Explain me 10 common heart disease with ecg changes and ECG diagram
ECG electrocardiogram changes heart disease myocardial infarction atrial fibrillation
STEMI inferior anterior ECG ST elevation myocardial infarction 12-lead
atrial flutter ventricular tachycardia ECG sawtooth pattern
Wolff-Parkinson-White syndrome ECG delta wave short PR interval left ventricular hypertrophy
complete heart block third degree AV block pericarditis hyperkalemia ECG
ventricular tachycardia wide QRS monomorphic polymorphic ECG torsades de pointes
pericarditis diffuse ST elevation saddle shape ECG PR depression
pulmonary embolism ECG S1Q3T3 right heart strain sinus tachycardia
left ventricular hypertrophy ECG Sokolow-Lyon voltage criteria tall R wave
hyperkalemia peaked T wave ECG sine wave widened QRS electrolyte
10 Common Heart Diseases with ECG Changes
1. 🫀 ST-Elevation Myocardial Infarction (STEMI)
ECG Changes
- Hyperacute T-waves (earliest sign — tall, peaked, broad-based)
- ST-segment elevation ≥1 mm in ≥2 contiguous leads (convex/tombstone morphology)
- Pathological Q waves (>40 ms wide, >25% of R-wave height) — appear within hours to days
- Reciprocal ST depression in opposite leads
- T-wave inversion in the subacute phase
| Infarct Territory | Elevated ST Leads | Reciprocal Depression |
|---|---|---|
| Anterior (LAD) | V1–V4 | II, III, aVF |
| Inferior (RCA) | II, III, aVF | I, aVL |
| Lateral (LCx) | I, aVL, V5–V6 | V1–V3 |
| Posterior | V7–V9 | V1–V3 (tall R) |
2. 🫀 Non-ST-Elevation Myocardial Infarction (NSTEMI) / Unstable Angina
ECG Changes
- ST depression (horizontal or downsloping) ≥0.5 mm in ≥2 contiguous leads
- T-wave inversion (symmetric, deep — Wellens' pattern in proximal LAD stenosis)
- No pathological Q waves (distinguishes from STEMI)
- No ST elevation (by definition)
- May have normal ECG in up to 6% of cases
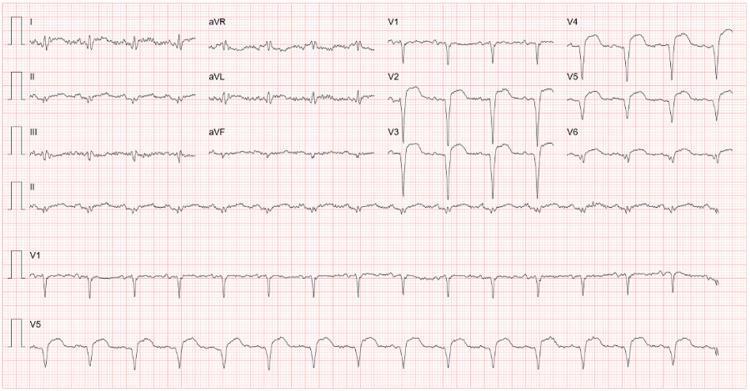
3. 🫀 Atrial Fibrillation (AF)
ECG Changes
- Absent P waves — replaced by chaotic fibrillatory (f) waves (especially visible in V1)
- Irregularly irregular RR intervals (the hallmark)
- Narrow QRS (unless aberrant conduction or bundle branch block)
- Ventricular rate variable: 100–180 bpm (uncontrolled), <100 bpm (rate-controlled)
- Coarse vs. fine fibrillatory baseline
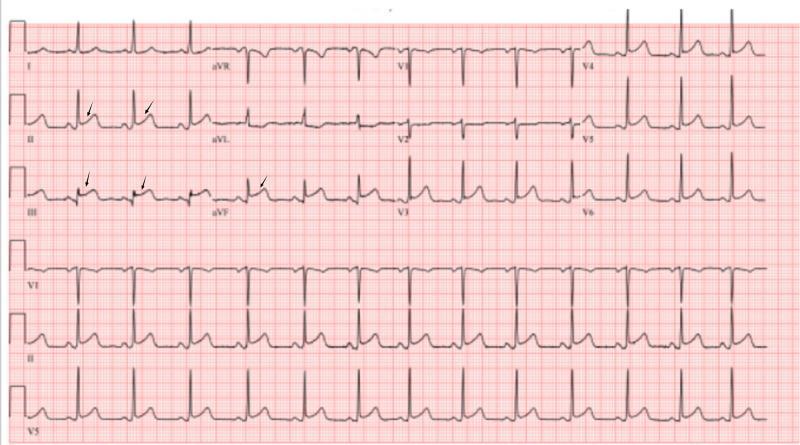
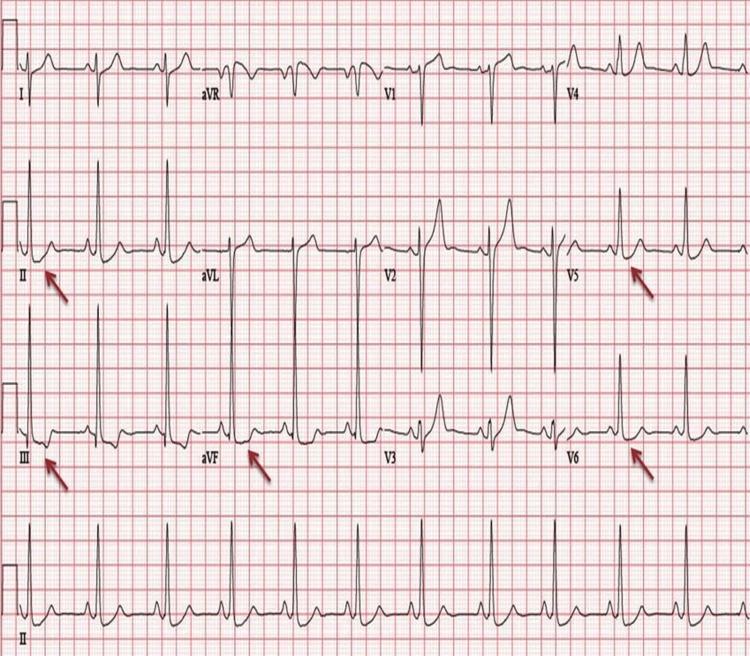
4. 🫀 Atrial Flutter
ECG Changes
- Sawtooth flutter (F) waves at ~300 bpm — best seen in II, III, aVF, and V1
- Regular atrial rate ~250–350 bpm (typical flutter ~300 bpm)
- AV conduction ratio typically 2:1 (ventricular rate ~150 bpm), may be 3:1 or 4:1
- Narrow QRS (unless aberrant conduction)
- No isoelectric baseline between flutter waves (distinguishes from multifocal atrial tachycardia)
5. 🫀 Third-Degree (Complete) Heart Block
ECG Changes
- Complete AV dissociation — P waves and QRS complexes are independent of each other
- P-wave rate > QRS rate (e.g., atrial rate 80 bpm, ventricular rate 30–45 bpm)
- No relationship between P waves and QRS complexes (PR interval varies)
- Escape rhythm: narrow QRS if junctional (40–60 bpm); wide QRS if ventricular (20–40 bpm)
- Bradycardia, often symptomatic

6. 🫀 Wolff-Parkinson-White (WPW) Syndrome
ECG Changes (Classic Triad)
- Short PR interval (<120 ms) — accessory pathway bypasses AV node delay
- Delta wave — slurred upstroke at the start of QRS (pre-excitation of ventricle)
- Wide QRS (>120 ms) — due to fusion of normal and accessory pathway depolarization
- Secondary ST-T changes — discordant to delta wave direction
- "Pseudo-infarction" pattern — negative delta waves in inferior leads can mimic Q waves

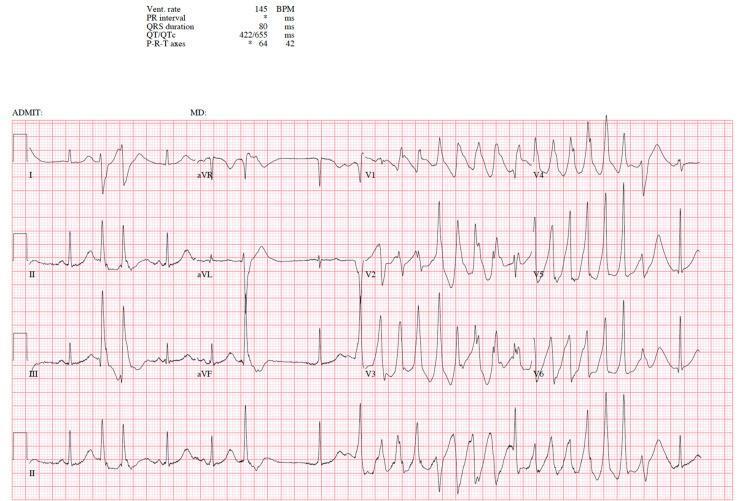
7. 🫀 Ventricular Tachycardia / Torsades de Pointes
ECG Changes — Monomorphic VT
- Wide QRS (>120 ms), rate 100–250 bpm
- Regular RR intervals
- AV dissociation, fusion beats, capture beats
- LBBB or RBBB morphology
ECG Changes — Torsades de Pointes (Polymorphic VT)
- "Twisting of the points" — QRS axis rotates around the isoelectric baseline
- Irregular, wide-complex tachycardia
- Preceded by long QTc (>500 ms), often with long-short-long RR sequence
- Can degenerate into ventricular fibrillation
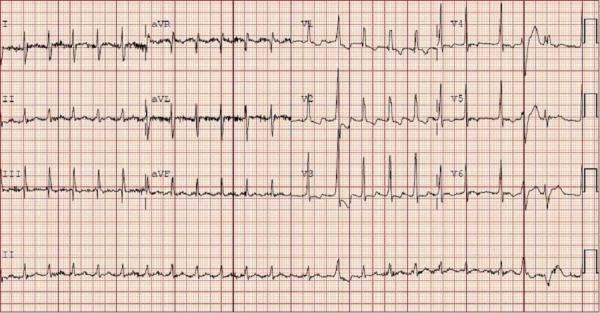
8. 🫀 Acute Pericarditis
ECG Changes (4 stages)
| Stage | Timing | ECG Finding |
|---|---|---|
| Stage 1 | Day 1–2 | Diffuse concave ("saddle-shaped") ST elevation + PR depression in most leads; PR elevation + ST depression in aVR |
| Stage 2 | Days–weeks | ST normalizes, T waves flatten |
| Stage 3 | Weeks | T-wave inversion (diffuse) |
| Stage 4 | Months | ECG normalizes |
- Diffuse ST elevation (not confined to one coronary territory)
- Spodick's sign — downsloping TP segment
- PR depression in leads II, V4–V6
- No reciprocal ST depression (except aVR)
- No Q waves

9. 🫀 Pulmonary Embolism (PE)
ECG Changes
- Sinus tachycardia (most common finding ~44%)
- S1Q3T3 pattern (McGinn-White sign): deep S in I, Q wave in III, T-wave inversion in III — present in ~12–20%
- Right bundle branch block (complete or incomplete) — rSR' in V1
- T-wave inversions in V1–V3 (right ventricular strain)
- Right axis deviation
- Atrial arrhythmias (AF, flutter)
- P pulmonale (peaked P >2.5 mm in II) — right atrial enlargement

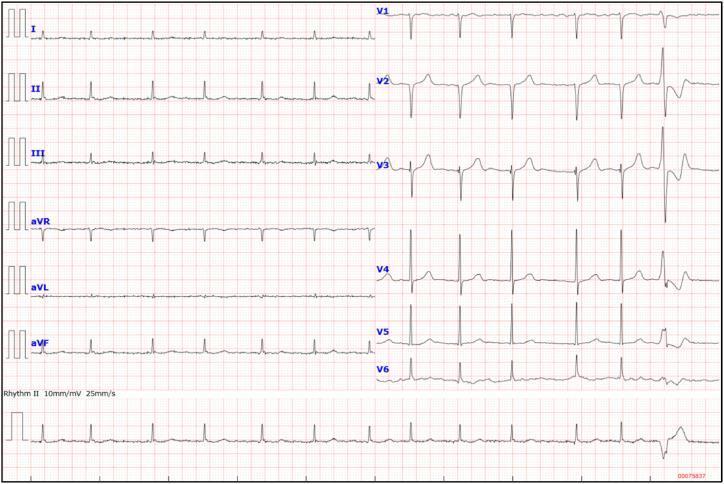
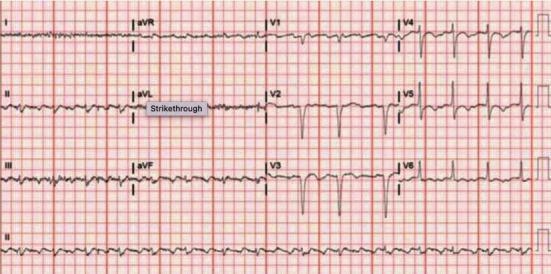
10. 🫀 Left Ventricular Hypertrophy (LVH) / Hypertensive Heart Disease
ECG Changes
- High-voltage QRS (Sokolow-Lyon criteria: S in V1 + R in V5 or V6 ≥35 mm)
- Cornell criteria: R in aVL + S in V3 >28 mm (men) / >20 mm (women)
- Left axis deviation
- ST depression + T-wave inversion in lateral leads (I, aVL, V5, V6) — the "strain pattern"
- Prolonged QRS duration
- Left atrial enlargement (biphasic P in V1 with deep terminal component)
| K+ Level | ECG Change |
|---|---|
| 5.5–6.5 mEq/L | Tall, peaked ("tented") T waves — narrow base |
| 6.5–8.0 mEq/L | Flattened/absent P waves, prolonged PR, wide QRS |
| >8.0 mEq/L | Sine-wave pattern → ventricular fibrillation → asystole |

Quick Reference Summary Table
| # | Disease | Key ECG Changes |
|---|---|---|
| 1 | STEMI | ST elevation, Q waves, reciprocal depression, hyperacute T |
| 2 | NSTEMI/UA | ST depression, T-wave inversion, no Q waves |
| 3 | Atrial Fibrillation | No P waves, irregularly irregular, f-waves |
| 4 | Atrial Flutter | Sawtooth F-waves ~300 bpm, 2:1–4:1 block |
| 5 | Complete Heart Block | AV dissociation, P rate > QRS rate, escape rhythm |
| 6 | WPW Syndrome | Short PR, delta wave, wide QRS, pseudoinfarction |
| 7 | VT / Torsades | Wide QRS tachycardia, twisting QRS axis (TdP), long QTc |
| 8 | Pericarditis | Diffuse saddle ST elevation, PR depression, no Q waves |
| 9 | Pulmonary Embolism | S1Q3T3, sinus tachycardia, T inversion V1–V3, RBBB |
| 10 | LVH / Hypertension | High voltage, strain pattern, left axis deviation |