thorat allergy type
Reading File
Finding Sources
Finding Sources
Searching the Web
throat allergy types hypersensitivity reactions pharyngitis IgE
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Here is a thorough breakdown of throat allergy types, organized by the Gell and Coombs hypersensitivity classification used in clinical medicine:
Throat Allergy - Types of Hypersensitivity Reactions
Throat involvement in allergic reactions falls under the broader framework of hypersensitivity reactions, classified by Gell and Coombs into four types. The throat (pharynx/larynx) can be affected by all four, but most clinical "throat allergies" are Type I.
The Four Types (Gell & Coombs Classification)
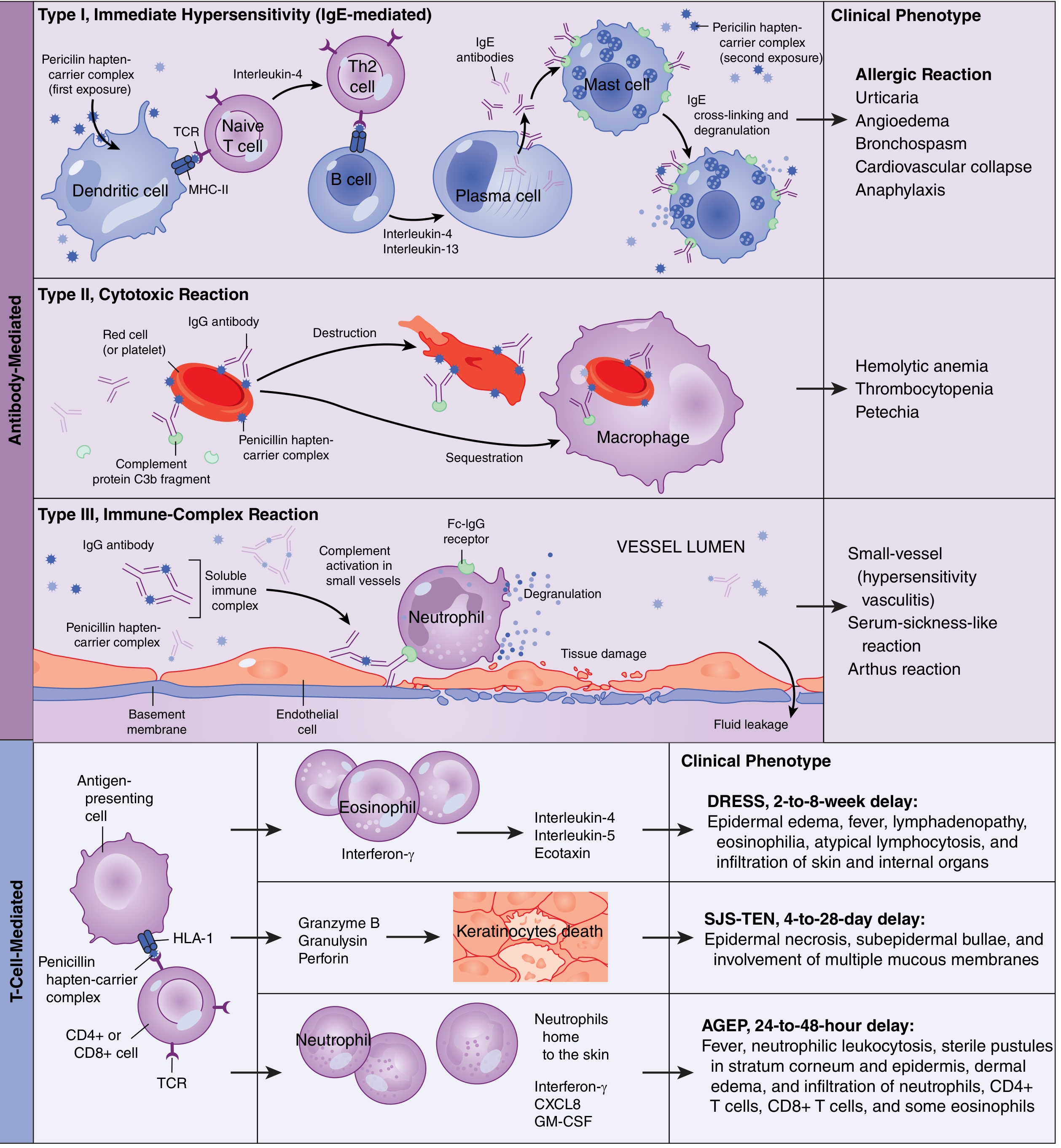
Type I - Immediate Hypersensitivity (Most Common "Throat Allergy")
- Mediator: IgE antibodies
- Mechanism: On first allergen exposure, Th2 cells drive B cells to produce IgE, which coats mast cells. On re-exposure, the allergen cross-links IgE on mast cells, causing degranulation and release of histamine, leukotrienes, and prostaglandins.
- Throat symptoms: Throat tightness, itching/pruritus of the throat, angioedema of the pharynx/larynx, swelling
- Onset: Within minutes (< 1 hour)
- Common triggers: Pollen (trees: Feb-May; grasses: Apr-Aug; weeds: Jul-frost), animal dander, molds (inhalants), foods, drugs, insect venom
- Associated conditions: Allergic rhinitis with post-nasal drip irritating the throat, asthma, angioedema, anaphylaxis
- Most severe form: Laryngeal angioedema in anaphylaxis - can be life-threatening
Type II - Cytotoxic Reaction
- Mediator: IgG and IgM antibodies bind to cell-surface antigens
- Mechanism: Antibody-antigen complexes on cell surfaces activate complement (C3b) and recruit macrophages/NK cells, leading to cell destruction
- Throat relevance: Rare direct throat involvement. Seen with certain drug reactions affecting mucous membranes (e.g., pemphigus affecting oral/pharyngeal mucosa), transfusion reactions
- Examples: Hemolytic anemia, thrombocytopenia, Hashimoto thyroiditis
Type III - Immune Complex-Mediated Reaction
- Mediator: IgG/IgM antibodies form soluble immune complexes with antigens
- Mechanism: Immune complexes deposit in vessel walls, activate complement, recruit neutrophils, causing local inflammation (Arthus reaction) and tissue injury
- Throat relevance: Serum sickness can cause pharyngeal inflammation, arthralgia, and fever. Vasculitis may affect throat mucosa.
- Examples: Serum sickness, SLE, rheumatoid arthritis
Type IV - Cell-Mediated (Delayed) Hypersensitivity
- Mediator: Sensitized T lymphocytes (Th1 cells) - NO antibodies involved
- Mechanism: T cells recognize antigen, recruit more lymphocytes and macrophages to the site; reaction takes 48-72 hours (up to 3 days) to develop
- Throat relevance: Contact reactions to inhaled or ingested chemicals, certain drug reactions (e.g., Stevens-Johnson syndrome involving oral/pharyngeal mucosa)
- Examples: Contact dermatitis, SJS/TEN (affects mucous membranes including throat), DRESS syndrome, PPD test reaction
Summary Table
| Type | Name | Key Antibody/Cell | Onset | Throat Manifestations |
|---|---|---|---|---|
| I | Immediate/Atopic | IgE + Mast cells | < 1 hour | Itchy throat, tightness, angioedema, anaphylaxis |
| II | Cytotoxic | IgG, IgM + Complement | Hours | Rare - drug-induced mucosal damage |
| III | Immune Complex | IgG/IgM complexes | 6-24 hours | Pharyngeal inflammation in serum sickness |
| IV | Delayed/Cell-Mediated | T cells (no antibody) | 48-72 hours | SJS mucosal involvement, contact reactions |
Allergic Trigger Categories (for Throat Allergy)
From K.J. Lee's Essential Otolaryngology, these are the main allergen categories:
- Inhalants - pollen, animal dander, molds (most common cause of allergic rhinitis/throat symptoms)
- Ingestants - foods, medications
- Injectants - drugs, insect venom
- Contactants - nickel, poison ivy, topical medications
Diagnostic Testing for Throat/Airway Allergy
- Skin prick/puncture test - excellent screening, low false-positive rate
- Intradermal dilutional testing (IDT) - most common method used by otolaryngologists, highly sensitive
- RAST (in vitro) - measures serum allergen-specific IgE; more specific than skin testing
Treatment
- Antihistamines - block histamine H1 receptors (Type I)
- Corticosteroids - reduce inflammation across types
- Epinephrine - first-line for laryngeal angioedema/anaphylaxis
- Immunotherapy (subcutaneous or sublingual) - shifts immune response, increases IgG4, requires 3-5 years; treats the underlying sensitivity
Sources: Goldman-Cecil Medicine; Rosen's Emergency Medicine; K.J. Lee's Essential Otolaryngology - all via the medical textbook library
This is a shared conversation. Sign in to Orris to start your own chat.