Discuss the Pharmacology and drug treatment of heart failure
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
By what time tomorrow
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
Discuss the Pharmacology and drug treatment of heart failure
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Searching PubMed
"heart failure" AND "pharmacological treatment"
I have all the content needed. Here is a comprehensive discussion of the pharmacology and drug treatment of heart failure, drawn from Goodman & Gilman's Pharmacological Basis of Therapeutics (16th Ed.).
Pharmacology and Drug Treatment of Heart Failure
1. Pathophysiology — The Framework for Treatment
Heart failure (HF) is a state in which the heart cannot pump blood at a rate commensurate with the body's needs, or can only do so at elevated filling pressures. Two major syndromes exist:
- HFrEF (Heart Failure with Reduced Ejection Fraction, EF <40%) — systolic failure, the dilated, weak heart
- HFpEF (Heart Failure with Preserved Ejection Fraction, EF >50%) — diastolic failure, the stiff, hypertrophied heart
Key pathophysiological mechanisms driving HFrEF:
| Mechanism | Consequence |
|---|---|
| Reduced cardiac output | Activation of the sympathetic nervous system (SNS) |
| Low renal perfusion | Activation of the renin-angiotensin-aldosterone system (RAAS) |
| Chronic SNS activation | β-receptor downregulation, fibrosis, arrhythmias, cardiomyocyte death |
| Chronic RAAS activation | Na⁺/water retention → volume overload → worsening preload |
| Elevated filling pressures | Pulmonary/peripheral edema (congestion) |
The paradigm shift in HF pharmacology was recognizing that treating symptoms alone (with inotropes) worsens long-term outcomes, while interrupting neurohumoral activation reduces mortality.
2. Heart Failure Staging
| Stage | Description | NYHA Class |
|---|---|---|
| A | Risk factors, no structural disease | — |
| B | Structural disease, no symptoms | I |
| C | Structural disease + current/prior symptoms | II–III |
| D | Refractory HF at rest, refractory to GDMT | IV |
3. Drug Treatment of Chronic HFrEF
Treatment Principle I: Neurohumoral Modulation (RAAS Blockade)
ACE Inhibitors (ACEIs)
- Mechanism: Inhibit conversion of Angiotensin I → Angiotensin II; reduce aldosterone; lower preload and afterload; attenuate cardiac remodeling
- Key trial: CONSENSUS (1987) — enalapril reduced mortality ~40% in NYHA class IV. SOLVD (1991) — ~16% reduction in NYHA II–III
- Examples: Enalapril, lisinopril, captopril, ramipril
- Adverse effects: Dry cough (bradykinin accumulation), angioedema (contraindication to further use), hyperkalemia, hypotension, teratogenicity
- Clinical use: All patients with HFrEF (Stage B–D) unless contraindicated
Angiotensin Receptor Blockers (ARBs)
- Mechanism: Selectively block AT₁ receptors — same downstream benefits as ACEIs without bradykinin-mediated cough
- Examples: Valsartan, candesartan, losartan
- Use: When ACEIs are not tolerated (mainly due to cough); not to be combined with ACEIs due to increased adverse effects without additional benefit
Angiotensin Receptor–Neprilysin Inhibitor (ARNI)
- Drug: Sacubitril/valsartan (LCZ696)
- Mechanism: Sacubitril inhibits neprilysin (which degrades natriuretic peptides BNP, ANP), thereby enhancing vasodilation, natriuresis, and anti-remodeling effects. Combined with valsartan (ARB)
- Key trial: PARADIGM-HF (2014) — sacubitril/valsartan reduced all-cause mortality by ~16% vs. enalapril in 8,442 patients
- Guideline recommendation: Replace ACEI/ARB with ARNI in NYHA II–III patients who can tolerate it. Cannot be combined with an ACEI (risk of angioedema); a 36-hour washout is required when switching from ACEI
Mineralocorticoid Receptor Antagonists (MRAs)
- Drugs: Spironolactone, eplerenone
- Mechanism: Block aldosterone receptors in kidney (reduce Na⁺ retention, K⁺ loss) and heart (reduce fibrosis)
- Key trials:
- RALES (1999): Spironolactone reduced mortality ~30% in severe HF (EF <35%) on background of ACEI + diuretics
- EMPHASIS-HF: Eplerenone reduced mortality in mild HF
- Adverse effects: Hyperkalemia (monitor K⁺ and renal function), gynecomastia/menstrual disorders (spironolactone only — due to sex steroid receptor cross-reactivity; eplerenone is more selective)
- Contraindicated if CrCl <30 mL/min or K⁺ ≥5 mmol/L
Treatment Principle II: Preload Reduction (Diuretics)
Diuretics relieve congestive symptoms (dyspnea, edema) but do not improve mortality in HF.
Loop Diuretics (First-line)
- Drugs: Furosemide, bumetanide, torsemide
- Mechanism: Block Na⁺-K⁺-2Cl⁻ co-transporter in the thick ascending limb of Henle — potent natriuresis
- Furosemide starting dose: 20–40 mg/day; titrate to 40–240 mg/day
- Adverse effects: Hypokalemia, hyponatremia, hypomagnesemia, hyperuricemia, ototoxicity (at high doses), nephrotoxicity
Thiazide Diuretics (Adjunct)
- Drugs: Hydrochlorothiazide, chlorthalidone
- Used in combination with loop diuretics to break diuretic resistance ("sequential nephron blockade")
- Adverse effects: Hypokalemia, hyperuricemia, hypercalcemia, glucose intolerance
Potassium-Sparing Diuretics
- Drugs: Spironolactone, eplerenone (as MRAs), amiloride, triamterene
- Used to prevent hypokalemia; risk of hyperkalemia when combined with ACEIs/ARBs
Treatment Principle III: Afterload Reduction
Hydralazine + Isosorbide Dinitrate (ISDN)
- Mechanism: Hydralazine = arterial vasodilator (reduces afterload); ISDN = venodilator (reduces preload via NO generation)
- Key indication: Black patients with NYHA III–IV HF (A-HeFT trial showed ~43% mortality reduction in African Americans vs. placebo)
- Also used when ACEIs/ARBs/ARNI are contraindicated (e.g., severe renal impairment, bilateral renal artery stenosis)
- Fixed-dose formulation: 37.5 mg hydralazine + 20 mg ISDN (BiDil)
- Adverse effects: Headache (nitrate-related), reflex tachycardia (hydralazine), lupus-like syndrome with prolonged high-dose hydralazine use
Treatment Principle IV: Increasing Cardiac Contractility
Digoxin (Cardiac Glycoside)
- Mechanism:
- Inhibits Na⁺/K⁺-ATPase → raises intracellular Na⁺ → reduces Na⁺/Ca²⁺ exchanger activity → more intracellular Ca²⁺ → positive inotropy
- Vagomimetic effect → slows AV conduction → rate control in atrial fibrillation
- Reduces SNS activation by sensitizing baroreceptors
- Key trial: DIG (1997) — digoxin did not reduce all-cause mortality but reduced HF hospitalizations by ~27%
- Therapeutic range: 0.5–0.8 ng/mL (narrow therapeutic index — target the lower end)
- Adverse effects/toxicity: Nausea, vomiting, visual disturbances (yellow-green halos), cardiac arrhythmias (especially at toxic levels: PVCs, heart block, VT)
- Toxicity precipitants: Hypokalemia, hypomagnesemia, renal insufficiency (digoxin is renally cleared)
- Antidote: Anti-digoxin Fab fragments (Digibind) — purified ovine antibody fragments
Treatment Principle V: Heart Rate Reduction
β-Blockers (Beta-Adrenergic Antagonists)
- Rationale: Chronic SNS activation in HF causes β-receptor downregulation, increased energy consumption, fibrosis, arrhythmias, and cardiomyocyte death. β-Blockers interrupt this maladaptive process
- Mechanism in HF: Competitive antagonism of β₁ (and β₂/α₁ for some agents); long-term benefit: reversal of the "HF gene program," improvement in LVEF after 3–6 months, reduced sudden cardiac death
- Clinical paradox: Acutely depress cardiac function but chronically improve EF and survival
- Key agents approved for HFrEF:
| Drug | Selectivity | Additional actions | t½ | Start → Target dose |
|---|---|---|---|---|
| Bisoprolol | β₁-selective | None | 10–12 h | 1.25 mg → 10 mg OD |
| Metoprolol succinate CR/XL | β₁-selective | None | 3–5 h (extended release required) | 12.5–25 mg → 200 mg OD |
| Carvedilol | Non-selective + α₁-blockade | Vasodilation | 6–10 h | 3.125 mg → 25–50 mg BD |
| Nebivolol | β₁-selective | NO-mediated vasodilation | variable | 1.25 mg → 10 mg OD |
- Key trials: MERIT-HF (metoprolol) and CIBIS-II (bisoprolol) both showed ~34% reduction in all-cause mortality
- Critical prescribing rules:
- Initiate only in clinically stable patients
- Start at one-eighth of target dose
- Titrate every 4 weeks ("start low, go slow")
- Do NOT initiate in acute decompensation or new-onset HF
- Adverse effects: Bradycardia, hypotension, bronchospasm (avoid in reactive airway disease), fluid retention (may require diuretic adjustment), fatigue
- CYP2D6: Metoprolol and carvedilol are CYP2D6 substrates — poor metabolizers (8% of Caucasians) have 5-fold higher Cₘₐₓ
Ivabradine
- Mechanism: Selective inhibitor of cardiac HCN pacemaker channels (Iₓ) → reduces heart rate without affecting contractility or blood pressure
- Indication: NYHA II–III HFrEF, HR >70 bpm in sinus rhythm on maximally tolerated β-blocker dose (guideline Class IIa)
- Adverse effects: Bradycardia, phosphenes (transient visual brightness), increased risk of atrial fibrillation
- Evidence: SHIFT trial (Swedberg et al., 2010) — reduced HF hospitalizations and HF mortality, but not total or cardiovascular mortality
Treatment Principle VI: SGLT2 Inhibition
- Drugs: Dapagliflozin, empagliflozin, canagliflozin
- Primary mechanism: Block sodium-glucose co-transporter 2 (SGLT2) in the proximal tubule → glycosuria + natriuresis ("a better diuretic effect")
- Off-target mechanisms (proposed): Inhibition of Na⁺/H⁺ exchanger (NHE), reduction of myocardial sodium overload, anti-inflammatory effects
- Key trials:
- EMPA-REG OUTCOME (empagliflozin) — initial cardiovascular outcomes trial in diabetic patients; showed major HF benefit
- DAPA-HF (McMurray 2019) — dapagliflozin reduced the composite of worsening HF or cardiovascular death by 26% in HFrEF, independent of diabetes status
- Approval: Dapagliflozin was the first SGLT2 inhibitor approved for HF in the U.S. (2020)
- Adverse effects: Genital mycotic infections, diabetic ketoacidosis (rare), volume depletion
The "Fantastic Four" of modern HFrEF therapy (GDMT): ACEI/ARB/ARNI + β-blocker + MRA + SGLT2 inhibitor — this combination is now guideline-directed medical therapy (GDMT).
4. AHA/ACC Treatment Algorithm for HFrEF (Stage C)
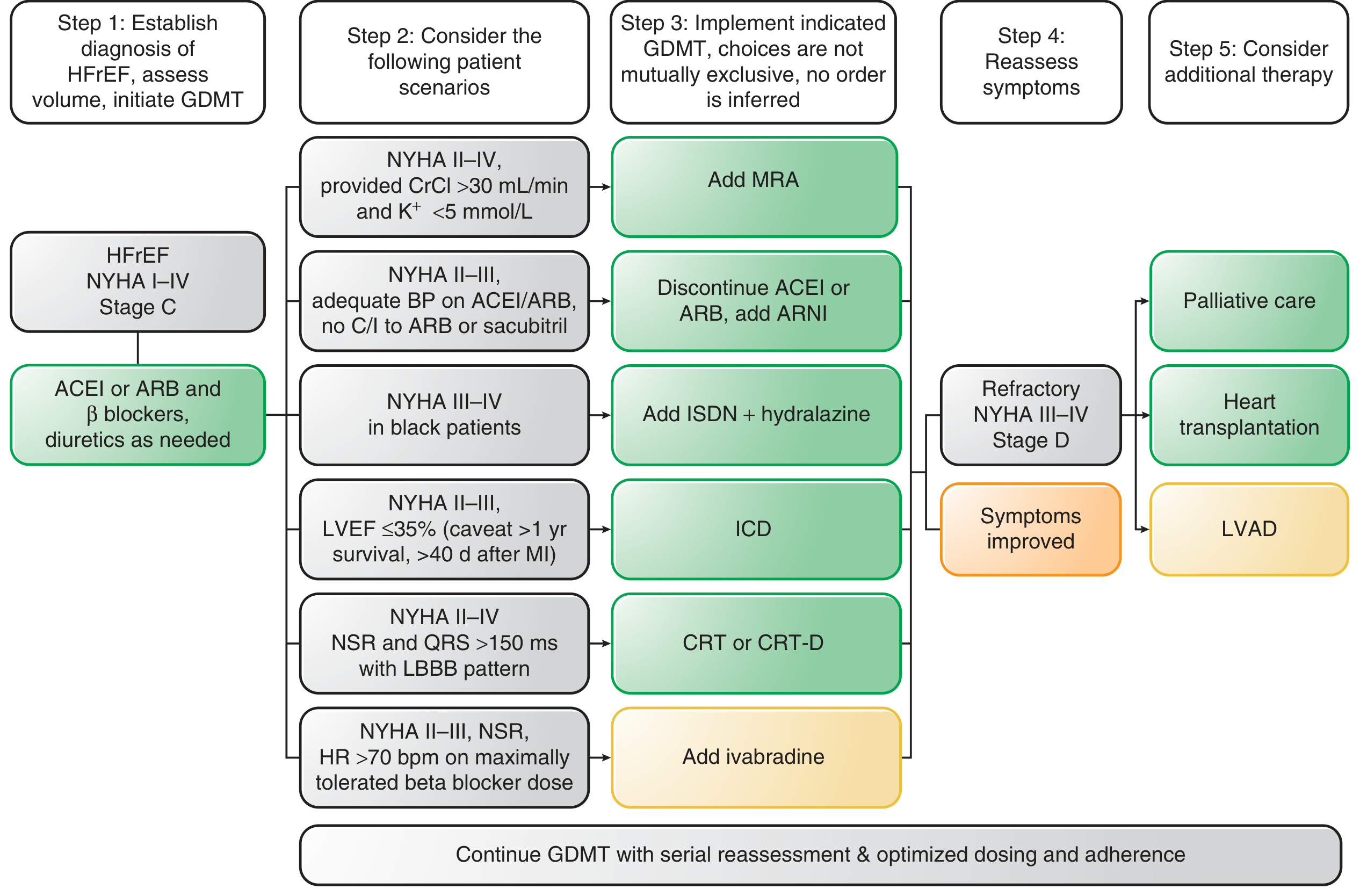
Figure: AHA/ACC Heart Failure Treatment Algorithm — Goodman & Gilman's, 16th Edition
Step-by-step:
- Establish HFrEF diagnosis → Initiate ACEI or ARB + β-blocker; diuretics as needed
- Consider additional therapy (choices not mutually exclusive):
- NYHA II–IV + CrCl >30 + K⁺ <5 → Add MRA
- NYHA II–III, tolerating ACEI/ARB → Switch to ARNI (sacubitril/valsartan)
- NYHA III–IV in Black patients → Add ISDN + hydralazine
- NYHA II–III, LVEF ≤35% → ICD (implantable defibrillator)
- NYHA II–IV, QRS >150 ms with LBBB → CRT (cardiac resynchronization therapy)
- NYHA II–III, HR >70 bpm on max β-blocker → Ivabradine
- Reassess → If refractory (Stage D): heart transplantation or LVAD
5. Drug Treatment of Acutely Decompensated Heart Failure (ADHF)
Acutely decompensated HF is the leading cause of hospitalization in patients >65 years. 1-year mortality is ~30%. The treatment is less evidence-based than chronic HF — no acute drug has improved long-term prognosis.
a) Diuretics (IV loop diuretics — first-line)
- IV furosemide 40–80 mg bolus, then infusion
- Titrate based on symptoms and urine output
- Adding a thiazide (small dose) can overcome loop diuretic resistance
- Avoid excessive doses → hypotension, reduced GFR, electrolyte imbalance, neurohumoral activation
b) Vasodilators
- Nitroglycerin and sodium nitroprusside reduce preload and afterload
- Best for patients with elevated blood pressure; avoid if systolic BP <110 mmHg
- Nesiritide (recombinant BNP): Reduces preload/afterload via cGMP; FDA-approved for ADHF but evidence for improved outcomes is weak
- Main risk: Hypotension (associated with poor outcomes)
c) Positive Inotropic Agents (in cardiogenic shock / severe low-output states)
- Dobutamine (β₁-agonist): Increases myocardial contractility; used short-term in hemodynamically unstable patients
- Dopamine (low dose: DA₁ renal vasodilation; high dose: α₁ vasoconstriction)
- Milrinone (PDE3 inhibitor): Increases cAMP → inotropy + vasodilation ("inodilator"); useful in patients on chronic β-blockers; increased risk of arrhythmias and mortality with prolonged use
d) Myofilament Calcium Sensitizers
- Levosimendan: Binds troponin C → increases Ca²⁺ sensitivity of myofilaments (inotropy without increasing intracellular Ca²⁺ → fewer arrhythmias); also opens K⁺ATP channels (vasodilation); approved in Europe, not the U.S.
- Role: Possibly superior to dobutamine in select patients; no clear mortality benefit
6. Drug Treatment of HFpEF
HFpEF remains the major unmet need in HF pharmacology. No drug has yet shown a mortality benefit in HFpEF. Current recommendations:
- Treat the underlying comorbidities: optimize blood pressure, control diabetes and obesity
- Use diuretics for congestion/symptom relief
- ACEIs, ARBs, spironolactone, sildenafil (PDE5 inhibitor) — all failed in clinical trials
- SGLT2 inhibitors are a promising emerging option (EMPEROR-Preserved trial with empagliflozin showed benefit in HFpEF)
- Exercise training is the only intervention that reliably improves exercise capacity in HFpEF
7. Key Landmark Clinical Trials Summary
| Trial | Drug | Population | Mortality Reduction |
|---|---|---|---|
| CONSENSUS (1987) | Enalapril | NYHA IV | ~40% |
| SOLVD (1991) | Enalapril | NYHA II–III | ~16% |
| DIG (1997) | Digoxin | NYHA II–III | Neutral (↓hospitalization 27%) |
| RALES (1999) | Spironolactone | NYHA III–IV | ~30% |
| MERIT-HF (1999) | Metoprolol CR/XL | NYHA II–IV | ~34% |
| CIBIS-II (1999) | Bisoprolol | NYHA III–IV | ~34% |
| PARADIGM-HF (2014) | Sacubitril/valsartan | NYHA II–IV | ~16% vs. enalapril |
| DAPA-HF (2019) | Dapagliflozin | NYHA II–IV | ~17% vs. placebo |
8. Important Drug Failures — Lessons Learned
The history of HF pharmacology is punctuated by drugs that improved hemodynamics acutely but increased mortality chronically:
| Drug | Mechanism | Failure Reason |
|---|---|---|
| Milrinone, pimobendan | PDE inhibitors (↑cAMP, ↑inotropy) | Increased arrhythmias and death |
| Dobutamine (chronic) | β₁ agonist | Increased mortality |
| Flosequinan, vesnarinone | Mixed mechanisms | Increased mortality |
| Moxonidine | Central sympatholytic | Increased mortality |
| Infliximab, etanercept | TNF-α blockers | Increased mortality (inflammation hypothesis failed) |
| Bosentan | Endothelin receptor antagonist | No benefit in HFrEF |
| Sildenafil | PDE5 inhibitor | Failed in HFpEF |
The central lesson: Drugs that stimulate the failing heart short-term can deplete energy reserves and increase arrhythmic risk. Sustained benefit requires unloading the heart and blocking the maladaptive neurohumoral cascade — not simply increasing contractility.
Summary: The Pillars of HFrEF Pharmacotherapy
NEUROHUMORAL BLOCKADE
├── RAAS: ACEI → ARB → ARNI (sacubitril/valsartan)
├── SNS: β-blockers (bisoprolol, carvedilol, metoprolol XL)
└── Aldosterone: MRA (spironolactone, eplerenone)
VOLUME/HEMODYNAMIC MANAGEMENT
├── Diuretics: Loop (furosemide) ± thiazides
└── Vasodilators: Hydralazine+ISDN (especially Black patients)
NOVEL MECHANISMS
└── SGLT2 inhibitors: Dapagliflozin, empagliflozin
SYMPTOM/RATE CONTROL
├── Digoxin (rate control + symptom relief)
└── Ivabradine (HR reduction when β-blockers insufficient)
Sources: Goodman & Gilman's The Pharmacological Basis of Therapeutics, 16th Edition — Chapter 33: Pharmacological Treatment of Heart Failure; Katzung's Basic and Clinical Pharmacology, 16th Edition.
Recent meta-analysis: Tang et al. (2024) — Network meta-analysis of pharmacological therapy for HFrEF [PMID: 39578732] confirms combination GDMT superiority.
This is a shared conversation. Sign in to Orris to start your own chat.