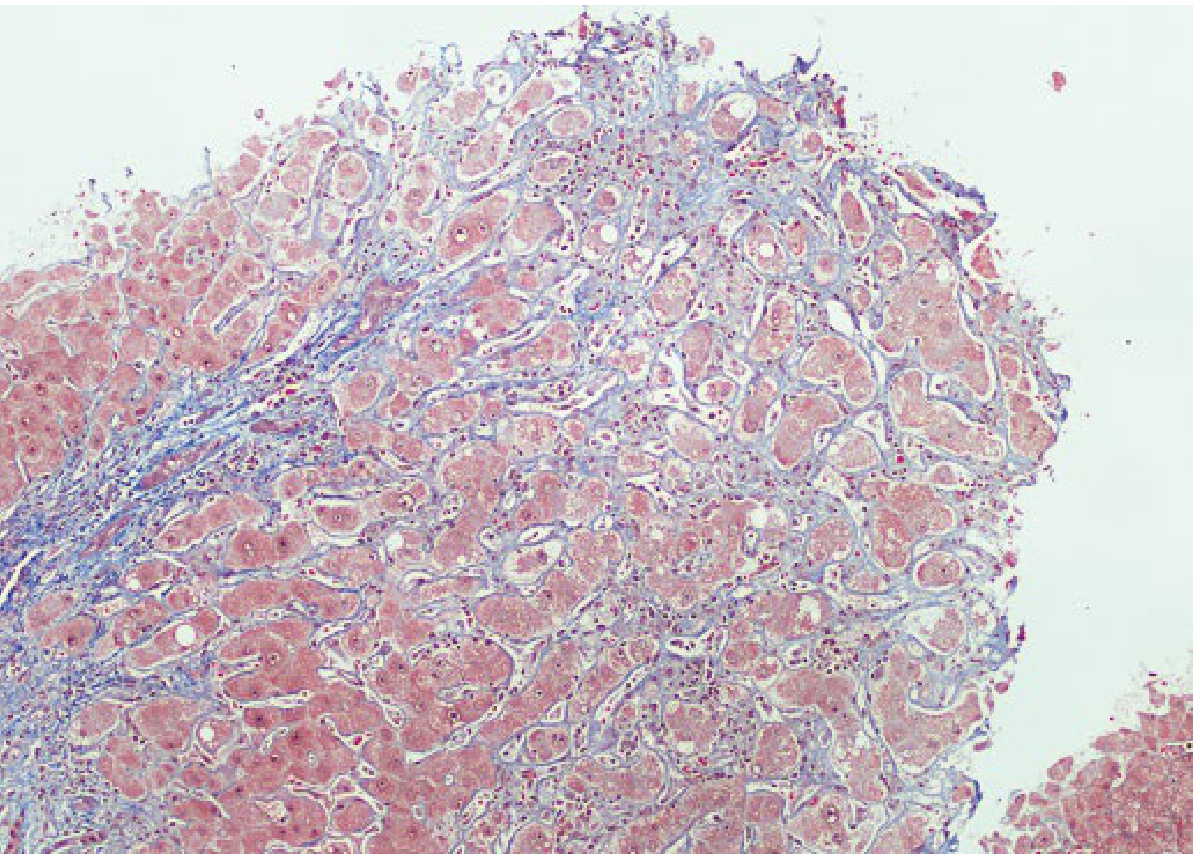
Microscopy:
Histopathology: Alcoholic cirrhosis - Masson trichrome stain. Blue = collagen fibers forming fibrous septa. Pink/red = regenerative nodules of hepatocytes. Note bridging fibrosis.
Three forms of fibrosis in ALD:
- Portal and perivenular fibrosis → fibrous septa formation → small regenerative nodules (= classic cirrhosis)
- Diffuse interstitial fibrosis - collagen encircles individual hepatocytes throughout lobule without regeneration or septae
- Progressive perivenular fibrosis - dense scar in Zone 3 with minimal portal fibrosis
Microscopic features of cirrhosis:
- Fibrous septa bridging portal tracts and central veins (porto-central and porto-portal bridges)
- Regenerative nodules - disorganized hepatocytes without normal lobular architecture
- Loss of central vein architecture
- Residual fat vacuoles, Mallory bodies (early)
- Bile ductule proliferation
- Inflammatory infiltrate (lymphocytes, plasma cells)
COMPLICATIONS OF ALD:
ALD COMPLICATIONS
├── Portal Hypertension
│ ├── Oesophageal/gastric varices (bleeding - lethal)
│ ├── Caput medusae
│ ├── Splenomegaly → hypersplenism
│ └── Ascites
├── Hepatic Encephalopathy (↑ ammonia, false neurotransmitters)
├── Hepatorenal Syndrome (functional renal failure)
├── Coagulopathy (↓ clotting factors, ↓ Vit K absorption)
├── Hypoalbuminaemia → oedema
├── Feminisation signs (↑ oestrogen: gynecomastia, spider naevi, palmar erythema)
├── Infections (SBP - spontaneous bacterial peritonitis)
└── Hepatocellular Carcinoma (HCC) - 3-6% of cirrhotic patients
3. CIRRHOSIS - Definition & Classification
(Harsh Mohan, Pg. 603)
DEFINITION (WHO/Harsh Mohan):
Cirrhosis is defined as a diffuse process characterized by fibrosis and conversion of normal liver architecture into structurally abnormal nodules (regenerative nodules) bounded by fibrous septa.
Key features of definition:
- Diffuse (whole liver involved)
- Fibrosis (irreversible collagen deposition)
- Regenerative nodules (disorganized hepatocyte proliferation)
- Distorted architecture (portal-systemic shunting)
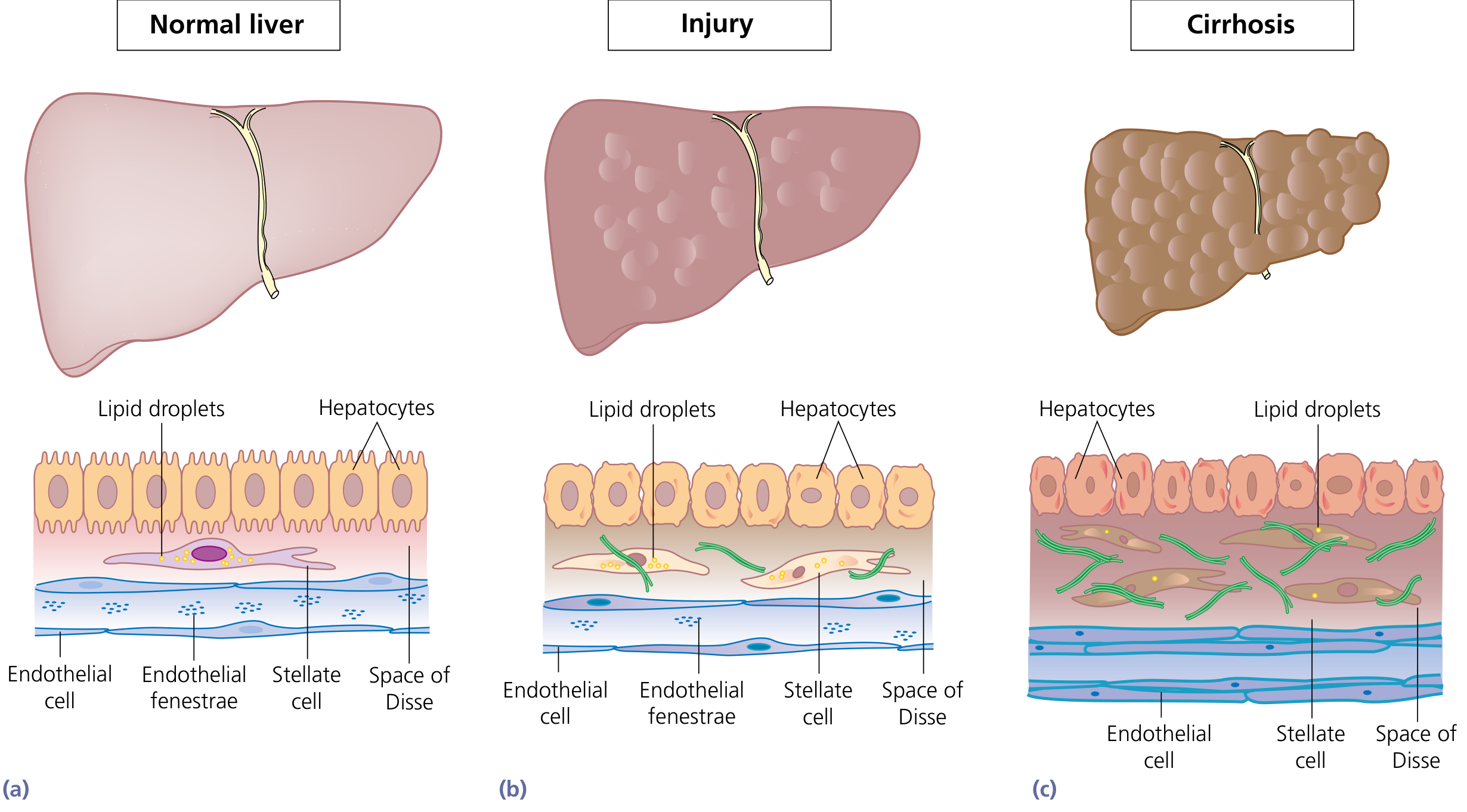
PATHOGENESIS OF CIRRHOSIS (Stellate Cell Activation):
Progression: Normal liver (a) → Injury with stellate cell activation (b) → Cirrhosis with dense collagen in Space of Disse, loss of endothelial fenestrae (c). Source: Yamada's Textbook of Gastroenterology
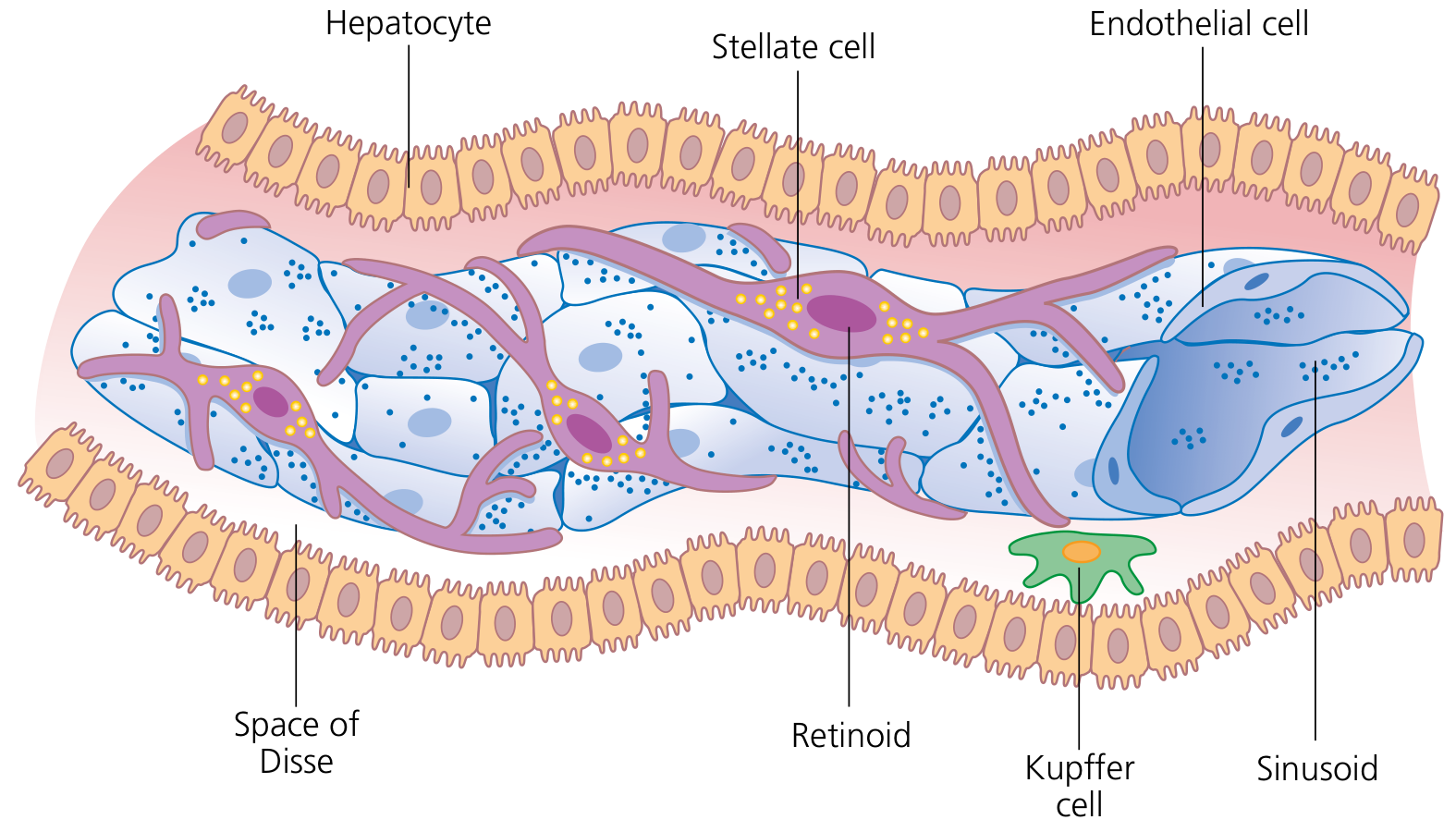
Cells of the hepatic sinusoid. Stellate cells (Ito cells) in Space of Disse store retinoids; upon activation they become myofibroblasts and produce collagen - key to fibrosis. Source: Yamada's Textbook of Gastroenterology
Mechanism of fibrosis:
- Chronic liver injury (any cause) → hepatocyte necrosis + inflammation
- Kupffer cell activation → release TNF-α, TGF-β1, PDGF
- Hepatic stellate cells (Ito cells) in Space of Disse ACTIVATED by TGF-β1
- Activated stellate cells → transform into myofibroblasts
- Myofibroblasts: ↑ collagen (type I, III) synthesis + ↓ MMP (matrix metalloproteinase) activity → net collagen deposition in Space of Disse
- Loss of endothelial fenestrae → impaired hepatocyte-blood exchange → liver dysfunction
- Stellate cell contraction → ↑ sinusoidal resistance → portal hypertension
- Progressive fibrosis → bridging fibrosis → cirrhosis
CLASSIFICATION OF CIRRHOSIS (Harsh Mohan):
A. MORPHOLOGICAL CLASSIFICATION:
| Type | Nodule Size | Causes |
|---|
| Micronodular (Laennec's/Portal) | Uniform nodules <3 mm | Alcohol (most common), biliary cirrhosis, haemochromatosis |
| Macronodular (Post-necrotic) | Irregular nodules >3 mm (up to several cm) | Viral hepatitis (HBV, HCV), Wilson's disease, α1-AT deficiency |
| Mixed | Both | Various |
Note: Micronodular cirrhosis can progress to macronodular with continued insult or abstinence (regeneration)
B. ETIOLOGICAL CLASSIFICATION (Harsh Mohan):
| Type | Etiology |
|---|
| Alcoholic cirrhosis | Chronic alcohol abuse |
| Post-necrotic (Post-hepatitic) cirrhosis | HBV, HCV, drugs, toxins |
| Biliary cirrhosis | Primary biliary cirrhosis (PBC), Primary sclerosing cholangitis (PSC), Biliary atresia |
| Pigment cirrhosis | Haemochromatosis |
| Cardiac cirrhosis | Chronic right heart failure → chronic venous congestion |
| Nutritional/Metabolic | Wilson's disease, α1-AT deficiency, Galactosaemia, Tyrosinaemia |
| Cryptogenic | No identifiable cause (~10%; many now = NASH) |
C. FUNCTIONAL CLASSIFICATION:
| Class | Based on |
|---|
| Compensated | No clinical symptoms; abnormal LFTs |
| Decompensated | Ascites, jaundice, encephalopathy, variceal bleed |
MORPHOLOGY OF CIRRHOSIS (General):
Gross:
- Small, shrunken (or occasionally enlarged early), hard liver
- Granular/nodular surface (nodules of varying size)
- Cut section: nodules surrounded by fibrous tissue
- Green tinge if cholestatic
Microscopy:
- Regenerative nodules - clusters of hepatocytes with altered lobular architecture
- Fibrous septa - collagen bands (stain blue with Masson trichrome) surrounding nodules
- Bridging fibrosis - porto-portal and porto-central bridges
- Bile ductule proliferation at margins of nodules (ductular reaction)
- Inflammatory infiltrate in fibrous septa
- Features of cause (e.g., Mallory bodies in ALD, ground-glass hepatocytes in HBV, iron deposits in haemochromatosis)
3. POST-NECROTIC CIRRHOSIS - Etiopathogenesis & Morphology
DEFINITION:
Post-necrotic cirrhosis (also called post-hepatitic cirrhosis or macronodular cirrhosis) develops following massive or submassive hepatic necrosis, where the necrotic areas are replaced by fibrous tissue with subsequent regeneration of surviving hepatocytes into irregular nodules of varying sizes.
ETIOPATHOGENESIS:
Causes (MUST KNOW):
| Cause | Details |
|---|
| Viral hepatitis - most common | HBV (most common worldwide; HBV+HDV co-infection = more severe), HCV (common in Western countries) |
| Drugs and toxins | INH (isoniazid), methyldopa, halothane, methotrexate, CCl₄, phosphorus |
| Autoimmune hepatitis | Hypergammaglobulinaemia, ANA/ASMA positive |
| Wilson's disease | Copper accumulation → hepatocyte necrosis |
| α1-Antitrypsin deficiency | Abnormal protein accumulation in hepatocytes |
| Cryptogenic | Previously idiopathic; many = NASH |
Mechanism:
MASSIVE / SUBMASSIVE / REPEATED EPISODES OF HEPATIC NECROSIS
↓
Collapse of reticulin framework
(necrotic hepatocytes removed by macrophages)
↓
Fibrous tissue replaces necrotic areas
(scar/fibrous collapse)
↓
Surviving hepatocytes regenerate
(but normal architecture is LOST)
↓
Irregular REGENERATIVE NODULES of varying sizes
surrounded by fibrous scars = MACRONODULAR CIRRHOSIS
↓
Portal-systemic shunting → Portal hypertension
Key Pathological Sequence:
- Hepatocyte necrosis (panacinar/submassive) → loss of liver cells
- Reticulin framework collapse → approximation of portal tracts and central veins
- Inflammatory response → lymphocytes, plasma cells, macrophages
- Stellate cell activation → fibroblast proliferation → collagen deposition in collapsed areas
- Attempted regeneration → irregular nodule formation (no scaffolding to guide regeneration)
- Architectural distortion → portal hypertension, liver failure
MORPHOLOGICAL FEATURES:
GROSS:
- Liver is shrunken, firm, irregular with coarsely nodular surface
- Nodules are LARGE and IRREGULAR in size and shape (>3 mm; can be 0.3 - 5+ cm)
- Nodules separated by broad, irregular fibrous scars/bands (the collapsed parenchyma)
- Cut section: irregular tan-brown nodules with dense white fibrous septa
- May show bile staining (green/yellow tinge) if cholestatic component present
- Capsule is thickened and irregular
- Liver weight: reduced (500–1000 g; normal 1500 g)
Gross Diagram to Draw:
POST-NECROTIC CIRRHOSIS - GROSS (Cut Surface)
┌─────────────────────────────────────────────┐
│ IRREGULAR, COARSELY NODULAR SURFACE │
│ │
│ ╔══════╗ ╔═══╗ ╔═══════╗ │
│ ║ LARGE║ ░░░ ║ ║░░░║ NODULE║ │
│ ║ NODE ║ ░░░ ╚═══╝░░░║ (var ║ │
│ ║ (>3mm║░░░░░░░░░░░░░░║ size) ║ │
│ ╚══════╝░░░░╔═════╗░░░╚═══════╝ │
│ ░░░░░║SMALL║░░░░░░░░░░░ │
│ ░░░░░╚═════╝░░░░░░░░░░░ │
│ │
│ ░░░ = Broad fibrous scar (collapsed parench)│
│ ╔══╗ = Regenerative nodule (varying sizes) │
└─────────────────────────────────────────────┘
- Nodules: irregular, large (0.3–5 cm)
- Scars: broad, irregular, dense
- Color: pale-tan (fibrous) + yellowish-brown (nodules)
MICROSCOPY:
Features (H&E):
-
Regenerative nodules - Large, irregular clusters of hepatocytes with:
- Disorganized hepatic plates (two cell-thick plates instead of one)
- No normal lobular architecture (central vein may be absent or eccentrically placed)
- Prominent hepatocyte regeneration (binucleate cells, mitotic figures)
-
Broad fibrous septa (broader than in alcoholic micronodular):
- Dense collagen (stains blue on Masson trichrome)
- Contain remnant portal tracts and central veins trapped within scars
- Porto-portal and porto-central bridges (hallmark of bridging fibrosis)
-
Bile ductule proliferation - at margins of fibrous septa/nodule interface (ductular reaction)
-
Inflammatory infiltrate in septa:
- Lymphocytes and plasma cells (predominant in viral hepatitis)
- Interface hepatitis (piecemeal necrosis at periphery of nodules)
-
Evidence of etiology (look for):
- Ground glass hepatocytes (HBsAg-containing cells) - in HBV; stain with Orcein or Shikata's stain
- Dense lymphocytic infiltrate with plasma cells - autoimmune hepatitis
- Copper deposits (Rhodanine stain) - Wilson's disease
-
Collapsed reticulin in fibrous septa (Gordon & Sweet's reticulin stain shows condensed black fibers)
Microscopic Diagram to Draw:
POST-NECROTIC CIRRHOSIS - MICROSCOPY (H&E)
┌────────────────────────────────────────────────────┐
│ │
│ ████████ FIBROUS SEPTUM ████████████████ │
│ █ (broad, irregular, collagen, lymphocytes) █ │
│ ████████████████████████████████████████████ │
│ │ │ │
│ ┌────▼──────────────────────────▼────────────┐ │
│ │ REGENERATIVE NODULE (irregular, large) │ │
│ │ □□□□□□□□□□□□□□□□□□□□□□□□□□□□□□□□□□□□□□ │ │
│ │ □ Disordered hepatocytes □□□□□□□□□□□□□□ │ │
│ │ □ Binucleate forms (regeneration) □□□□□ │ │
│ │ □□□□□□□□□□□□□□□□□□□□□□□□□□□□□□□□□□□□□□ │ │
│ │ ↑ No central vein / Portal tract in nodule│ │
│ └────────────────────────────────────────────┘ │
│ │
│ ████ Broad fibrous septa with bile ductules ████ │
│ ████ + lymphocytes + plasma cells ██████████████ │
│ ████████████████████████████████████████████████ │
│ │
│ KEY: □ = hepatocyte █ = fibrous septum/collagen │
└────────────────────────────────────────────────────┘
STAINS:
- H&E: hepatocytes pink, fibrous septa pink
- Masson Trichrome: collagen fibers = BLUE (best for fibrosis)
- Reticulin (Gordon-Sweet): collapsed reticulin = black
- Orcein/Shikata: HBsAg ground glass cells = brown (in HBV)
Comparison: Alcoholic (Micronodular) vs Post-necrotic (Macronodular) Cirrhosis:
| Feature | Alcoholic (Laennec's) | Post-Necrotic |
|---|
| Nodule size | Uniform, <3 mm | Irregular, >3 mm |
| Fibrous septa | Thin, regular | Broad, irregular |
| Etiology | Alcohol | HBV, HCV, drugs, toxins, autoimmune |
| Fat (steatosis) | Often present | Usually absent |
| Mallory bodies | Present (early) | Absent (unless ALD component) |
| Inflammatory cells | Neutrophils | Lymphocytes + plasma cells |
| Reticulin | Preservation of framework | Collapsed framework |
| Liver size | Initially enlarged, then shrunken | Shrunken, irregular |
| HCC risk | Low-moderate | High (especially HBV) |
Complications of Cirrhosis (All Types):
CIRRHOSIS
│
├── PORTAL HYPERTENSION
│ ├── Oesophageal varices → HAEMATEMESIS (most common cause of death)
│ ├── Caput medusae (dilated abdominal veins)
│ ├── Haemorrhoids (anorectal varices)
│ └── Splenomegaly → Hypersplenism (pancytopenia)
│
├── ASCITES (↓ albumin + portal HT + ↑ aldosterone)
│
├── HEPATIC ENCEPHALOPATHY
│ (↑ ammonia, false neurotransmitters, GABA)
│ Asterixis (flapping tremor), confusion, coma
│
├── HEPATORENAL SYNDROME (functional AKI)
│
├── JAUNDICE (hepatocellular type)
│
├── COAGULOPATHY
│ (↓ factor I, II, V, VII, IX, X synthesis)
│
├── ENDOCRINE CHANGES
│ Feminisation: gynecomastia, spider naevi, palmar erythema, loss of body hair
│ Hypogonadism, amenorrhoea
│
└── HEPATOCELLULAR CARCINOMA (HCC)
- Highest risk: HBV (5-10x), HCV, alcoholic cirrhosis
Sources: Yamada's Textbook of Gastroenterology 7e (Wiley); Guyton & Hall Textbook of Medical Physiology 14e; Harper's Illustrated Biochemistry 32e; Lippincott Biochemistry 8e; content aligned with Harsh Mohan Textbook of Pathology 7th ed., Chapter 19 (The Liver, Biliary Tract and Exocrine Pancreas).
QUICK REVISION MNEMONICS FOR MUHS:
Jaundice Types: "PHO" - Pre-hepatic (Hemolytic), Hepatic (Hepatocellular), Obstructive (Post-hepatic)
Obstructive Jaundice Labs: "PALE DUCKS" - Pale stool, ALP ↑↑↑, Absent urobilinogen, Liver enzymes (AST/ALT) normal, Elevated direct bilirubin, Dark urine, Urine bilirubin +, Cholesterol ↑, PT corrects with Vit K, Stool clay-colored
ALD Triad: "FAC" - Fatty change → Alcoholic hepatitis (Mallory's hyaline) → Cirrhosis
Mallory bodies = cytokeratin intermediate filaments = eosinophilic rope-like = PATHOGNOMONIC of alcoholic hepatitis (also Wilson's, PBC, NASH)
Post-necrotic Cirrhosis = MACROnodular = Viral (HBV/HCV) + Drugs + Autoimmune = broad septa + lymphocytes
Stellate cells activated by: TGF-β1 → become myofibroblasts → produce Type I & III collagen → cirrhosis