Sepsis
Reading File
Finding Sources
Searching PubMed
"sepsis" AND "management"
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a comprehensive clinical overview of sepsis, synthesized from Harrison's Principles of Internal Medicine 22e, Rosen's Emergency Medicine, and The Washington Manual of Medical Therapeutics.
Sepsis
Definition (Sepsis-3, 2016)
Sepsis is defined as a life-threatening organ dysfunction caused by a dysregulated host response to infection. It is operationalized as a SOFA (Sequential Organ Failure Assessment) score increase of ≥2 from baseline, which carries an in-hospital mortality >10%.
Septic shock is a subset of sepsis with:
- Persistent hypotension requiring vasopressors to maintain MAP ≥65 mmHg, AND
- Serum lactate >2 mmol/L despite adequate volume resuscitation
- Mortality in septic shock is approximately 40%
The older SIRS (Systemic Inflammatory Response Syndrome) criteria (fever/hypothermia, tachycardia, tachypnea, leukocytosis/leukopenia) have been abandoned as the primary diagnostic framework in Sepsis-3 due to poor specificity - they are still clinically useful but no longer define sepsis.
qSOFA (quick SOFA) - a bedside screening tool: altered mentation, RR ≥22/min, SBP ≤100 mmHg. Score ≥2 should prompt further organ dysfunction assessment.
Epidemiology
- ~88% of sepsis cases are community-onset (detected within 48 h of hospitalization); ~12% are hospital-onset
- ~53% of U.S. sepsis cases are bacterial culture-positive, split roughly evenly between gram-positive and gram-negative organisms
- Most common organisms: S. aureus, Streptococcus spp., E. coli, Klebsiella, Pseudomonas aeruginosa
- Most common primary infection sites: urinary tract (49%), respiratory tract (33%), intra-abdominal (14%), skin/soft tissue (10%)
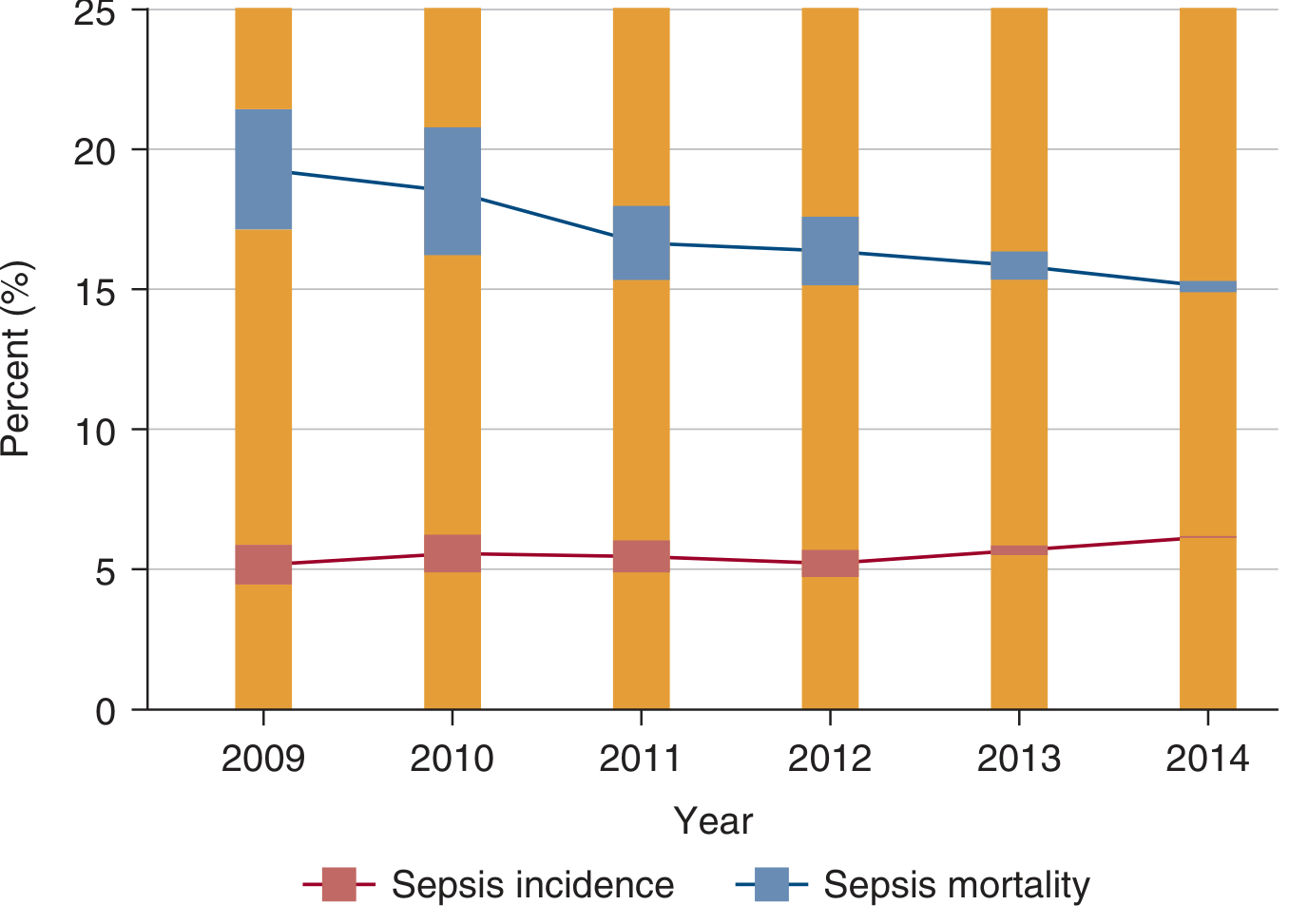
- Mortality has been declining over time despite stable or rising incidence, as shown below:
Pathophysiology
The core mechanism is an exuberant, dysregulated immune response to infection that overflows local containment and causes systemic organ injury.
Trigger: PAMPs and DAMPs
- PAMPs (Pathogen-Associated Molecular Patterns): bacterial LPS (gram-negatives), cell wall components, pathogen nucleic acids
- DAMPs (Damage-Associated Molecular Patterns): histones, HMGB1, oxidized phospholipids, ATP released from injured host cells
- Both are recognized by Pattern Recognition Receptors (PRRs) - including Toll-like receptors (TLRs, 10 human subtypes), NOD receptors, RAGE, and RIG-I receptors
Cellular Responses
- Neutrophils: upregulate CD11b, adhere to endothelium, release Neutrophil Extracellular Traps (NETs) - web-like DNA structures with antimicrobial proteins (cathepsin-G, myeloperoxidase, neutrophil elastase)
- Monocytes/Macrophages: release proinflammatory cytokines - IL-6, IL-18, TNF-α, and activate inducible nitric oxide synthase (iNOS)
- Endothelial cells and platelets: activated, promoting a prothrombotic state with microvascular thrombosis
Net Result
- Systemic vasodilation (NO-mediated)
- Capillary leakage - interstitial fluid accumulation
- Microvascular thrombosis - consuming platelets and clotting factors (risk of DIC)
- Impaired oxygen delivery, uptake, and utilization at the cellular level
- End-organ dysfunction: AKI, ARDS, hepatic dysfunction, encephalopathy, cardiovascular collapse
Hemodynamic Pattern
The "classic" septic patient has a hyperdynamic pattern: low SVR, maintained or increased cardiac output, low filling pressures. However, sepsis-induced myocardial dysfunction also occurs and can present very differently.
Clinical Presentation
| Feature | Detail |
|---|---|
| Fever or hypothermia | T >38°C or <36°C |
| Tachycardia | HR >90 bpm |
| Tachypnea | RR >20/min |
| Altered mental status | Confusion, agitation |
| Hypotension | SBP <90 or MAP <65 in shock |
| Signs of organ failure | Oliguria, jaundice, mottling, coagulopathy |
Laboratory Evaluation
Hematology
- CBC: Leukocytosis or leukopenia; thrombocytopenia in severe sepsis/DIC; bandemia (≥5-10% bands) suggests immature cell release
- Coagulation: Elevated PT/aPTT, decreased fibrinogen, increased fibrin split products - hallmarks of DIC
Chemistry
- Lactate: Key prognostic marker. Lactate 0-2.5 mmol/L = 5% mortality; 2.5-4 = 9%; >4 mmol/L = 28% mortality
- Creatinine/GFR: AKI signals organ failure and worse prognosis
- Bicarbonate: Low bicarb suggests metabolic acidosis from inadequate perfusion
- Anion gap: Elevated AG acidosis in sepsis - usually lactic acidosis
Biomarkers
- Procalcitonin (PCT): PCT >0.5 ng/mL suggests bacterial infection; PCT <0.1 ng/mL makes it less likely. Useful for antibiotic stewardship (serial measurements to guide de-escalation). A low PCT does NOT exclude severe bacterial infection.
- C-reactive protein (CRP): Less specific; useful in serial measurements
Microbiology
- Blood cultures (x2 sets), urine, sputum, CSF, wound cultures - obtain before antibiotics if possible, but do NOT delay antibiotics waiting for cultures
- Only 30-40% of clinical sepsis cases yield positive cultures
Imaging
- CXR: pneumonia, ARDS (bilateral infiltrates)
- CT abdomen/pelvis: intra-abdominal source (abscess, diverticulitis, appendicitis, pancreatitis)
- Echo: endocarditis vegetations, sepsis-induced cardiomyopathy
- MRI: necrotizing fasciitis, epidural abscess
Management
The core principles: early identification, early antibiotics, fluid resuscitation, hemodynamic support, source control.
1. Initial Resuscitation (First Hour - "Hour-1 Bundle")
- IV crystalloid: at least 30 mL/kg IBW within the first hour
- Balanced crystalloids (lactated Ringer's) preferred over normal saline - associated with lower rates of AKI and potentially improved mortality
- Albumin does not show significant benefit over crystalloid
- Monitor volume responsiveness to prevent overload (dynamic parameters: pulse pressure variation, stroke volume variation, passive leg raise response)
2. Vasopressors
Required if MAP <65 mmHg despite adequate resuscitation:
- Norepinephrine - first-line agent (α1 + β1 agonist; dopamine shown to have more adverse events)
- Vasopressin - second-line adjunct; weak evidence of mortality benefit in less severe septic shock (norepinephrine 5-14 μg/min)
- Epinephrine - used in anaphylactic shock; also in cardiogenic shock
- Angiotensin II - adjunct in refractory vasodilatory shock
- Phenylephrine - selective α1 agonist; limited evidence in septic shock
3. Antibiotics
- Initiate broad-spectrum empirical antibiotics immediately after blood cultures - delays in appropriate antibiotics are associated with increased mortality
- Tailor to suspected source and local resistance patterns (e.g., MRSA coverage if high risk, antipseudomonal if immunocompromised)
- De-escalate based on culture results and PCT guidance
Recent evidence (JAMA 2024 meta-analysis, PMID 38864162): prolonged/extended infusion of β-lactam antibiotics is associated with improved outcomes in sepsis/septic shock compared to intermittent bolus dosing.
4. Source Control
- Identify and eliminate the anatomical infection source as soon as possible
- Examples: surgical drainage of abscess, debridement of necrotizing fasciitis, removal of infected central line, cholecystectomy for gangrenous cholecystitis
5. Lactate Clearance
- Target normalization of elevated lactate levels as a resuscitation endpoint
- Lactate clearance is associated with improved mortality
6. Steroids
- Hydrocortisone (200-300 mg/day): consider in septic shock refractory to vasopressors (adrenal insufficiency) - per Surviving Sepsis Guidelines
7. Glycemic Control
- Target blood glucose 140-180 mg/dL; avoid hypoglycemia
8. Mechanical Ventilation (if ARDS develops)
- Low tidal volume ventilation (6 mL/kg IBW)
- Target plateau pressure <30 cmH2O
- Prone positioning for severe ARDS
9. Early Goal-Directed Therapy (EGDT) - Historical Context
- Originally proposed by Rivers et al. (2001): targeted CVP 8-12, MAP ≥65, UO ≥0.5 mL/kg/hr, ScvO2 ≥70%
- Three large multicenter RCTs (ProCESS, ProMISE, ARISE) showed no mortality benefit of formal EGDT over usual care - mainly because usual care had already incorporated early antibiotics and fluid resuscitation
- The principles of early identification and aggressive resuscitation remain valid; the specific EGDT protocol is no longer recommended
Organ-Specific Complications
| Organ | Manifestation |
|---|---|
| Kidney | Sepsis-AKI (most common cause of AKI in ICU) |
| Lung | ARDS - bilateral infiltrates, PaO2/FiO2 <300 |
| Heart | Sepsis-induced cardiomyopathy (reversible) |
| Liver | Shock liver, hyperbilirubinemia |
| Brain | Sepsis-associated encephalopathy |
| Coagulation | DIC |
Surviving Sepsis Campaign (SSC) 2021 Summary
| Timeframe | Action |
|---|---|
| 0-1 hour | Measure lactate; blood cultures; broad-spectrum antibiotics; 30 mL/kg IV crystalloid; vasopressors if MAP <65 |
| 1-3 hours | Reassess fluid responsiveness; re-measure lactate if initial >2 mmol/L |
| 3-6 hours | ICU-level monitoring; source control; corticosteroids if vasopressor-refractory |
Recent Evidence Updates
- PMID 38864162 (JAMA 2024 Meta-Analysis): Prolonged vs. intermittent infusion of β-lactam antibiotics in sepsis/septic shock - prolonged infusion shows improved clinical cure and potentially mortality benefit
- PMID 39961104 (Ann Intern Med 2025, Systematic Review): SEP-1 bundle compliance associated with improved outcomes, though implementation challenges exist
- PMID 39037814 (JAMA Network Open 2024, Meta-Analysis): Sepsis alert systems in EDs are associated with reduced mortality and improved bundle adherence
Sources: Harrison's Principles of Internal Medicine 22e, p. 2360; Rosen's Emergency Medicine 9e, p. 2757; The Washington Manual of Medical Therapeutics, p. 295-297; Scott-Brown's Otorhinolaryngology, p. 404
This is a shared conversation. Sign in to Orris to start your own chat.