Bell mgendie law physiology
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Loading Image
Finding Sources
I now have excellent textbook content and the diagram. Let me compile a thorough answer.
Bell-Magendie Law
The Law
The Bell-Magendie Law states that:
Dorsal (posterior) roots of spinal nerves are sensory (afferent); ventral (anterior) roots are motor (efferent).
This is one of the foundational principles of neuroanatomy and spinal cord physiology.
The Diagram
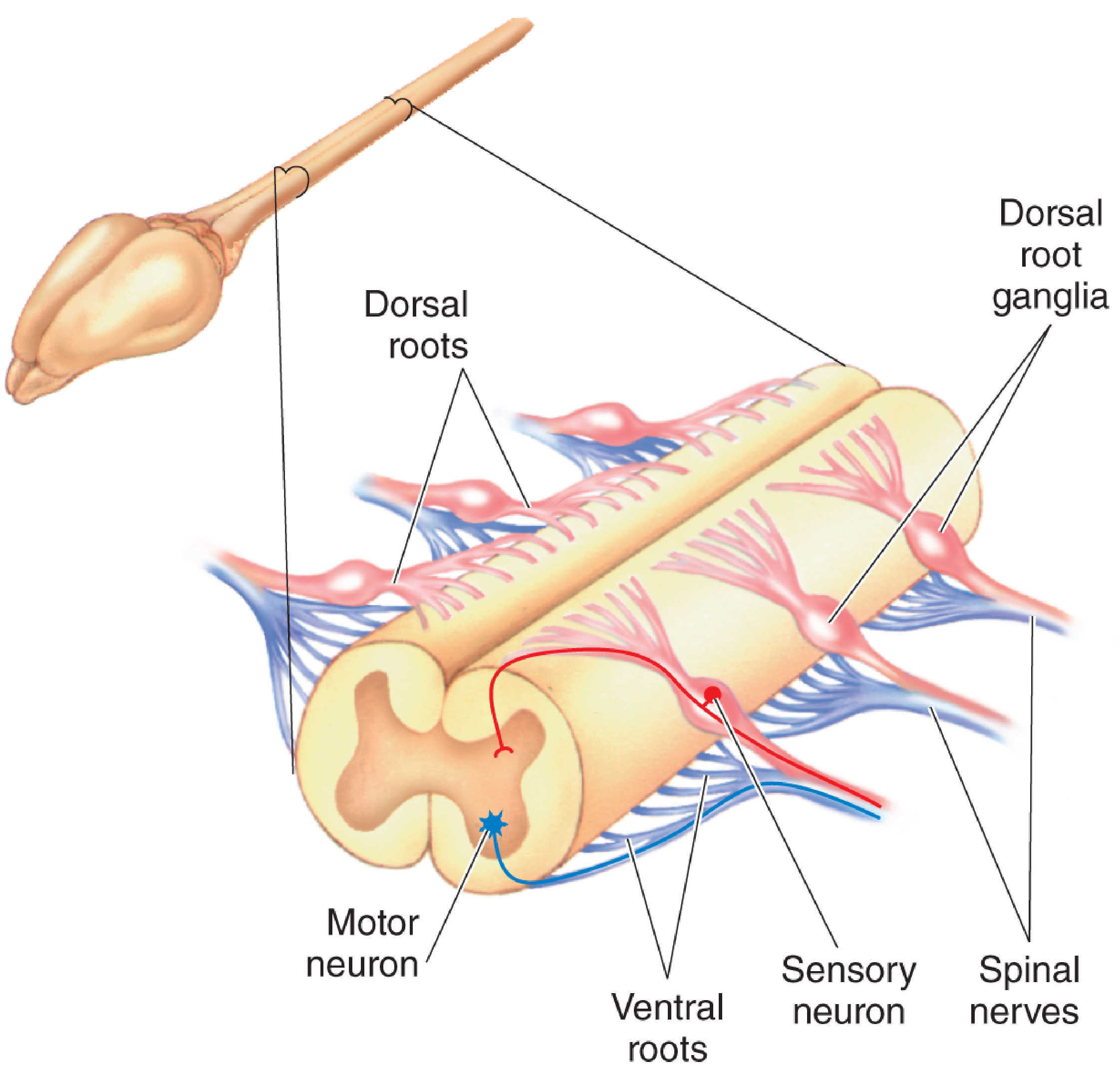
The spinal cord with dorsal roots (sensory, pink) and ventral roots (motor, blue) combining to form spinal nerves. - Neuroscience: Exploring the Brain, 5th Ed.
Historical Background
The law is named after Charles Bell (Scottish anatomist) and François Magendie (French physiologist), who independently demonstrated the functional distinction of spinal nerve roots in the early 19th century.
- Charles Bell (1811) first proposed that the ventral root carries motor axons - axons that command muscles to move.
- François Magendie (1822) experimentally demonstrated that the dorsal root is sensory by cutting each root separately in animal experiments and observing the distinct loss of sensation vs. movement. His experiments used unanesthetized animals (he was later criticized for this by Bell and others).
- Together, their work established the principle as "Bell-Magendie Law."
As stated in Neuroscience: Exploring the Brain, 5th Ed.:
"François Magendie showed that the dorsal root contains axons bringing information into the spinal cord, such as those that signal the accidental entry of a tack into your foot. Charles Bell showed that the ventral root contains axons carrying information away from the spinal cord - for example, to the muscles that jerk your foot away in response to the pain of the tack."
Anatomy and Physiology
Dorsal Root (Sensory / Afferent)
- Contains afferent (sensory) nerve fibers carrying impulses from the periphery INTO the spinal cord
- Sensory modalities carried: pain, temperature, touch, pressure, proprioception, vibration
- The cell bodies of these sensory neurons are located in the dorsal root ganglion (DRG) - a swelling just outside the spinal cord
- One dorsal root ganglion is present for each spinal nerve level
- The central processes enter the dorsal horn of the spinal cord; peripheral processes go to skin, muscle, and joints
Ventral Root (Motor / Efferent)
- Contains efferent (motor) nerve fibers carrying impulses FROM the spinal cord OUT to muscles and glands
- The cell bodies of these motor neurons (lower motor neurons) lie within the ventral horn of the spinal cord gray matter (entirely within the CNS)
- Their axons exit via the ventral root into the periphery
- Also carries preganglionic autonomic fibers (sympathetic in T1-L2; parasympathetic in S2-S4)
Spinal Nerve Formation
After exiting, the dorsal and ventral roots unite to form a mixed spinal nerve, which contains both sensory and motor fibers. The spinal nerve then divides into:
- Dorsal (posterior) primary ramus - supplies back muscles and skin
- Ventral (anterior) primary ramus - supplies limbs and anterior/lateral trunk
Clinical Significance
| Lesion | Effect |
|---|---|
| Dorsal root or DRG damage | Pure sensory loss (anesthesia, loss of proprioception) - no motor deficit |
| Ventral root damage | Pure motor deficit (lower motor neuron weakness, flaccid paralysis, muscle atrophy) - no sensory loss |
| Spinal nerve damage (distal to union) | Mixed sensory and motor deficit |
| Anterior horn cell disease (e.g., polio, ALS) | Pure motor weakness without sensory loss |
Examples in disease:
- Tabes dorsalis (neurosyphilis): selective dorsal root/posterior column degeneration → sensory ataxia, loss of proprioception, no motor loss - consistent with Bell-Magendie law
- Poliomyelitis: destroys anterior horn cells → flaccid paralysis without sensory loss
- Herniated disc: can compress a dorsal root → radicular pain and/or sensory loss in a dermatomal pattern; if ventral root is compressed → weakness in the corresponding myotome
Summary Table
| Feature | Dorsal Root | Ventral Root |
|---|---|---|
| Function | Sensory (afferent) | Motor (efferent) |
| Cell body location | Dorsal root ganglion (PNS) | Ventral horn (CNS) |
| Direction of impulse | Periphery → CNS | CNS → Periphery |
| Cutting effect | Loss of sensation | Paralysis |
| Autonomic fibers | None | Preganglionic autonomic |
The Bell-Magendie Law remains the anatomical basis for understanding radiculopathies, spinal cord injury levels, and the distinction between sensory vs. motor neuropathies. - Neuroscience: Exploring the Brain, 5th Ed., p. 577
Role of skin in temperature regulation physiology. First year MBBS.
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Finding Sources
I now have excellent, comprehensive content from Guyton & Hall. Let me compile the full answer for a 1st year MBBS student.
Role of Skin in Temperature Regulation
Based on Guyton and Hall Textbook of Medical Physiology
Overview
The human body maintains a core temperature of 37°C (98.6°F) through a process called thermoregulation. The skin is the primary effector organ for heat exchange with the environment, while the hypothalamus acts as the central thermostat. The skin contributes to temperature regulation through:
- Cutaneous blood flow (vasodilation / vasoconstriction)
- Sweating (evaporative heat loss)
- Piloerection (insulation)
- Subcutaneous fat (insulation)
- Temperature sensing (thermoreceptors)
1. The Hypothalamus - The Body's Thermostat
Before diving into the skin's role, it is important to understand the control center:
- The anterior hypothalamic-preoptic area contains heat-sensitive and cold-sensitive neurons
- When heated, it immediately triggers: skin vasodilation + profuse sweating all over the body
- The posterior hypothalamus integrates signals from both the preoptic area AND peripheral skin receptors to coordinate the final response
- When the preoptic area is cooled: shivering is triggered and sweating is inhibited
2. Skin as a Sensory Organ for Temperature
The skin contains both cold receptors and warmth receptors, but importantly:
"The skin has far more cold receptors than warmth receptors - in fact, 10 times as many in many parts of the skin. Therefore, peripheral detection of temperature mainly concerns detecting cool and cold instead of warm temperatures."
- Guyton & Hall, Medical Physiology
- Temperature sensing is mediated by TRP (Transient Receptor Potential) channels in somatosensory neurons and epidermal cells:
| TRP Protein | Function | Activation Threshold |
|---|---|---|
| TRPV1 | Heat sensor | ≥42°C (pain/burning) |
| TRPV3 | Warmth sensor | ≥32°C |
| TRPV4 | Warmth sensor | ≥27°C |
| TRPM8 | Cold sensor | ≤27°C |
| TRPA1 | Cold sensor | ≤17°C (icy cold) |
When the skin is chilled over the entire body, it reflexly:
- Stimulates shivering (increases heat production)
- Inhibits sweating
- Promotes skin vasoconstriction (reduces heat loss)
3. Cutaneous Blood Flow - The Most Powerful Mechanism
The skin has an enormous capacity to vary its blood flow - this is the primary mechanism of heat transfer between the core and the environment.
In Hot Conditions - Vasodilation
- Sympathetic vasoconstrictor tone is inhibited by the posterior hypothalamus
- Skin blood vessels dilate intensely
- This brings warm core blood to the skin surface where heat radiates, conducts, and convects into the environment
- Full vasodilation can increase the rate of heat transfer to the skin as much as 8-fold
In Cold Conditions - Vasoconstriction
- The posterior hypothalamus stimulates sympathetic centers
- Skin blood vessels constrict, shunting blood away from the periphery to the core
- Reduces heat loss from the body surface dramatically
- This is why skin turns pale and cold in cold weather
Countercurrent Heat Exchange
- Deep arteries and veins run alongside each other in the limbs
- Warm arterial blood going outward transfers heat to the cool venous blood returning - conserving body heat in cold conditions
4. Sweating - Evaporative Heat Loss
This is the most effective cooling mechanism when environmental temperature exceeds skin temperature.
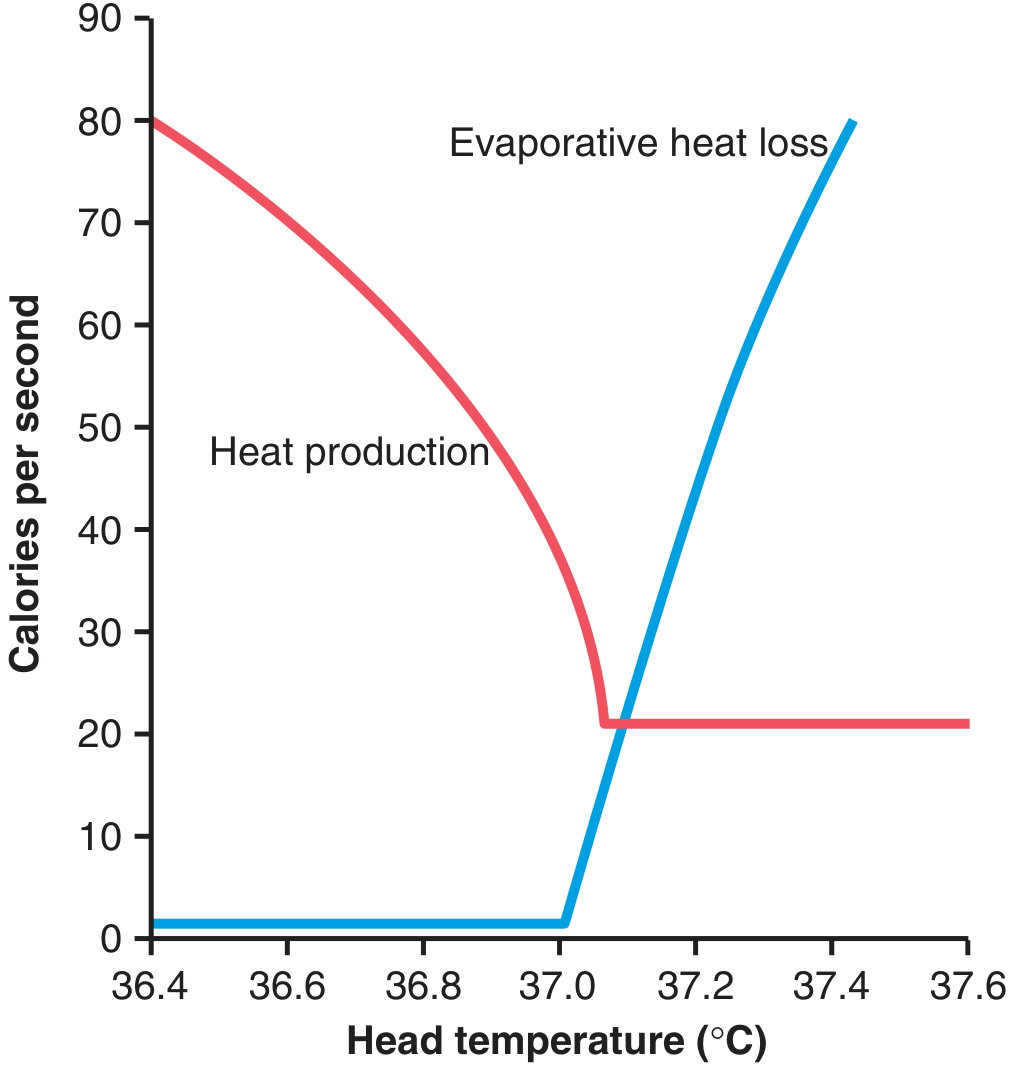
Figure: At the critical core temperature of ~37.1°C, evaporative heat loss from sweating rises sharply while heat production falls to minimum. - Guyton & Hall
Eccrine Sweat Glands
- 2-5 million eccrine glands distributed over the entire body surface
- Controlled by cholinergic sympathetic nerve fibers (unique - sympathetic but uses acetylcholine)
- Sweat is essentially dilute plasma (99% water + NaCl, urea, lactic acid)
- As sweat evaporates from skin surface, it absorbs 580 kcal of latent heat per liter of water evaporated - very efficient cooling
- An additional 1°C rise in body core temperature above 37.1°C causes sweating sufficient to remove 10 times the basal rate of body heat production
Apocrine Sweat Glands
- Found in axilla, groin, areola
- Respond to emotional stimuli (stress, fear, pain) via adrenergic (norepinephrine) stimulation
- Not important in thermoregulation
Methods of Heat Loss via Skin
| Method | Mechanism | Condition |
|---|---|---|
| Radiation | Infrared heat emission from skin surface | At rest; accounts for ~60% of heat loss |
| Conduction | Direct contact heat transfer to cooler objects | Minor unless immersed in water |
| Convection | Air carries away heat from skin surface | Wind/moving air increases loss |
| Evaporation | Sweating - only effective method when ambient temp > skin temp | Hot environments; exercise |
5. Piloerection ("Goosebumps")
- Cold triggers sympathetic stimulation of arrector pili muscles attached to hair follicles
- Hairs stand upright ("goosebumps")
- In humans this has minimal effect, but in animals it traps an insulating layer of air next to the skin, greatly reducing heat loss
6. Subcutaneous Fat - Insulation
- The subcutaneous fat layer acts as a thermal insulator
- Fat conducts heat ~1/3 as readily as other body tissues
- Prevents heat loss from the core to the skin and then to the environment
- This is why obese individuals and marine mammals (whales, seals) retain heat better in cold environments
7. Local Skin Temperature Reflexes
The skin also participates in local reflex arcs independently of the hypothalamus:
"When a person places a foot under a hot lamp, local vasodilation and mild local sweating occur. Placing the foot in cold water causes local vasoconstriction and cessation of sweating. These are caused by local effects directly on blood vessels AND by local cord reflexes from skin receptors to the spinal cord and back."
- Guyton & Hall
This means each skin area can regulate itself locally, with the hypothalamus modulating the overall intensity.
8. Skin Temperature Can Alter the Hypothalamic Set Point
An important concept: skin temperature signals can shift the threshold at which the hypothalamus triggers sweating or shivering:
- Warm skin lowers the set point for sweating (sweating begins at a lower core temp)
- Cold skin raises the set point for shivering (shivering begins at a higher core temp)
- This is an "anticipatory" mechanism - cold skin predicts a fall in core temperature and pre-emptively increases heat production
Summary Diagram (Concept)
COLD ENVIRONMENT HOT ENVIRONMENT
↓ ↓
Skin cold receptors Skin warm receptors
↓ ↓
Posterior Hypothalamus ←→ Anterior Hypothalamic-Preoptic Area
↓ ↓
• Skin vasoconstriction • Skin vasodilation (8x heat transfer)
• Piloerection • Sweating (eccrine, cholinergic)
• Shivering • Inhibit heat production
• Fat insulation retained • Behavioral responses
↓ ↓
HEAT CONSERVED HEAT DISSIPATED
Clinical Relevance (for exams)
| Condition | Thermoregulation Defect |
|---|---|
| Spinal cord transection above T1 | Hypothalamus cannot control sweating or skin blood flow - poikilothermia |
| Anhidrosis (no sweating) | Heat stroke risk in hot environments |
| Burns | Loss of skin barrier - uncontrolled evaporative water and heat loss |
| Neonates | Poorly developed thermoregulation - easily hypothermic |
| Fever | Hypothalamic set point raised by pyrogens (IL-1, PGE2) - vasoconstriction + shivering to REACH the new set point |
Primary source: Guyton and Hall Textbook of Medical Physiology (Chapter 74 - Regulation of Body Temperature)
This is a shared conversation. Sign in to Orris to start your own chat.