Give a 10 marks answer for wallerian degeneration from standard orthopaedic textbooks for orthopaedic rguhs pg exams
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive material from multiple standard textbooks. Let me compile the complete 10-marks exam answer.
Wallerian Degeneration
Introduction
Wallerian degeneration (WD) is the ordered, anterograde (distal) degeneration of an axon and its myelin sheath following transection or severe injury that disconnects the axon from its cell body (perikaryon). It was first described by Augustus Volney Waller in 1850 after he observed degeneration in the hypoglossal and glossopharyngeal nerves of frogs following nerve section. It is classically described as "dying forward" - the nerve degenerates from the point of axonal damage outward toward the periphery. This contrasts with "dying-back" (axonal degeneration), seen in metabolic polyneuropathies, where degeneration proceeds from distal to proximal.
- Bradley and Daroff's Neurology in Clinical Practice
- Adams and Victor's Principles of Neurology, 12th Ed
When Does Wallerian Degeneration Occur?
WD follows Sunderland Grade II to Grade V injuries (i.e., axonotmesis and neurotmesis - any injury where axonal continuity is disrupted). It does NOT occur in neuropraxia (Grade I), where only conduction block exists without structural axonal disruption.
| Seddon | Sunderland | Wallerian Degeneration |
|---|---|---|
| Neuropraxia | Grade I | Absent |
| Axonotmesis | Grade II, III, IV | Present |
| Neurotmesis | Grade V | Present |
- Miller's Review of Orthopaedics, 9th Edition
- Rockwood and Green's Fractures in Adults, 10th Edition, 2025
Mechanism / Pathophysiology
Trigger
After nerve injury, the axon distal to the injury site is disconnected from its metabolic hub - the cell body (perikaryon). This disconnection disrupts both anterograde and retrograde axoplasmic transport, triggering a cascade of degenerative events.
Molecular Events (Distal Segment)
- Rapid calcium influx through the disrupted axonal plasma membrane activates calpain proteases, initiating programmed axonal death (sharing features with apoptosis).
- Leukocyte recruitment and cytokine-mediated signaling cascade is initiated.
- Synthesis of neurotrophins, chemokines, extracellular matrix molecules, proteolytic enzymes, and interleukins is upregulated.
- By Day 3: Schwann cells retract from the nodes of Ranvier.
- Activated Schwann cells and macrophages begin to phagocytose axon and myelin debris.
- The entire distal axonal process of WD takes approximately 1 week.
The myelin breaks down into blocks or ovoids containing axon fragments (historically called "digestion chambers of Cajal"). The fragments are converted by macrophages into neutral fats and cholesterol esters, which are then transported away via the bloodstream.
- Bradley and Daroff's Neurology in Clinical Practice
- Adams and Victor's Principles of Neurology, 12th Ed
Changes Distal to the Injury
| Timeframe | Event |
|---|---|
| Minutes - Hours | Disruption of axoplasmic flow, calcium influx |
| Day 1-2 | Axonal swelling, granular disintegration begins |
| Day 3 | Schwann cell retraction from nodes of Ranvier; macrophage infiltration begins |
| Day 3-7 | Active phagocytosis of axon and myelin debris by Schwann cells and macrophages |
| Week 1-3 | Complete Wallerian degeneration of distal segment |
| Week 2-3 | Schwann cell proliferation; formation of Bands of Büngner (Schwann cells lining up within endoneurial tubes) |
The Bands of Büngner are of critical orthopaedic importance - they form a structural scaffold that guides regenerating axons from the proximal stump to distal targets. The upregulation of c-Jun protein in Schwann cells drives the transition from myelin-producing cells to repair/regeneration-supporting cells.
- Rockwood and Green's Fractures in Adults, 10th Ed
- Bradley and Daroff's Neurology in Clinical Practice
Changes Proximal to the Injury
- Limited retrograde degeneration: The axon breaks down back to the first node of Ranvier proximal to the injury site (1-2 nodes).
- Chromatolysis (central chromatolysis): The cell body undergoes:
- Breakup and dispersion of the rough endoplasmic reticulum (Nissl substance)
- Eccentric displacement of the cell nucleus
- Increased nuclear expression of transcription factors
- Switch in gene expression pattern from axon maintenance to protein synthesis (regeneration mode)
- In very proximal injuries (e.g., proximal arm amputation), the cell body itself may undergo apoptosis.
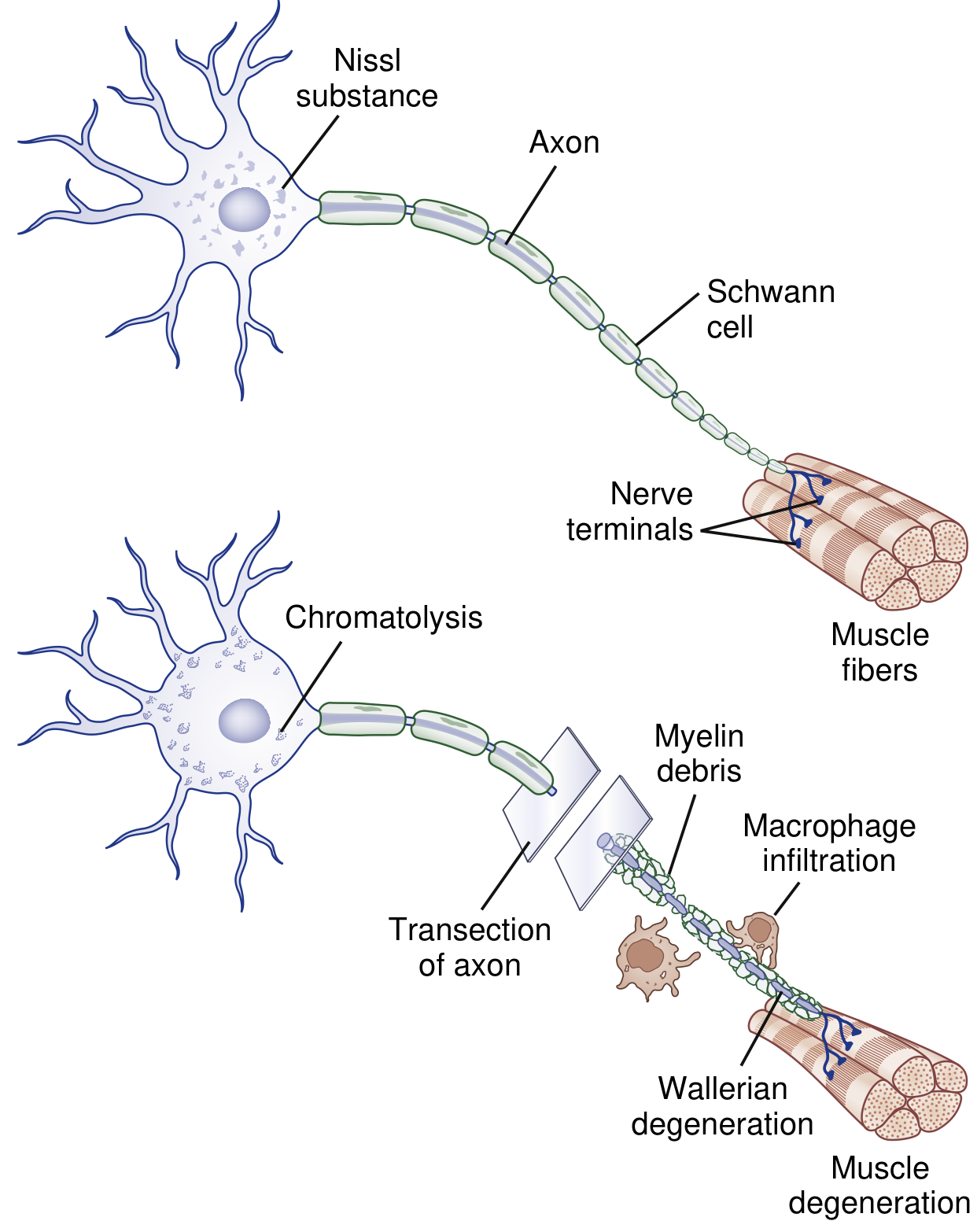
Fig: After axotomy, the axon and myelin distal to the transection degenerate. Macrophages are recruited and digest debris. Proximally, the axon degenerates up to the first node of Ranvier and the cell body undergoes chromatolysis - switching from maintenance to regeneration mode. (Bradley and Daroff's Neurology in Clinical Practice)
Electrodiagnostic Significance
- Before WD is complete (within the first 3-5 days): The distal nerve segment retains electrical excitability. Nerve conduction studies may appear falsely normal distally.
- After WD is complete (beyond Day 7-10): Nerve conduction studies show loss of SNAP and CMAP amplitudes distally.
- EMG: Fibrillation potentials and positive sharp waves appear in denervated muscle, typically 2-3 weeks after injury.
- This is why electrodiagnostic studies are ideally performed 3-4 weeks after injury for accurate severity grading.
- Cummings Otolaryngology (relevant physiologic principle); Miller's Review of Orthopaedics
Nerve Regeneration After Wallerian Degeneration
Once WD and debris clearance are complete, axonal regeneration can begin:
- Axons sprout from the proximal stump, crossing the injury site (a major barrier even if only 1-2 mm across).
- Growth rate: approximately 1 mm/day (or 1 inch/month, clinically used).
- Regenerating axons follow contact guidance from the Bands of Büngner within endoneurial tubes.
- ~50% of fibers fail to cross the repair site, forming a neuroma-in-continuity.
- Problems with regeneration include poor type specificity (motor axons entering sensory tubes) and poor topographical specificity (misdirection to wrong territory) - reasons why fascicular matching during nerve repair is important.
- Hoffman-Tinel sign (advancing Tinel) is the clinical marker of axonal regeneration.
- Regenerated axons remain abnormal - reduced fiber diameter and hence slower conduction velocity compared to normal.
- Rockwood and Green's Fractures in Adults, 10th Ed
Orthopaedic Relevance and Clinical Points
- Timing of surgery: There is strong evidence (experimental and clinical) that delay of repair beyond 1-2 months profoundly deteriorates the quality of nerve regeneration. Early repair (<3 months) is preferred for Sunderland Grade III-V injuries.
- Upper limit of repair: After ~4 years from injury, significant motor recovery is unlikely even with surgical intervention.
- Factors affecting outcome: Age (elderly fare worse), metabolic comorbidities (diabetes, renal failure), mechanism of injury (scalpel laceration better than chain-saw), and distance from injury to target organ.
- Experimental strategies: Pharmacologic agents to slow WD, electrical stimulation to promote axon growth, gene therapy to increase neurotrophic factors, and polyethylene glycol fusion of divided axons (within 24 hours) to prevent WD entirely - these remain experimental.
- Rockwood and Green's Fractures in Adults, 10th Ed
Wallerian Degeneration vs. Other Degenerative Processes
| Feature | Wallerian Degeneration | Axonal Degeneration | Segmental Demyelination |
|---|---|---|---|
| Cause | Axonal transection/severe injury | Metabolic/toxic (dying-back) | Schwann cell / myelin attack |
| Direction | Distal to injury (anterograde) | Distal to proximal (retrograde) | Focal, at internodal segments |
| Axon | Destroyed distal to lesion | Destroyed (distal first) | Intact |
| Myelin | Destroyed distal to lesion | Destroyed parallel to axon | Destroyed; axon spared |
| Muscle atrophy | Yes | Yes | No |
| Example | Nerve transection | Diabetic polyneuropathy | Guillain-Barre Syndrome |
- Adams and Victor's Principles of Neurology, 12th Ed
Summary
Wallerian degeneration is the anterograde degeneration of axon and myelin distal to a nerve injury, occurring in axonotmesis and neurotmesis (Sunderland II-V). It is initiated by calcium-mediated axon destruction, progresses over 1 week, involves Schwann cell and macrophage phagocytosis, and results in formation of Bands of Büngner. Proximally, chromatolysis represents the cell body switching to regeneration mode. Understanding WD is fundamental to interpreting electrodiagnostic studies, planning timing of surgical repair, and predicting functional recovery after peripheral nerve injuries in orthopaedic practice.
References (Standard Textbooks):
- Rockwood and Green's Fractures in Adults, 10th Edition, 2025
- Miller's Review of Orthopaedics, 9th Edition
- Bradley and Daroff's Neurology in Clinical Practice
- Adams and Victor's Principles of Neurology, 12th Edition
Give a 10 marks answer for wallerian degeneration from standard orthopaedic textbooks for orthopaedic rguhs pg exams
I already have comprehensive textbook content from the previous query. Here is the complete 10-marks structured answer:
Wallerian Degeneration
(10 Marks - RGUHS Orthopaedic PG Exam)
1. Definition and Historical Background
Wallerian degeneration (WD) is the ordered, anterograde (distal) degeneration of an axon and its myelin sheath following a nerve injury that disconnects the axon from its cell body (perikaryon). It was first described by Augustus Volney Waller in 1850 after observing degeneration in the hypoglossal and glossopharyngeal nerves of frogs following nerve section.
Adams and Victor's describe it as "dying forward" - degeneration proceeds from the point of axonal damage outward toward the periphery. This contrasts with "dying-back" axonal degeneration seen in metabolic polyneuropathies (e.g., diabetic neuropathy), where degeneration proceeds distal to proximal.
2. When Does Wallerian Degeneration Occur?
WD follows Sunderland Grade II to Grade V injuries - i.e., any injury where axonal continuity is disrupted (axonotmesis and neurotmesis). It does NOT occur in neuropraxia (Grade I), where only focal conduction block exists without structural axonal disruption.
| Seddon Classification | Sunderland Grade | Wallerian Degeneration |
|---|---|---|
| Neuropraxia | Grade I | Absent - only conduction block |
| Axonotmesis | Grade II, III, IV | Present - axon disrupted, connective tissue variably intact |
| Neurotmesis | Grade V | Present - all layers disrupted |
- Miller's Review of Orthopaedics, 9th Ed
- Rockwood and Green's Fractures in Adults, 10th Ed, 2025
3. Pathophysiology - Molecular Trigger
After nerve injury, the axon distal to the injury is disconnected from its metabolic hub (the perikaryon/cell body), disrupting both anterograde and retrograde axoplasmic transport. This triggers the following cascade:
- Rapid calcium and sodium influx through the disrupted axonal plasma membrane
- Calcium activates calpain proteases, initiating programmed axonal death (shares features with apoptosis)
- Leukocyte recruitment and cytokine-mediated signaling cascade is initiated
- Upregulation of neurotrophins, chemokines, extracellular matrix molecules, proteolytic enzymes, and interleukins
- Upregulation of c-Jun protein in Schwann cells - drives transition from myelin-producing cells to repair cells
- Bradley and Daroff's Neurology in Clinical Practice
4. Changes DISTAL to the Injury Site
| Timeframe | Event |
|---|---|
| Minutes - Hours | Disruption of axoplasmic flow; calcium influx; axonal swelling |
| Day 1-2 | Granular disintegration of axon begins |
| Day 3 | Schwann cells retract from nodes of Ranvier; macrophage infiltration begins |
| Day 3-7 | Active phagocytosis of axon and myelin debris by Schwann cells and macrophages |
| ~1 Week | Complete Wallerian degeneration of distal segment |
| Week 2-3 | Schwann cell proliferation; formation of Bands of Büngner |
Bands of Büngner: Schwann cells proliferate and align within endoneurial tubes to form longitudinal cellular columns. These are of critical orthopaedic importance as they form a structural scaffold that guides regenerating axons from the proximal stump to distal targets.
The myelin breaks down into blocks or ovoids containing axon fragments - historically termed "digestion chambers of Cajal". Macrophages convert these into neutral fats and cholesterol esters, which are then transported via the bloodstream.
- Rockwood and Green's Fractures in Adults, 10th Ed
- Adams and Victor's Principles of Neurology, 12th Ed
5. Changes PROXIMAL to the Injury Site
Fig: Wallerian Degeneration. Upper panel - normal neuron. Lower panel - after axotomy: chromatolysis in the cell body, axon degeneration with macrophage infiltration and myelin debris distally, and muscle degeneration at the end organ. (Bradley and Daroff's Neurology in Clinical Practice)
Two key changes occur proximal to the injury:
a) Limited retrograde axonal degeneration - The axon breaks down back proximally only to the first node of Ranvier proximal to the injury site (1-2 internodal segments).
b) Chromatolysis (Central chromatolysis) - The cell body undergoes:
- Breakup and dispersion of Nissl substance (rough endoplasmic reticulum)
- Eccentric displacement of the cell nucleus
- Increased nuclear expression of transcription factors
- Switch in gene expression from axon maintenance mode → protein synthesis/regeneration mode
- This represents the cell body preparing for axonal regeneration
In very proximal injuries (e.g., proximal limb amputation or nerve root avulsion), the cell body itself may undergo apoptosis, precluding regeneration entirely.
- Bradley and Daroff's Neurology in Clinical Practice
6. Electrodiagnostic Significance (Important for Exams)
| Time After Injury | Electrophysiology Finding |
|---|---|
| 0-3 days | Distal nerve segment still electrically excitable - NCS may appear falsely normal |
| Day 7-10 | WD complete - SNAP and CMAP amplitudes fall distally |
| Week 2-3 | Fibrillation potentials and positive sharp waves appear on EMG in denervated muscle |
This is why electrodiagnostic studies are ideally performed 3-4 weeks after injury to accurately grade the severity of nerve injury and distinguish neuropraxia from axonotmesis/neurotmesis.
- Miller's Review of Orthopaedics, 9th Ed
7. Nerve Regeneration After Wallerian Degeneration
Once WD and debris clearance are complete, regeneration begins from the proximal stump:
- Axonal sprouting from proximal stump - begins 2-3 weeks after injury in humans
- Axons must cross the injury/repair site (a significant barrier even if only 1-2 mm)
- Rate of regeneration: ~1 mm/day (clinically: 1 inch/month)
- Regenerating axons follow the Bands of Büngner within endoneurial tubes
- ~50% of fibers fail to cross the repair site, forming a neuroma-in-continuity
- Problems limiting full recovery:
- Poor type specificity (motor axons entering sensory endoneurial tubes)
- Poor topographical specificity (misdirection to wrong target territory)
- Hoffman-Tinel sign (advancing Tinel) = clinical marker of regenerating axons
- Regenerated axons have reduced fiber diameter and slower conduction velocity compared to pre-injury nerves
- Rockwood and Green's Fractures in Adults, 10th Ed
8. Comparison with Other Degenerative Processes
| Feature | Wallerian Degeneration | Axonal Degeneration | Segmental Demyelination |
|---|---|---|---|
| Cause | Nerve transection / severe injury | Metabolic / toxic (dying-back) | Schwann cell / immune attack |
| Direction | Distal to injury (anterograde) | Distal to proximal (retrograde) | Focal, at internodal segments |
| Axon | Destroyed distal to lesion | Destroyed (distal first) | Intact |
| Myelin | Destroyed (parallel to axon) | Destroyed (parallel to axon) | Destroyed; axon spared |
| Muscle atrophy | Yes | Yes | No |
| Fibrillation potentials | Yes | Yes | No |
| Example | Nerve laceration/crush | Diabetic polyneuropathy | Guillain-Barre Syndrome |
- Adams and Victor's Principles of Neurology, 12th Ed
9. Orthopaedic Clinical Relevance
-
Timing of surgical repair: Experimental and clinical evidence strongly supports that delay of repair beyond 1-2 months profoundly deteriorates regeneration quality - due to proximal stump losing ability to grow AND distal stump losing capacity to support axonal growth. Early repair (<3 months) is preferred for Sunderland III-V injuries.
-
Upper limit for repair: After approximately 4 years from injury, significant motor recovery is unlikely regardless of surgical intervention.
-
Factors affecting recovery outcome:
- Age (elderly patients fare worse)
- Metabolic comorbidities (diabetes, renal failure)
- Mechanism of injury (scalpel laceration > chain-saw laceration in prognosis)
- Distance from injury site to target organ (longer = worse)
- Early recovery of motor/sensory function (<3 months) = good prognostic sign
-
Experimental strategies (not yet in clinical use):
- Pharmacologic agents to slow WD
- Electrical stimulation to promote axon growth
- Gene therapy to increase neurotrophic factor production
- Polyethylene glycol (PEG) fusion of divided axon ends within 24 hours to prevent WD entirely - initial experimental results are encouraging
- Rockwood and Green's Fractures in Adults, 10th Ed
10. Summary
Wallerian degeneration is the anterograde degeneration of axon and myelin distal to a nerve injury, occurring in Sunderland Grade II-V injuries. It is initiated by calcium-mediated axonal destruction, is complete within approximately one week, and involves Schwann cell and macrophage-mediated phagocytosis of myelin and axon debris. The Bands of Büngner formed distally act as a regeneration scaffold. Proximally, chromatolysis marks the cell body's shift to regeneration mode. Understanding WD is fundamental to interpreting electrodiagnostic studies (best done at 3-4 weeks), planning the timing of surgical repair, and predicting functional recovery after peripheral nerve injuries in orthopaedic practice.
References (Standard Textbooks):
- Rockwood and Green's Fractures in Adults, 10th Edition, 2025
- Miller's Review of Orthopaedics, 9th Edition
- Bradley and Daroff's Neurology in Clinical Practice
- Adams and Victor's Principles of Neurology, 12th Edition
Give a 10 mark answer for post operative analgesics from standard orthopaedic textbooks for orthopaedic rguhs pg exams
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
I now have rich, comprehensive content from multiple authoritative texts including Miller's Anesthesia, Miller's Review of Orthopaedics, Barash's Clinical Anesthesia, and Rockwood & Green's. Let me compile the complete exam answer.
Postoperative Analgesics
(10 Marks - RGUHS Orthopaedic PG Exam)
1. Introduction
Postoperative pain is one of the most common and significant concerns following orthopaedic surgery. Inadequately treated acute postoperative pain leads to:
- Impaired mobilization and physiotherapy
- Pulmonary complications (splinting, atelectasis)
- Deep vein thrombosis
- Chronic post-surgical pain (central sensitization)
- Prolonged hospital stay and reduced patient satisfaction
The modern standard of care is multimodal analgesia - using multiple drug classes acting at different points in the pain pathway to achieve superior pain control with reduced opioid requirements and side effects.
- Miller's Anesthesia, 10th Edition
- Miller's Review of Orthopaedics, 9th Edition
2. Concept of Multimodal Analgesia
Multimodal analgesia combines different analgesic drug classes that act via different mechanisms on different receptors within the pain transmission pathway to produce:
- Synergistic analgesia
- Reduced opioid consumption and opioid-related side effects
- Earlier mobilization and return of function
- Reduced length of hospital stay
It is the cornerstone of Enhanced Recovery After Surgery (ERAS) pathways and is now recommended by the combined guidelines of the AAHKS, AAOS, and American Society of Regional Anesthesia and Pain Medicine (ASRA).
"The analgesic benefits of controlling postoperative pain are generally maximized when a multimodal strategy to facilitate the patient's convalescence is implemented."
- Miller's Anesthesia, 10th Ed
3. Classification of Postoperative Analgesics
Postoperative Analgesics
├── A. Systemic Agents
│ ├── Opioids (morphine, fentanyl, tramadol)
│ ├── Non-opioids
│ │ ├── Paracetamol (acetaminophen)
│ │ ├── NSAIDs (ketorolac, ibuprofen, diclofenac)
│ │ └── COX-2 inhibitors (celecoxib, parecoxib)
│ └── Adjuvants
│ ├── Gabapentinoids (gabapentin, pregabalin)
│ ├── Ketamine (NMDA antagonist)
│ └── Alpha-2 agonists (clonidine, dexmedetomidine)
└── B. Regional / Locoregional Techniques
├── Neuraxial (epidural, intrathecal)
├── Peripheral nerve blocks
└── Local infiltration / periarticular injection
4. Systemic Analgesics
A. Opioids
Opioids are a cornerstone option for moderate to severe postoperative pain. They act primarily through mu (μ) receptors in the CNS, with some peripheral action at inflamed tissues.
Key features:
- No analgesic ceiling (theoretically), but limited in practice by side effects
- Wide inter-subject variability in dose-response relationship
- Routes: IV (most reliable onset), oral, subcutaneous, transmucosal, intramuscular
- IV/IM used for moderate-to-severe pain; transition to oral once tolerating diet
Common agents:
| Drug | Route | Notes |
|---|---|---|
| Morphine | IV/IM/oral | Gold standard; avoid in renal failure (active metabolite accumulation) |
| Fentanyl | IV | Short-acting; suitable for PCA |
| Tramadol | IV/oral | Weak opioid + serotonin-norepinephrine reuptake inhibitor; lower respiratory depression risk |
| Codeine | Oral | Prodrug - poor metabolizers get no effect; ultra-rapid metabolizers get toxicity |
Side effects of opioids:
- Nausea/vomiting, sedation, respiratory depression, constipation, pruritus, urinary retention
- Risk of dependence and tolerance with prolonged use
Patient-Controlled Analgesia (PCA):
-
Patient self-administers IV opioid bolus via a programmable pump
-
Eliminates administrative delays and compensates for inter-patient variability
-
Settings: demand dose, lockout interval (typically 5-10 min), 1-hour and 4-hour limits
-
Shown to decrease postoperative pain, drug use, sedation, and pulmonary complications compared to PRN regimens
-
Well accepted by patients; improves satisfaction
-
Barash, Cullen, and Stoelting's Clinical Anesthesia, 9th Ed
-
Miller's Anesthesia, 10th Ed
B. Paracetamol (Acetaminophen)
-
Acts centrally via activation of descending serotonergic pathways and inhibition of prostaglandin synthesis
-
Has antipyretic and mild anti-inflammatory properties
-
Maximum dose: 4 g/day in adults (reduce in hepatic disease, elderly, malnourished)
-
Available as: oral, rectal suppository, and IV formulation (FDA approved 2011)
-
IV acetaminophen after joint arthroplasty: decreased pain scores, less opioid use, longer time to morphine rescue, greater patient satisfaction (Sinatra et al.)
-
Meta-analysis of 865 patients (4 RCTs) after total hip arthroplasty showed addition of IV acetaminophen to multimodal analgesia reduced opioid consumption and pain scores
-
AAHKS/AAOS/ASRA strong recommendation: IV or oral acetaminophen does not increase risk of complications following primary total joint arthroplasty (TJA)
-
Miller's Anesthesia, 10th Ed
-
Miller's Review of Orthopaedics, 9th Ed
C. NSAIDs and COX-2 Inhibitors
NSAIDs inhibit cyclooxygenase (COX-1 and COX-2) enzymes, reducing prostaglandin synthesis at the site of inflammation and in the CNS.
AAHKS/AAOS/ASRA strong recommendations (for TJA):
- An oral NSAID given preoperatively and/or early postoperatively reduces pain and opioid consumption after primary TJA
- IV ketorolac given preoperatively, intraoperatively, or within 24 hours postoperatively reduces pain and opioid consumption within the first 48 hours
NNT (Number Needed to Treat) for >50% pain relief in moderate-to-severe pain:
- Ketorolac 30 mg IM: NNT ~3.5 (very effective single-agent analgesic)
- Ibuprofen 400 mg: NNT ~3.0
- (Lower NNT = greater analgesic efficacy)
Side effects and orthopaedic concerns:
| Side Effect | Details |
|---|---|
| GI bleeding | COX-1 inhibition reduces mucosal protective prostaglandins |
| Platelet dysfunction | COX-1 inhibits thromboxane A2 (platelet aggregation); COX-2 inhibitors have minimal effect |
| Renal dysfunction | Risk in hypovolemia, pre-existing renal disease |
| Bone healing | Controversial - two systematic reviews show NO increased nonunion risk with short-term normal-dose NSAIDs; ketorolac >120 mg/day increases spinal fusion nonunion risk (dose-dependent). Short-term NSAID use for post-fracture pain is generally safe |
| Bronchospasm | Avoid in aspirin-sensitive asthma |
COX-2 inhibitors (celecoxib, parecoxib):
-
Fewer GI complications and minimal platelet inhibition
-
Cardiovascular risk with long-term use (rofecoxib withdrawn)
-
Short-term perioperative celecoxib is safe and noninferior to naproxen/ibuprofen for cardiovascular risk (RCT of 24,081 patients)
-
Perioperative NSAIDs not associated with increased risk of postoperative MI after TJA
-
Miller's Anesthesia, 10th Ed
-
Miller's Review of Orthopaedics, 9th Ed
D. Gabapentinoids (Gabapentin and Pregabalin)
These act on the α2-δ subunit of voltage-gated calcium channels in the dorsal horn, reducing central sensitization and neuropathic pain.
AAHKS/AAOS/ASRA strong recommendations for TJA:
-
In the perioperative period: gabapentinoids do NOT reduce postoperative pain, but pregabalin reduces opioid consumption
-
After discharge: pregabalin reduces postoperative pain, neuropathic pain, and opioid consumption after TJA; gabapentin does NOT
-
Pregabalin is 2-4 times more potent than gabapentin as an analgesic
-
Gabapentin: also reduces postoperative delirium in thoracic surgery (900 mg preoperatively)
-
Miller's Review of Orthopaedics, 9th Ed
-
Barash, Cullen, and Stoelting's Clinical Anesthesia, 9th Ed
E. Ketamine (NMDA Receptor Antagonist)
- Blocks N-methyl-D-aspartate (NMDA) receptors, preventing central sensitization and "wind-up"
- Subanesthetic doses (0.05-0.3 mg/kg/h IV infusion) used as adjuvant to opioids
- Benefits: reduces opioid consumption, attenuates opioid-induced hyperalgesia, has anti-inflammatory effects
- Small doses added to morphine PCA reduce morphine consumption and improve respiratory parameters
- Can be administered IV, IM, or epidurally
- Side effects: dysphoria, hallucinations (reduced at low doses), increased secretions
5. Regional / Locoregional Analgesic Techniques
A. Epidural Analgesia (Neuraxial)
- Gold standard for major lower limb, pelvic, and spine surgery
- Catheter placed at a level congruent with the surgical dermatome (catheter incision-congruent analgesia = optimal results)
- Drugs: local anesthetics (bupivacaine, ropivacaine) ± opioids (morphine, fentanyl) ± adjuvants (clonidine, epinephrine)
- Benefits: superior pain control, reduced stress response, earlier mobilization, preserved bowel function
- Complications: hypotension (commonest), urinary retention, motor block, pruritus, respiratory depression (with opioids), rare neurologic injury (<4 in 10,000)
- Lumbar epidural for lower limb surgery causes more frequent quadriceps motor block and may impair early ambulation
B. Peripheral Nerve Blocks (Orthopaedic Specific)
For Total Knee Arthroplasty (TKA) - AAHKS/AAOS/ASRA guidelines:
| Block | Location | Coverage | Notes |
|---|---|---|---|
| Femoral Nerve Block (FNB) | Proximal anterior thigh | Motor + sensory; anterior/medial knee | Quadriceps weakness → fall risk; needs knee immobilizer |
| Adductor Canal Block (ACB) | Medial-anterior midthigh | Sensory only; anterior/medial knee | Preserves quadriceps function; equivalent pain relief to FNB; allows earlier ambulation |
| iPACK Block | Posterior to knee capsule | Sensory only; posterior knee | Blocks terminal sciatic fibers; covers posterior knee pain ("pseudo-DVT pain") |
| Periarticular Block (PAB) | Intraarticular + periarticular | Entire knee | Surgeon-performed; multiple injections of local anesthetic |
Best combination for TKA: ACB + iPACK provides best perioperative pain relief and postoperative function. ACB single injection is as effective as indwelling catheter (catheters dislodge during ambulation).
- Miller's Review of Orthopaedics, 9th Ed
6. WHO Analgesic Ladder (Modified for Postoperative Use)
The WHO analgesic ladder, originally designed for cancer pain, is adapted in reverse for postoperative pain ("ceiling to floor" approach):
| Step | Severity | Agents |
|---|---|---|
| Step 3 (Severe) | NRS 7-10 | IV opioids ± PCA + paracetamol + NSAID + regional block |
| Step 2 (Moderate) | NRS 4-6 | Oral opioids (tramadol/codeine) + paracetamol + NSAID |
| Step 1 (Mild) | NRS 1-3 | Paracetamol + NSAIDs/COX-2 inhibitors |
Descending as pain resolves. Regional techniques should be used at all levels when applicable.
7. Special Considerations in Orthopaedic Surgery
| Situation | Recommendation |
|---|---|
| Total joint arthroplasty | Multimodal: paracetamol + NSAID + ACB + iPACK + pregabalin; minimize opioids |
| Fracture fixation | Short-term NSAIDs safe (no significant nonunion risk); avoid high-dose ketorolac after spinal fusion |
| Opioid-tolerant patients | Higher baseline opioid dose required; avoid undertreatment; risk of withdrawal |
| Elderly patients | Reduce opioid doses; monitor cognition; gabapentinoids cautiously (sedation risk) |
| Obese/OSA patients | Opioid-sparing multimodal strongly recommended to reduce respiratory depression risk |
| Pediatric patients | Paracetamol + NSAIDs + regional blocks; avoid codeine (pharmacogenomic risk) |
8. Monitoring of Postoperative Analgesia
Adequate monitoring is mandatory (per Miller's Anesthesia Box 77.1):
- Pain scores at rest and with activity (VAS or NRS 0-10) - documented regularly
- Vital signs: HR, BP, respiratory rate, SpO2
- Opioid-specific: sedation score, respiratory rate, SpO2
- Regional technique-specific: motor block assessment, site inspection
- PCA-specific: demand dose, lockout interval, successful/unsuccessful attempts, total drug delivered
9. Summary Table
| Drug Class | Example | Mechanism | Main Orthopaedic Use |
|---|---|---|---|
| Opioids | Morphine, Tramadol | μ-receptor agonist | Moderate-severe acute pain; PCA |
| Paracetamol | IV/oral acetaminophen | Central COX inhibition + serotonergic | Base of all multimodal regimens; TJA |
| NSAIDs | Ketorolac, Ibuprofen | COX-1+2 inhibition | Opioid-sparing; TJA; fracture pain |
| COX-2 inhibitors | Celecoxib, Parecoxib | Selective COX-2 inhibition | Reduced GI/platelet risk vs NSAIDs |
| Gabapentinoids | Pregabalin | α2-δ calcium channel | Neuropathic pain; post-TJA (pregabalin) |
| Ketamine | Ketamine infusion | NMDA antagonist | Opioid-sparing adjuvant; central sensitization |
| Epidural | Bupivacaine + fentanyl | Neuraxial blockade | Spine, hip, major lower limb surgery |
| Nerve blocks | ACB, iPACK, FNB | Peripheral nerve blockade | TKA; hip arthroplasty |
10. Conclusion
Optimal postoperative analgesia in orthopaedics requires a multimodal, individualized approach that combines systemic agents (paracetamol, NSAIDs, opioids, adjuvants) with regional techniques (epidural, peripheral nerve blocks, periarticular infiltration). The goals are: adequate pain control, early mobilization, opioid-sparing, and prevention of chronic post-surgical pain. Strong evidence from AAHKS/AAOS/ASRA guidelines supports the use of paracetamol, NSAIDs/ketorolac, pregabalin, and adductor canal block as the pillars of multimodal analgesia in total joint arthroplasty.
References (Standard Textbooks):
- Miller's Anesthesia, 10th Edition
- Miller's Review of Orthopaedics, 9th Edition (AAHKS/AAOS/ASRA guidelines)
- Barash, Cullen & Stoelting's Clinical Anesthesia, 9th Edition
- Rockwood and Green's Fractures in Adults, 10th Edition, 2025
This is a shared conversation. Sign in to Orris to start your own chat.