Isoniazid
Reading File
Finding Sources
Searching PubMed
isoniazid tuberculosis pharmacology toxicity
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a comprehensive overview of Isoniazid (INH) based on authoritative textbook sources:
Isoniazid (INH - Isonicotinic Acid Hydrazide)
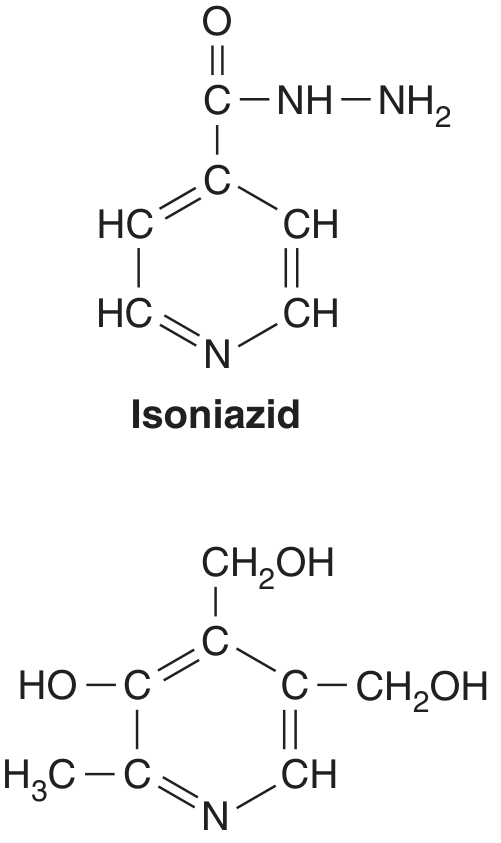
The structural similarity between isoniazid and pyridoxine (vitamin B6) is the basis for INH-induced pyridoxine deficiency and peripheral neuropathy.
Drug Class & Overview
Isoniazid is a first-line bactericidal antitubercular drug (isonicotinic acid hydrazide). It is used in all phases of TB chemotherapy and forms the backbone of short-course regimens (INH + pyrazinamide + rifampin). It is also used as prophylaxis in tuberculin skin test converters without active disease.
- Active against: M. tuberculosis (primary), M. kansasii (first-line), M. bovis (moderate activity)
- Inactive against: MAC (poor activity), all non-mycobacterial genera
- MIC for M. tuberculosis: 0.025-0.05 mg/L (US clinical isolates); 0.1-1 μg/mL by classical assay
Mechanism of Action
INH is a prodrug - it enters bacilli by passive diffusion and must be activated intracellularly:
- KatG (mycobacterial catalase-peroxidase) activates INH, producing an isonicotinoyl radical
- This radical reacts with NAD+ and NADP+ to form ~12 covalent adducts
- Key toxic adducts:
- Nicotinoyl-NAD isomer → inhibits InhA (enoyl-ACP reductase) and KasA (β-ketoacyl-ACP synthase) → blocks mycolic acid synthesis → disrupts cell wall → bactericidal death
- Nicotinoyl-NADP isomer (K < 1 nM) → inhibits dihydrofolate reductase → interferes with nucleic acid synthesis
- KatG activation also produces reactive oxygen species (superoxide, H₂O₂, NO radical) that contribute to mycobactericidal effect. M. tuberculosis is especially susceptible because it has a defect in the oxyR oxidative stress regulator.
- Goodman & Gilman's Pharmacological Basis of Therapeutics, p. 1292
Pharmacokinetics (ADME)
| Parameter | Detail |
|---|---|
| Oral bioavailability | ~100% (300 mg dose) |
| Protein binding | ~10% |
| Distribution | Freely distributes into all body fluids including CSF, caseous tissue, pleural fluid |
| Metabolism | Hepatic NAT2 (N-acetyltransferase 2) → acetylisoniazid → acetylhydrazine → hepatotoxic metabolites (CYP2E1) |
| Excretion | 75-95% in urine within 24 h (as acetylisoniazid + isonicotinic acid) |
| PK model | Two-compartment model |
NAT2 Acetylator Phenotype (Critical Pharmacogenomics)
- Slow acetylators: t½ = 2.1-4.0 h; higher plasma levels (Cmax ~4 μg/mL); greater risk of peripheral neuropathy and hepatotoxicity
- Fast acetylators: t½ < 1.5 h; lower plasma levels (Cmax ~2 μg/mL); risk of reduced microbial cure, relapse, and acquired drug resistance
- 88% of variability in INH clearance is explained by NAT2 genotype
- Fast acetylation more common in: Inuit, Japanese populations
- Slow acetylation predominant in: Scandinavians, North African whites, those of Jewish descent
- Three subgroups now recognized: fast, intermediate, and slow
INH's bactericidal kill is concentration-dependent and correlates with AUC₀₋₂₄ or Cmax.
- Goodman & Gilman's, p. 1292-1293
Mechanisms of Resistance
Prevalence of resistant mutants: ~1 in 10⁶ bacilli (TB cavities may contain 10⁷-10⁹ organisms, so pre-existing resistance is expected).
| Mutation | Effect | Level of Resistance |
|---|---|---|
| KatG mutation/deletion (especially Ser315Asn) | Cannot form nicotinoyl-NAD adducts; retains catalase activity and biofitness | High-level |
| InhA overexpression | Reduced drug binding at target | Low-level (+ cross-resistance to ethionamide) |
| ahpC overexpression | Detoxifies organic peroxides, compensates for KatG loss | Low-level |
| kasA mutations | Resistance at β-ketoacyl synthase | Variable |
| Efflux pump induction | Reduces intracellular drug concentration | Low-level |
Because resistance mutations are independent events, the probability of resistance to two drugs is ~1 in 10¹² → justifies combination therapy.
Adverse Effects
1. Hepatotoxicity (Most Serious)
-
Transaminase elevation occurs in 10-36% of patients in the first 10 weeks (usually minor and self-limiting)
-
Clinical hepatitis develops in ~2% of all exposed patients; 5-10% of hepatitis cases are fatal
-
Severe hepatic injury in ~0.1% of all patients
-
Risk increases with age: 0.3% in 3rd decade → ≥2% after age 50
-
70% of fatal cases occur in women; Black and Hispanic women are at particular risk
-
Risk is NOT dose-related
-
Mechanism: acetylhydrazine metabolite → CYP2E1 → reactive hepatotoxic metabolites; immune-mediated component also implicated
-
Potentiated by: alcohol, rifampin, pyrazinamide, acetaminophen, chronic HBV/HCV/HIV infection, malnutrition
-
Histology: hepatocellular necrosis (focal or zonal/submassive/massive)
-
INH hepatotoxicity is the second leading cause of drug-induced liver injury requiring liver transplantation in the USA (after acetaminophen)
-
Sleisenger & Fordtran's GI & Liver Disease, p. 1677
2. Peripheral Neuropathy
- Occurs in ~2% of patients taking 5 mg/kg/day without pyridoxine supplementation
- Mechanism: INH is a structural analog of pyridoxine (vitamin B6) → causes excessive renal excretion of pyridoxine → depletes neuronal pyridoxal 5'-phosphate → impairs GABA synthesis
- Symptoms: paresthesias of hands and feet (most common), ataxia, muscle twitching
- More frequent in: slow acetylators, diabetics, malnourished patients, alcoholics, patients with anemia
- Prevention: co-administer pyridoxine 25-50 mg/day
3. CNS Toxicity
- Seizures (especially in those with pre-existing seizure disorders)
- Optic neuritis and atrophy
- Dizziness, ataxia, toxic encephalopathy
- Mental abnormalities: euphoria, memory impairment, psychosis
4. Drug-Induced Lupus / Autoimmune
- Vasculitis with anti-nuclear antibodies
- Drug-induced SLE syndrome
- Arthritic symptoms
- All resolve on discontinuation
5. Miscellaneous
- Dry mouth, epigastric distress, methemoglobinemia, tinnitus, urinary retention
- Sideroblastic/pyridoxine-deficiency anemia (in predisposed patients)
INH Overdose (Toxicology)
Classic triad (ingestion >20-30 mg/kg):
- Seizures - generalized tonic-clonic, refractory to phenytoin/barbiturates/benzodiazepines alone
- Anion-gap metabolic acidosis - refractory to NaHCO₃ (lactic acidosis from seizure activity)
- Coma
Symptoms appear within 30 minutes to 3 hours of ingestion.
Treatment:
- IV Pyridoxine - gram-for-gram equivalent to the amount of INH ingested
- Unknown dose: 5 g IV in adults (70 mg/kg in children, max 5 g); give 1 g every 2-3 min until seizures stop
- Benzodiazepines for seizures (in combination with pyridoxine)
- Phenytoin has NO role
- NaHCO₃ has little role
- Patients asymptomatic for 6 hours after ED presentation are safe for discharge
Mechanism of seizures: INH binds pyridoxal 5'-phosphate → depletes GABA (primary CNS inhibitory neurotransmitter)
- Tintinalli's Emergency Medicine, p. 1276-1299
Drug Interactions (via CYP Inhibition/Induction)
| Drug | Mechanism | Effect |
|---|---|---|
| Acetaminophen | CYP2E1 induction | Increased hepatotoxicity |
| Phenytoin / fosphenytoin | CYP2C19 inhibition | Phenytoin toxicity (neurological) |
| Carbamazepine | CYP3A inhibition | Neurological toxicity |
| Diazepam | CYP3A + CYP2C19 inhibition | Sedation, respiratory depression |
| Warfarin | CYP2C9 inhibition | Increased bleeding risk (esp. INH >300 mg/day) |
| Theophylline | CYP3A inhibition | Seizures, palpitations, nausea |
| Ethosuximide | CYP3A inhibition | Psychotic behavior |
| Vincristine | CYP3A inhibition | Limb weakness, tingling |
- Goodman & Gilman's, Table 65-4
Clinical Use Summary
| Use | Regimen |
|---|---|
| Active pulmonary TB (drug-susceptible) | HRZE × 2 months → HR × 4 months (DOTS) |
| TB meningitis | Extended 9-12 month regimen |
| Latent TB infection (LTBI) prophylaxis | INH 300 mg/day × 6-9 months (or 3HP: INH + rifapentine weekly × 12 weeks) |
| M. kansasii | First-line agent |
Recent evidence (PubMed, 2024): A systematic review/meta-analysis (PMID 39639188, BMC Genomic Data, Dec 2024) confirmed that NAT2 genetic variants are significantly linked to isoniazid-induced hepatotoxicity risk, reinforcing current pharmacogenomic guidance on NAT2 testing to predict adverse outcomes. This is consistent with the textbook mechanistic framework above.
Key memory mnemonics:
- INH = "Inhibits Nicotinoyl-adduct formation in Hep C-like fashion" - prodrug, needs KatG
- Side effects: Hepatitis, Inhibits pyridoxine (neuropathy), Natural resistance via KatG mutation
- Prevent neuropathy with B6 (pyridoxine); treat overdose with IV pyridoxine
This is a shared conversation. Sign in to Orris to start your own chat.