Management of schizophrenia
Reading File
Finding Sources
Searching PubMed
"schizophrenia"[MeSH Terms] AND "antipsychotic agents"[MeSH Terms]
Searching the Web
schizophrenia management guidelines 2024 2025 antipsychotics psychosocial
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Reading File
I now have enough comprehensive information. Let me compile the full, detailed response.
Management of Schizophrenia
A structured approach to schizophrenia management covers three domains: pharmacological treatment (antipsychotics), psychosocial interventions, and physical health monitoring. Treatment must be individualized, staged by episode type, and sustained long-term.
1. Classification of Antipsychotics
Antipsychotics are broadly divided into:
- First-Generation Antipsychotics (FGAs / "typicals"): e.g. haloperidol, chlorpromazine, fluphenazine, trifluoperazine. High D2 blockade, high extrapyramidal side-effect (EPSE) risk. Piperazine phenothiazines and butyrophenones carry the highest EPS risk.
- Second-Generation Antipsychotics (SGAs / "atypicals"): e.g. olanzapine, risperidone, quetiapine, aripiprazole, amisulpride, paliperidone, lurasidone, ziprasidone. Lower EPSE risk at therapeutic doses; broader receptor profiles.
- Clozapine: The only truly "atypical" SGA with near-zero EPSE liability and superior efficacy in treatment-resistant schizophrenia (TRS). Reserved due to the risk of agranulocytosis.
The real distinction between FGAs and SGAs is the ability to choose a dose within the licensed range that is effective without causing EPSEs. - The Maudsley Prescribing Guidelines in Psychiatry, 15th ed.
2. Treatment Algorithm (First-Episode Schizophrenia)
The algorithm below is from Maudsley Prescribing Guidelines:
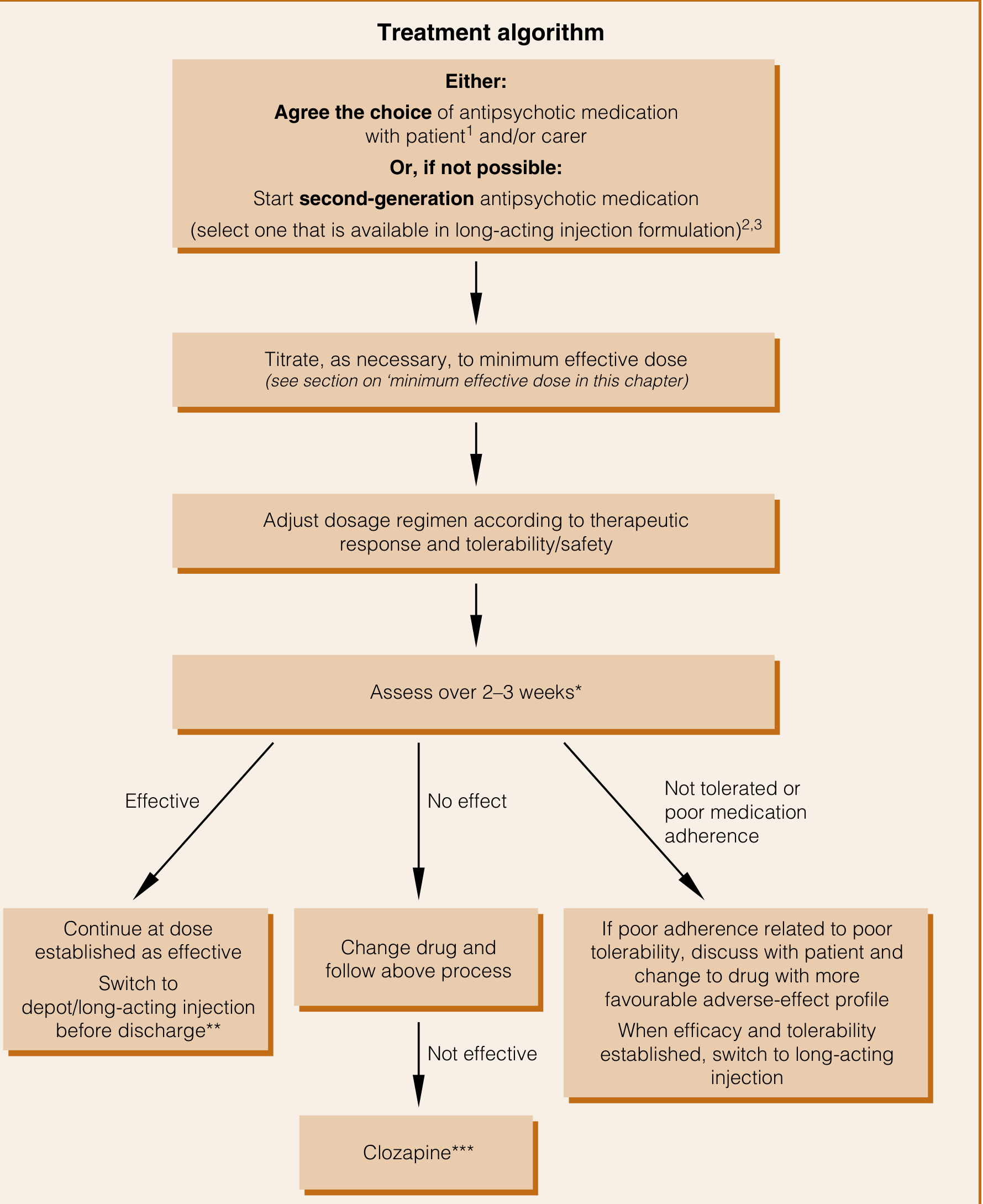
Step 1 - Agree drug choice with patient (or start an SGA if agreement is not possible). Preferably select one available in a long-acting injection (LAI) formulation.
Step 2 - Titrate to the minimum effective dose. Adjust based on therapeutic response and tolerability.
Step 3 - Assess over 2-3 weeks:
- Effective → Continue at established dose; switch to depot/LAI before discharge.
- No effect → Change drug and repeat the process. If still not effective → Clozapine.
- Not tolerated / poor adherence → Switch to a drug with a more favourable adverse-effect profile; then convert to LAI once efficacy and tolerability are established.
Drug choice notes:
- FGAs should probably be reserved for 2nd- or 3rd-line use given higher TD and EPS risk and possibly poorer outcomes vs SGAs.
- Choice should be based primarily on the comparative adverse-effect profile.
- Patients given informed choice tend to have better outcomes.
- Where prior treatment failure has occurred (but not confirmed TRS), olanzapine or risperidone are better options than quetiapine.
- Olanzapine, given the wealth of evidence for slight superiority, should generally be tried before clozapine.
3. Multi-Episode Schizophrenia and Maintenance Treatment
- The majority of patients with one episode will have further episodes; with each relapse, baseline function deteriorates - most of this decline occurs in the first decade of illness.
- Suicide risk (10%) is concentrated in the first decade.
- Antipsychotics taken regularly protect against relapse in the short and medium term.
- Targeted treatment (only when symptoms re-emerge) produces a worse outcome than prophylactic treatment.
- Optimal prophylactic dose: 5 mg/day risperidone equivalents. Higher doses offer no benefit and worsen tolerability.
- Doses that are acutely effective should generally be continued as maintenance.
Depot / Long-Acting Injectable (LAI) Antipsychotics
Non-adherence among people with schizophrenia is extremely high: ~25% are partially/non-adherent within 10 days of discharge, 50% at 1 year, and 75% at 2 years. Non-adherence increases relapse risk, severity, and suicide attempts four-fold.
- Meta-analyses show that depot/LAI maintenance treatment reduces relative risk of relapse by 30% and absolute risk by 10% compared with oral treatment.
- LAIs should be offered to:
- Patients who would prefer them after an acute episode
- Patients known to be non-adherent to oral treatment
Given low rates of adherence and the near-certainty of relapse if antipsychotics are not taken, the routine use of oral antipsychotics is difficult to justify. - The Maudsley Prescribing Guidelines in Psychiatry, 15th ed.
4. Treatment-Resistant Schizophrenia (TRS)
Definition: Failure to respond adequately despite adequate trials (correct dose, correct duration, confirmed adherence) of at least two different antipsychotics - at least one of which should be a non-clozapine SGA.
Before diagnosing TRS, always:
- Confirm adherence (check plasma drug levels - absolute non-adherence with zero blood levels is surprisingly common)
- Exclude substance use (including alcohol) as a confounding factor
- Review co-prescribed medications and physical illness
Clozapine - The Gold Standard for TRS
- Evidence supporting clozapine in TRS is overwhelming.
- Clozapine should be started at 6.25 mg (effective test dose), then titrated slowly to achieve a target plasma level of ~350 mcg/L over approximately 3 weeks.
- Target doses vary by sex, smoking status, and genetic CYP1A2 activity (e.g. Asian patients metabolise clozapine more slowly and require lower doses).
- Mandatory monitoring: FBC for agranulocytosis (weekly for 18 weeks, then fortnightly, then monthly).
Clozapine-Resistant Schizophrenia
Options when clozapine at optimised dose is still inadequate:
- Add a second antipsychotic to augment (adequate trial = 8-10 weeks; choose a drug that does not compound clozapine's adverse effects - e.g. avoid metabolically problematic agents)
- ECT augmentation - meta-analyses suggest benefit; some RCTs show ~50% of patients achieve response with ECT + clozapine vs none with clozapine alone. Evidence quality is moderate and results are mixed; ECT + clozapine is generally well tolerated (transient amnesia, headache, nausea as main adverse effects)
5. Managing Suboptimal Response: Dose Increase, Switch, or Augment?
When current treatment is suboptimal, four options exist:
- Increase the dose - evidence is limited; higher doses risk more adverse effects
- Switch antipsychotic - often the most practical step
- Add an adjunctive medication - limited evidence base
- Wait and monitor - reasonable if external factors are expected to improve
Always optimise the minimum effective dose before escalating. For SGAs, recommended doses are based on rigorous fixed-dose trials; navigate within licensed ranges rather than pushing above them.
6. Side Effect Management
Metabolic Effects (Diabetes, Weight Gain)
- Schizophrenia itself carries elevated rates of insulin resistance even before antipsychotic exposure.
- Clozapine and olanzapine carry the highest risk of hyperglycaemia, impaired glucose tolerance, and diabetic ketoacidosis (DKA) - risk from clozapine may reach one-third of patients after 5 years.
- Risperidone / paliperidone / amisulpride cause the most prolactin elevation.
- Lifestyle interventions (diet, weight management, physical activity) should be offered to all patients.
- Monitor: fasting glucose, HbA1c, lipids, weight/BMI, blood pressure.
Extrapyramidal Side Effects (EPSEs)
- Tardive dyskinesia (TD): Switch to clozapine, olanzapine, quetiapine, or a D2 partial agonist. Consider vesicular monoamine transporter 2 (VMAT2) inhibitors (valbenazine, deutetrabenazine) if switch is not possible.
- Parkinsonism: Dose reduction or switch to a weaker D2 antagonist or partial agonist. Adjunctive anticholinergics are not routinely recommended.
- Akathisia: Dose reduction; switch to quetiapine or olanzapine; adjunctive propranolol (10-30 mg bid/tid) or mirtazapine 15 mg daily.
Hyperprolactinaemia
- Most common with risperidone, paliperidone, amisulpride.
- If symptomatic (galactorrhoea, sexual dysfunction): switch to a dopamine partial agonist (aripiprazole, cariprazine) or add adjunctive aripiprazole 5 mg daily.
- Counsel about risks of untreated asymptomatic hyperprolactinaemia (reduced bone density, increased breast cancer risk in women).
7. Psychosocial Interventions
Medications should always be combined with psychosocial treatments:
| Intervention | Indication / Notes |
|---|---|
| Cognitive Behavioural Therapy for Psychosis (CBTp) | Reduces positive symptoms; recommended by NICE for all patients |
| Family interventions | Reduce relapse rates; target high expressed emotion |
| Assertive Community Treatment (ACT) | For patients with frequent hospitalisations / high service use |
| Supported employment (IPS) | Improves vocational outcomes significantly |
| Social skills training | Improves functioning and reduces negative symptoms |
| Cognitive remediation | Targets cognitive deficits; evidence growing |
| Early Intervention Services | First-episode psychosis; significantly improves long-term outcomes |
A recent Lancet Psychiatry network meta-analysis (2024) confirmed that psychological and psychosocial interventions have significant benefit in TRS.
8. Physical Health Monitoring
People with schizophrenia have a 15-20 year reduction in life expectancy, mainly due to cardiovascular disease and metabolic syndrome. Annual physical health checks must include:
- Weight, BMI, waist circumference
- Blood pressure
- Fasting glucose / HbA1c
- Fasting lipids
- ECG (particularly for drugs prolonging QTc: haloperidol, ziprasidone, sertindole)
- Prolactin level (if symptomatic)
- FBC (mandatory for clozapine)
- Smoking status and cessation support
- Substance use review
9. Duration of Treatment
| Situation | Recommended Duration |
|---|---|
| First episode | Minimum 1-2 years after remission (NICE); 2-5 years (RANZCP); 18 months (Canadian guidelines) |
| Multi-episode | Indefinite maintenance therapy is usually warranted |
| Treatment-resistant | Lifelong clozapine in most cases |
Summary - Key Principles
- Start with an SGA - agree choice with patient; prefer one available as LAI.
- Use minimum effective dose - equivalent to ~5 mg risperidone/day for maintenance.
- Convert to LAI early - non-adherence is universal; LAI reduces relapse risk by 30% relative to oral.
- Two adequate trials failed → clozapine - confirm adherence first; ensure at least one prior drug was olanzapine.
- Monitor metabolic and physical health at every stage.
- Always combine with psychosocial treatments - medications alone are insufficient.
- Clozapine-resistant patients: augment with a second antipsychotic or consider ECT.
Recent Evidence Update
- A 2025 JAMA Psychiatry network meta-analysis (PMID 39412783) found differential effects of antipsychotics on cognitive function - clinically relevant when choosing agents.
- A 2025 Lancet Psychiatry international guideline (INTEGRATE) provides updated algorithmic treatment guidance with akathisia, TD, and hyperprolactinaemia management recommendations largely consistent with the above.
Sources: The Maudsley Prescribing Guidelines in Psychiatry, 15th Edition; Kaplan and Sadock's Synopsis of Psychiatry; NICE Guidelines; INTEGRATE International Guideline (Lancet Psychiatry, 2025); PubMed literature.
This is a shared conversation. Sign in to Orris to start your own chat.