Stages of pubertal development and premenstrual syndrome- answer for dnb paper- defence from novacks gynae and recent recommneded updates
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Searching PubMed
premenstrual syndrome PMDD treatment guidelines
Reading File
Reading File
Reading Article
PMID: 37973069
Reading File
Reading File
Searching the Web
ACOG 2023 premenstrual disorders clinical practice guideline No 7 recommendations summary
Reading Web Page
https://docred-strapi-cms-prod.s3.sa-east-1.amazonaws.com/ma…
Reading File
I now have comprehensive data from Berek & Novak's Gynecology and the ACOG 2023 guideline. Let me compile the complete DNB-level answer.
Stages of Pubertal Development & Premenstrual Syndrome
DNB Paper Answer - Berek & Novak's Gynecology + ACOG 2023 Updates
PART 1: STAGES OF PUBERTAL DEVELOPMENT
Overview
Pubertal development in girls occurs in an orderly, predictable sequence over approximately 4.5 years. Any deviation from this sequence or the expected time frame should be regarded as abnormal. The first sign of puberty is accelerated growth, followed by breast budding, appearance of pubic hair, peak growth velocity, and finally menarche.
Pubertal changes begin on average in the 11th year of life, with a wide range of normal.
(Berek & Novak's Gynecology, p. 311)
Marshall-Tanner Staging
Breast Development (Thelarche)
| Stage | Description |
|---|---|
| Stage 1 (Prepubertal) | No palpable breast tissue; areolae generally <2 cm; nipple may be inverted, flat, or raised |
| Stage 2 (Breast bud) | Visible and palpable mound of breast tissue; areolae begin to enlarge; skin of areolae thins; nipple develops |
| Stage 3 | Further growth and elevation of entire breast; when seated, nipple is at or above the midplane of breast tissue |
| Stage 4 | Areola and papilla project above the general breast contour as a secondary mound |
| Stage 5 (Mature) | Mature contour and proportion; nipple more pigmented; Montgomery glands visible; nipple is below midplane when seated |
Full breast development usually takes 3 to 3.5 years, but may occur in as little as 2 years. Breast size is no indication of breast maturity.
(Berek & Novak's Gynecology, p. 312)
Pubic Hair Development (Pubarche)
| Stage | Description |
|---|---|
| Stage 1 | No sexually stimulated pubic hair; some nonsexual fine hair may be present in genital area |
| Stage 2 | First appearance of coarse, long, crinkly pubic hair along the labia majora |
| Stage 3 | Coarse, curly hair extends onto the mons pubis |
| Stage 4 | Adult hair in thickness and texture; not as widely distributed as adults; does not extend onto inner thighs |
| Stage 5 | Adult distribution; hair extends onto inner aspects of thighs; may extend toward umbilicus and anus |
(Berek & Novak's Gynecology, p. 313)
Note: In boys, pigmented pubic hair is often the first recognized sign of puberty, though it typically appears about 6 months after genital growth begins. Tanner stage 3 in boys is often accompanied by gynecomastia (symmetric or asymmetric), and mature sperm can first be identified by microscopy.
Sequence of Pubertal Events in Girls
- Accelerated linear growth (first sign)
- Thelarche (breast budding) - typically first recognized change
- Adrenarche/Pubarche (pubic/axillary hair)
- Peak height velocity
- Menarche (average age ~12.5-13 years in the US; occurs approximately 2-3 years after thelarche)
Growth and Body Composition Changes
- Girls reach peak height velocity early in puberty, before menarche - so they have limited growth potential after menarche.
- Boys reach peak height velocity about 2 years later than girls.
- Boys grow an average of 28 cm during the growth spurt; girls grow a mean of 25 cm.
- Adult men are on average 13 cm taller than women.
- By maturity, men have 1.5x the lean body mass and 1.5x the skeletal mass of women; women have twice as much body fat.
- Estrogen drives characteristic fat distribution at thighs, buttocks, and abdomen in girls.
- Testosterone is the primary anabolic driver of male pubertal changes.
(Berek & Novak's Gynecology, p. 315)
Mechanisms Underlying Puberty
The hypothalamic-pituitary-gonadal (HPG) axis develops in two distinct stages during puberty:
- Early puberty: Decreased sensitivity to the negative/inhibitory effects of low circulating sex steroids present in childhood
- Late puberty: Maturation of the positive/stimulatory feedback response to estrogen, responsible for the ovulatory mid-cycle LH surge
GnRH Pulse Generator:
- The central nervous system inhibits puberty onset until the appropriate time
- At puberty, the GnRH pulse generator is reactivated (disinhibited) - leading to increased amplitude and frequency of GnRH pulses
- Increased GnRH → increased gonadotropins → increased gonadal steroids
Key Neuroendocrine Regulators (gatekeepers):
- Kisspeptin and Neurokinin B are implicated as gatekeepers for puberty onset
- Metabolic modifiers: Leptin and nesfatin-1 can alter the actions of these gatekeepers
(Berek & Novak's Gynecology, p. 319-320)
Adrenarche
- Adrenarche refers to activation of the adrenal glands - the increase in adrenal androgen secretion (DHEA, DHEAS) that begins at ages 6-8 years
- Precedes and is independent of gonadarche (HPG axis activation)
- Responsible for early pubic and axillary hair, body odor, and early acne
Bone Age
- Bone/skeletal age is estimated from x-rays of the nondominant hand, knee, or elbow compared to standards (Greulich and Pyle atlas)
- Skeletal age correlates more closely with pubertal stage than with chronological age
- Used with height and chronological age to predict final adult height (Bayley-Pinneau tables)
- Midparental height formula: Add 13 cm to mother's height (for boys) or subtract 13 cm from father's height (for girls); average with other parent's height; ±8.5 cm gives the 3rd to 97th percentile range
(Berek & Novak's Gynecology, p. 315)
Aberrations of Pubertal Development (Novak's Table 8-1)
Delayed/Interrupted Puberty:
- Most common cause: Constitutional Delay of Growth and Development (CDGD) - strong genetic component, represents an extreme of normal distribution
- Anatomic: Mullerian agenesis, imperforate hymen, transverse vaginal septum
- Hypergonadotropic (FSH >30 mIU/mL) hypogonadism: Turner syndrome, pure gonadal dysgenesis (46,XX or 46,XY)
- Hypogonadotropic (LH and FSH <10 mIU/mL) hypogonadism
- Also consider celiac disease, Crohn's disease, sickle cell anemia, cystic fibrosis
PART 2: PREMENSTRUAL SYNDROME (PMS) AND PMDD
(Berek & Novak's Gynecology, Chapter 23, p. 1101-1103)
Definition and Epidemiology
- PMS has been characterized by more than 100 different physical and psychological signs and symptoms, making it difficult to define scientifically
- The distinction from PMDD is important: PMDD is a more severe, psychiatrically defined disorder
- PMDD affects an estimated 3-5% of ovulating women
- Symptoms must be in the luteal phase and resolve with or shortly after onset of menses
Pathophysiology
- No specific serum hormone level is directly associated with premenstrual dysphoria
- A subgroup of women is vulnerable not to absolute hormone levels, but to hormonal changes (fluctuations in estrogen and progesterone)
- There is a correlation between the degree of hormonal change and incidence of mood disorder
- Serotonergic dysregulation is the leading hypothesis - abnormal CNS response to normal fluctuations of ovarian steroids, particularly progesterone metabolites (allopregnanolone) acting on GABA-A receptors
Diagnosis of PMDD (DSM-5 Criteria)
- In the majority of menstrual cycles, at least 5 symptoms must be present during the premenstrual week
- Symptoms start to improve within a few days after onset of menses
- Symptoms become minimal or absent in the postmenstrual week
At least one of these must be present (core mood symptoms):
- Marked affective lability
- Marked irritability/anger/interpersonal conflict
- Marked depressed mood/hopelessness/self-deprecating thoughts
- Marked anxiety/tension
Additional symptoms (from this list):
- Decreased interest in usual activities
- Difficulty in concentration
- Lethargy
- Marked change in appetite
- Hypersomnia or insomnia
- A sense of being overwhelmed or out of control
- Physical symptoms: bloating, breast tenderness
Requirements:
- Symptoms must markedly interfere with work, family, or academic responsibilities
- Must not be exacerbations of another existing disorder
- Must be corroborated by at least 2 months of prospective daily ratings
- Screen for domestic abuse and other contributing life circumstances
(Berek & Novak's Gynecology, p. 1102)
Treatment of PMS
No treatment for PMS has been validated by empirical studies. Lifestyle interventions:
- Elimination of caffeine from the diet
- Smoking cessation
- Regular exercise
- Regular meals with complex carbohydrates
- Adequate sleep
- Stress reduction (meditation, yoga, delegating responsibilities)
Treatment of PMDD (Novak's Table 23-2)
| Category | Options |
|---|---|
| Antidepressants (SSRIs/SNRIs) | Fluoxetine 20 mg/day; Sertraline 50-150 mg/day; Paroxetine CR 12.5-25 mg/day; Citalopram 5-20 mg/day; Venlafaxine 75 mg/day; Clomipramine 25-75 mg/day |
| Ovulation suppression | Ethinyl estradiol 20 mcg/drospirenone 3 mg (Yaz); Transdermal estrogen; Leuprolide 3.75-7.5 mg IM monthly; Danazol 200-400 mg/day |
| Other medications | Alprazolam 0.25 mg BID during luteal phase; Bromocriptine; Spironolactone |
| Nonpharmacologic | Calcium 600 mg twice daily; Chasteberry (Vitex agnus-castus); Cognitive behavioral therapy |
(Berek & Novak's Gynecology, p. 1103)
FDA-approved SSRIs for PMDD: Fluoxetine, Sertraline, Paroxetine
RECENT UPDATES: ACOG CLINICAL PRACTICE GUIDELINE No. 7 (December 2023)
PMID: 37973069 | Obstetrics & Gynecology 142(6):1516-1533
This is the most current evidence-based guideline. Key recommendations:
Strong Recommendations
| Recommendation | Strength | Evidence Quality |
|---|---|---|
| SSRIs for management of affective premenstrual symptoms | STRONG | MODERATE |
| Combined oral contraceptives (COCs) for overall premenstrual symptoms | STRONG | LOW |
| Cognitive behavioral therapy (CBT) for affective premenstrual symptoms | STRONG | LOW-TO-MODERATE |
Conditional Recommendation
| Recommendation | Strength | Evidence Quality |
|---|---|---|
| GnRH agonists with combined hormonal add-back therapy for adults with severe, refractory premenstrual symptoms | SUGGEST (conditional) | - |
Key ACOG 2023 Points
- SSRIs are first-line pharmacologic treatment for PMDD - supported by multiple RCTs. Both continuous daily dosing and luteal-phase dosing (days 14-28) are effective.
- COC containing drospirenone (e.g., Yaz - EE 20 mcg + drospirenone 3 mg) has FDA approval for PMDD.
- Multimodal approach is recommended - combining lifestyle, pharmacologic, and psychological interventions.
- Diagnosis requires prospective symptom tracking - at least 2 months of daily ratings using validated tools (DRSP - Daily Record of Severity of Problems; PAF - Premenstrual Assessment Form).
- GnRH agonists (with add-back estrogen-progestin) reserved for severe, refractory cases; add-back therapy required to prevent hypoestrogenic side effects.
- Recommendations apply to both adults and adolescents (with caveats - limited specific evidence in adolescents).
- Surgical management (bilateral oophorectomy): last resort for truly refractory cases; requires discussion of hormonal add-back therapy post-surgery.
Approach to Management (ACOG 2023 Stepwise)
Step 1: Confirm diagnosis with prospective symptom tracking x 2 months
Step 2: Lifestyle/behavioral interventions (exercise, diet, CBT)
Step 3: First-line pharmacologic → SSRIs ± COCs
Step 4: Second-line → GnRH agonists with add-back therapy
Step 5: Surgical (oophorectomy) - only for severe, refractory, definitive cases
Quick Mnemonics for DNB
Tanner stages (Breast): "Bud - Breast - Secondary mound - Mature" (S1 = none, S2 = bud, S3 = breast enlargement, S4 = secondary mound, S5 = mature)
PMDD DSM-5: "5 symptoms, 1 must be mood (AIDA: Affective lability, Irritability, Depressed mood, Anxiety), 2 months prospective, menstrual timing essential"
PMS treatment ladder (ACOG 2023): Lifestyle → SSRIs/COCs/CBT → GnRH agonist + add-back → Surgery
Sources:
- Berek & Novak's Gynecology, 16th Edition (ISBN 9781496380357) - Chapter 8 (Pediatric & Adolescent Gynecology, p. 311-327) and Chapter 23 (p. 1101-1103)
- ACOG CPG No. 7 (Dec 2023) - Management of Premenstrual Disorders, Obstet Gynecol 142(6):1516-1533
What are the collateral blood supply of uterus - reference no acid gynae and recent recommended updates
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Searching the Web
collateral blood supply uterus uterine artery ligation pelvic vascular anatomy gynecology
Reading File
Reading File
Reading Web Page
https://www.mdpi.com/2039-7283/14/1/5
Finding Sources
Searching PubMed
uterine blood supply collateral circulation pelvic arteries
Reading File
Reading File
Reading File
Loading Image
Reading File
The Table 5-4 mentioned on page 67 (collateral channels table) is in the section that I've already captured via the snippets. The key information is in the paragraph at line 2658 which showed the collateral channel table. Let me now compile the complete answer using all the data gathered.
Collateral Blood Supply of the Uterus
DNB Paper Answer - Berek & Novak's Gynecology + Recent Updates
Primary Blood Supply of the Uterus
Before understanding collaterals, the primary supply must be established:
- Uterine artery - the dominant supply; arises from the anterior division of the internal iliac (hypogastric) artery
- Travels medially in the superior aspect of the broad ligament with a characteristic corkscrew/tortuous pattern (allows expansion in pregnancy)
- Crosses over the ureter approximately 1 cm lateral to the internal cervical os ("water under the bridge" - ureter = water, uterine artery = bridge)
- Blood flow through uterine arteries increases to approximately 500 mL/min in late pregnancy
(Berek & Novak's Gynecology, p. 161-164)
Pelvic Blood Supply Diagram (Berek & Novak's Fig. 5-9)
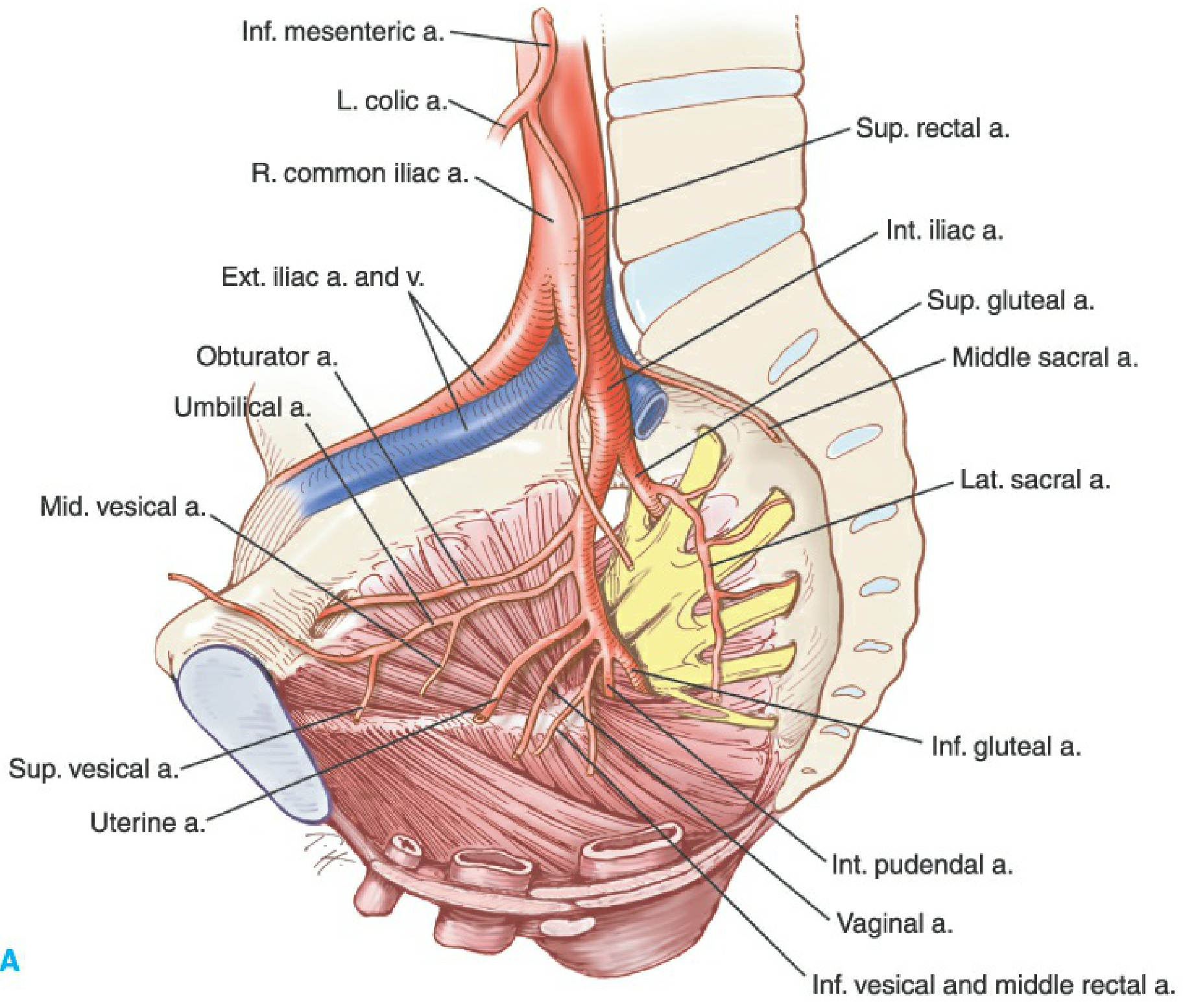
Figure 5-9A from Berek & Novak's Gynecology - Sagittal view of pelvic arterial supply showing uterine artery, internal iliac, ovarian artery, vaginal artery, and the major anastomotic channels.
Collateral Blood Supply of the Uterus
Principle of Pelvic Collateral Circulation
The pelvic vasculature is supplied with an extensive network of collateral connections that provides rich anastomotic communication between different major vessel systems. This redundancy ensures adequate oxygen and nutrient supply in major trauma or vascular compromise.
The clinical significance: Bilateral hypogastric (internal iliac) artery ligation - particularly when combined with ovarian artery ligation - dramatically reduces pulse pressure in the pelvis, converting flow from an arterial to a venous system and allowing collateral channels to continue blood supply to pelvic structures. Women have delivered normal infants in subsequent pregnancies after bilateral ligation of both hypogastric and ovarian arteries.
(Berek & Novak's Gynecology, p. 161 - General Principle No. 4)
Table: Collateral Channels of Circulation in the Pelvis (Novak's Table 5-4)
| Collateral Vessel | Anastomoses With |
|---|---|
| Ovarian artery (from aorta) | Uterine artery (from internal iliac) |
| Superior rectal artery (from inferior mesenteric artery) | Middle rectal artery (from internal iliac) |
| Lateral sacral arteries (from internal iliac - posterior division) | Median sacral artery (from aorta) |
| Iliolumbar artery (from internal iliac - posterior division) | 4th lumbar artery (from aorta) |
| Deep circumflex iliac artery (from external iliac) | Superior gluteal artery (from internal iliac) |
| Inferior epigastric artery (from external iliac) | Superior epigastric artery (from internal mammary) |
(Berek & Novak's Gynecology, Chapter 5 - Anatomy, Table 5-4, p. 167)
Detailed Collateral Pathways
1. Ovarian Artery ↔ Uterine Artery (Most Important)
- The ovarian artery arises from the ventral surface of the abdominal aorta, just below the origin of the renal vessels
- It travels as part of the infundibulopelvic (suspensory) ligament into the broad ligament
- It anastomoses freely with the uterine artery in the mesosalpinx and broad ligament
- This bidirectional anastomosis provides the most important collateral channel to the uterus
- Clinical relevance: When the uterine artery is ligated (O'Leary stitch), blood supply is maintained via the ovarian artery; conversely in UAE, residual supply may come from ovarian artery branches
2. Superior Rectal Artery ↔ Middle Rectal Artery
- Superior rectal artery = terminal branch of the inferior mesenteric artery
- Middle rectal artery = branch of the internal iliac artery
- This anastomosis becomes active after internal iliac artery (IIA) ligation above the posterior division
- Provides indirect collateral to the uterus via cervical/vaginal branches
3. Lateral Sacral ↔ Median Sacral (Primary after IIA ligation)
- Lateral sacral arteries arise from the posterior division of the internal iliac
- They anastomose with the median sacral artery (a direct branch of the aorta)
- Burchell's studies (pelvic aortograms in 22 patients) demonstrated this is the first and main anastomosis activated after IIA ligation below the posterior division
- Provides important indirect collateral support
4. Iliolumbar Artery ↔ 4th Lumbar Artery
- Iliolumbar artery arises from the posterior division of the internal iliac
- Anastomoses with the 4th lumbar artery (from the aorta)
- This is the second most important anastomosis activated after IIA ligation
- Together with the lateral sacral/median sacral anastomosis, these are the two primary groups of collateral channels (Burchell's landmark contribution)
5. Deep Circumflex Iliac ↔ Superior Gluteal
- Deep circumflex iliac arises from the external iliac artery
- Anastomoses with superior gluteal and 4th lumbar artery branches
- Provides systemic-systemic collateral circulation
6. Vaginal Artery ↔ Uterine Artery
- The vaginal artery (branch of internal iliac, or sometimes directly from uterine artery) anastomoses with descending branches of the uterine artery
- Provides important collateral to the lower uterine segment and cervix
Anatomic Variation - An Important Surgical Caveat
There is significant anatomic variation between individuals in the branching pattern of the internal iliac vessels:
- No constant order in which branches divide from the parent vessel
- Some branches may arise as common trunks or from other branches
- Obturator artery may arise from the external iliac or inferior epigastric artery
- Ovarian arteries may arise from the renal arteries or as a common trunk
- Inferior gluteal may originate from the posterior or anterior branch of internal iliac
- Blood flow patterns may be asymmetric from side to side
The pelvic surgeon must always be prepared for deviations from textbook vascular patterns.
(Berek & Novak's Gynecology, p. 161 - General Principle No. 2)
Clinical Surgical Applications
O'Leary Uterine Artery Ligation
- Bilateral ligation of uterine arteries at their origin from internal iliac (used in PPH)
- Reduces uterine blood flow by ~80%
- Blood supply maintained via ovarian artery anastomosis
Bilateral Internal Iliac (Hypogastric) Artery Ligation
- Reduces pulse pressure in pelvic vasculature by ~85%
- Converts arterial flow characteristics to venous (pressure reduction, not flow cessation)
- Collateral channels (lateral sacral/median sacral and iliolumbar/4th lumbar - Burchell's groups) allow continued pelvic perfusion
- Successful pregnancies reported after bilateral IIA + ovarian artery ligation
- Modern practice increasingly favors uterine artery embolization (UAE) or balloon occlusion over IIA ligation
Uterine Artery Embolization (UAE)
- Particle embolization via uterine arteries occludes fibroids' blood supply
- After UAE, collateral circulation (especially via ovarian artery) can re-establish uterine blood supply over time (relevant for UAE failure rates and fibroid recurrence)
- Bilateral UAE is needed because of collateral reconstitution
Recent Updates (2024-2025)
Burchell's Contribution (Historical but Exam-Important)
Burchell's pelvic aortography studies demonstrated that the two primary anastomotic groups activated after IIA ligation are:
- Lateral sacral arteries ↔ Median sacral artery
- 4th lumbar artery ↔ Iliolumbar artery
This corrected the earlier misconception that collaterals mainly came from external iliac and gluteal branches.
Current Evidence on IIA Ligation (MDPI 2025 Review - Gynecology 2025;14(1):5)
- IIA ligation is increasingly replaced by selective arterial embolization and temporary balloon occlusion (preoperative or intraoperative)
- IIA ligation is rarely described in textbooks now - surgeons must be familiar with anatomy before attempting
- Complications include: buttock claudication, impotence, bladder and rectal necrosis (rare if collaterals are intact)
- No long-term consequences of properly performed IIA ligation - women have delivered normal infants subsequently (Creasy & Resnik's MFM)
After Uterine Artery Ligation (UAL)
After UAL, uterine blood supply can return to normal due to establishment of collateral circulation and absorption of intraoperative sutures - making it suitable for women desiring future fertility (published evidence in PMC 2022).
Summary Table for Rapid Revision
| Collateral | From | To | Importance |
|---|---|---|---|
| Ovarian a. ↔ Uterine a. | Aorta | Internal iliac | Most direct; active normally |
| Lateral sacral ↔ Median sacral | IIA posterior div. | Aorta | Primary after IIA ligation (Burchell Group 1) |
| Iliolumbar ↔ 4th lumbar | IIA posterior div. | Aorta | Primary after IIA ligation (Burchell Group 2) |
| Superior rectal ↔ Middle rectal | Inf. mesenteric | Internal iliac | Active after IIA ligation above posterior division |
| Deep circumflex iliac ↔ Sup. gluteal | External iliac | IIA | Systemic-systemic |
| Vaginal a. ↔ Uterine a. | IIA (vaginal a.) | Uterine a. | Lower segment/cervical |
Sources:
- Berek & Novak's Gynecology, 16th Edition (ISBN 9781496380357) - Chapter 5 (Anatomy), pp. 161-167; General Principles No. 2, 3, 4; Table 5-4 Collateral Channels; Figure 5-9
- Imaging Anatomy Atlas Vol. 3 (ISBN 9781626239845) - Uterine Artery section
- Burchell RC - Pelvic vascular studies (historical landmark)
- IIA Ligation Review 2025 - Gynecology 2025;14(1):5
- Creasy & Resnik's Maternal-Fetal Medicine - Collateral circulation and PPH management
Hey
Hey! How can I help you?
This is a shared conversation. Sign in to Orris to start your own chat.