Liver function test (Add mnemonic if possible)
liver function tests LFT mnemonic complete guide
Liver Function Tests (LFTs)
Mnemonic: "ABCDEFGHI" - a popular way to remember all LFT components:
Letter Test A Albumin / A:G ratio / Ammonia / Alpha-1 antitrypsin B Bilirubin (Total / Direct / Indirect) / Bile pigments / Bile salts C Cholesterol / Coagulation (PT, INR) D De Ritis ratio (AST:ALT) E Enzymes (ALT, AST, ALP, GGT) F Fibrinogen / Flocculation tests G GGT (Gamma-glutamyltransferase) H Hepatitis markers (HBsAg, anti-HCV) I INR / Immunoglobulins
Overview
Tests Grouped by Category
1. Tests of Liver Injury (Enzymes)
ALT (Alanine Aminotransferase)
- More specific for liver disease than AST
- AST is elevated in cardiac/skeletal muscle injury; ALT is not
- Markedly elevated in acute viral hepatitis (elevated days before jaundice appears)
- Primary use: sensitive indicator of hepatocellular damage
AST (Aspartate Aminotransferase)
- Less specific (also elevated in heart, skeletal muscle)
- AST > ALT suggests:
- Alcoholic liver disease (AST:ALT ratio typically >2:1 - the De Ritis ratio)
- Early hepatic injury
- Cirrhosis (mild elevations)
- Non-hepatic muscle injury
- Both AST and ALT >10x upper reference limit (URL) = acute hepatitis; lower values = chronic hepatitis
ALP (Alkaline Phosphatase)
- Elevated in obstructive (cholestatic) jaundice
- Also elevated in bone disease (not liver-specific alone - confirm with GGT)
- If ALP elevated in isolation, rule out non-hepatic sources (bone, placenta, intestine)
- ALP >2x URL with AST <3x URL = cholestatic pattern
GGT (Gamma-Glutamyltransferase)
- Rises in parallel with ALP in cholestasis
- Used to confirm that elevated ALP is of hepatic origin (not bone)
- Elevated by alcohol and enzyme-inducing drugs
- Prognostic indicator for cardiovascular and all-cause mortality; rising GGT associated with type 2 diabetes and metabolic syndrome
2. Tests of Hepatic Synthetic Function
Albumin
- Low in chronic liver disease (cirrhosis, chronic hepatitis)
- Half-life ~20 days, so does not reflect acute changes quickly
- Decreased albumin = indicator of chronicity and severity
- Can also be low in malnutrition, nephrotic syndrome, inflammation (not liver-specific)
- Serial measurements monitor disease progression
Prothrombin Time (PT) / INR
- Liver synthesizes clotting factors I, II, V, VII, IX, X
- Prolonged PT in acute liver failure (impaired synthesis)
- Key differentiator: if PT corrects after vitamin K injection (10 mg SC/IM, measure after 24h) - suggests cholestasis (malabsorption of fat-soluble vitamin K), not hepatocellular failure
- Indicator of severity of liver disease
3. Tests of Bilirubin Metabolism
Serum Bilirubin (Total, Direct, Indirect)
- Conjugated (direct) bilirubin elevated in: obstructive jaundice, cholestasis, hepatocellular disease
- Unconjugated (indirect) bilirubin elevated in: hemolysis, Gilbert syndrome, Crigler-Najjar
- In hepatocellular disease: both conjugated and unconjugated rise (failure of uptake, conjugation, and excretion)
- In obstructive jaundice: mainly conjugated rises
Quick rule: Conjugated = Can't get out (obstruction) Unconjugated = Can't get in/conjugated (hemolysis, enzyme deficiency)
4. Other Tests
| Test | Significance |
|---|---|
| Total Protein | Low in cirrhosis, chronic liver disease |
| Ammonia | Elevated in hepatic encephalopathy (impaired urea cycle) |
| Serum Cholesterol | Elevated in cholestasis; low in severe hepatocellular failure |
| Alpha-1 Antitrypsin | Deficiency causes cirrhosis and emphysema |
| LDH | Non-specific; elevated in hepatitis and many other conditions |
Interpretation Patterns
| Pattern | Key Finding | Likely Cause |
|---|---|---|
| Hepatocellular | AST/ALT >> ALP | Viral hepatitis, alcoholic hepatitis, drug-induced |
| Cholestatic | ALP/GGT >> AST/ALT | Bile duct obstruction, PBC, PSC |
| Mixed | Both elevated | Drug-induced, early/resolving hepatitis |
| Synthetic failure | Low albumin, prolonged PT | Cirrhosis, acute liver failure |
Diagnostic Algorithm
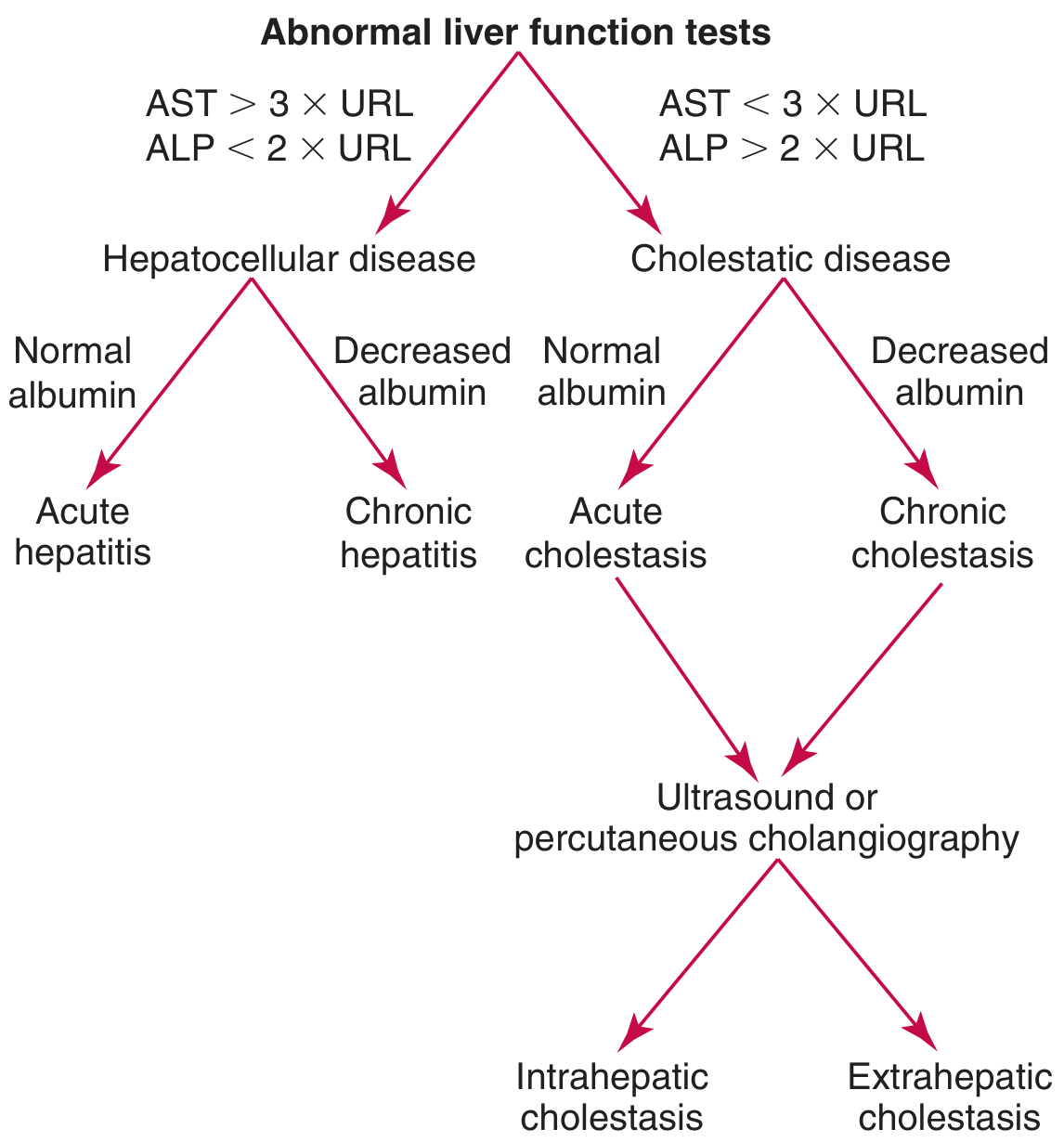
- AST >3x URL + ALP <2x URL → Hepatocellular disease
- Normal albumin → Acute hepatitis
- Low albumin → Chronic hepatitis
- AST <3x URL + ALP >2x URL → Cholestatic disease
- Then use ultrasound/cholangiography to differentiate intrahepatic vs. extrahepatic cholestasis
Quick Memory Aid: LFT Pattern Mnemonics
- ALT and AST rise markedly (>10x = acute hepatitis)
- Think "Blocked Bile" - ALP and GGT rise when bile can't flow
- >2:1 = Alcoholic liver disease
- <1:1 = Viral hepatitis or NAFLD
- PT prolonged
- Albumin low
- Coagulation factors impaired
- Think chronic disease or severe acute failure
Reference Ranges (approximate)
| Test | Normal Range |
|---|---|
| ALT | 7-56 U/L |
| AST | 10-40 U/L |
| ALP | 44-147 U/L |
| GGT | 9-48 U/L |
| Total Bilirubin | 0.2-1.2 mg/dL |
| Direct Bilirubin | 0.0-0.3 mg/dL |
| Albumin | 3.5-5.0 g/dL |
| Total Protein | 6.3-8.2 g/dL |
| PT | 11-13.5 seconds |
How do I interpret abnormal LFT patterns in specific diseases (hepatitis, cirrhosis, cholestasis)?
Interpreting Abnormal LFT Patterns in Specific Diseases
The Two Core Patterns - Master This First
| Feature | Hepatocellular | Cholestatic |
|---|---|---|
| Dominant rise | ALT, AST (>ALP) | ALP, GGT (>ALT, AST) |
| Key threshold | AST >3× URL, ALP <2× URL | AST <3× URL, ALP >2× URL |
| Bilirubin | Both conjugated + unconjugated raised | Mainly conjugated raised |
| Albumin/PT | Severely impaired in acute failure | May be normal initially |
| Think of | Hepatitis, drug toxicity, ischemia | Obstruction, PBC, PSC, drugs |
Disease-by-Disease LFT Interpretation
1. Acute Viral Hepatitis (A, B, C, D, E)
| Test | Finding |
|---|---|
| ALT | Markedly elevated (≥ AST); rises days before jaundice |
| AST | Elevated, but ALT ≥ AST |
| ALP | Mildly elevated or normal |
| Bilirubin | Elevated (both fractions) once jaundice appears |
| Albumin | Normal (acute = no time to deplete) |
| PT/INR | Normal unless severe/fulminant |
Key rule: ALT ≥ AST in viral hepatitis. Values >25× ULN are almost exclusively seen in acute hepatocellular disease.
2. Alcoholic Hepatitis
| Test | Finding |
|---|---|
| AST | Elevated, but rarely >300 U/L |
| ALT | Lower than AST |
| AST:ALT ratio | ≥2:1 (De Ritis ratio reversal) - in severe cases up to 4:1 |
| GGT | Often markedly elevated (elevated in 70% of chronic alcoholics; correlates with alcohol intake) |
| Bilirubin | Elevated |
| PT | May be prolonged |
Mnemonic: "Two Shots to One" - AST is TWO times ALT in alcoholic hepatitis.
- Alcoholic: AST:ALT ≥2:1, AST rarely >300 U/L
- Viral: ALT ≥ AST, transaminases often >500-1000 U/L
3. Non-Alcoholic Fatty Liver Disease (NAFLD) / NASH
| Test | Finding |
|---|---|
| ALT | Mildly-moderately elevated (usually <5× ULN) |
| AST | May be normal or mildly elevated; ALT>AST initially |
| ALP/GGT | Mildly elevated |
| Albumin/PT | Normal unless cirrhosis has developed |
Key point: NAFLD is one of the most common causes of incidentally elevated liver enzymes in the Western world. Do NOT diagnose NAFLD on enzymes alone - suspect it when metabolic risk factors (obesity, T2DM, hypertension, dyslipidemia) are present.
4. Drug-Induced Liver Injury (DILI)
| Type | LFT Pattern | Examples |
|---|---|---|
| Hepatocellular | ALT/AST >5× ULN dominant | Paracetamol, isoniazid, statins |
| Cholestatic | ALP >2× ULN dominant | Chlorpromazine, erythromycin estolate, anabolic steroids, OCP |
| Mixed | Both elevated | Many drugs |
- Predictable (dose-dependent): Classic example = paracetamol overdose. Causes extreme transaminase rise (>2000 U/L). Extreme elevation of LDH alongside extreme AST/ALT signals massive hepatic necrosis.
- Idiosyncratic: Not dose-dependent; minority of patients. Examples: isoniazid, halothane.
5. Cirrhosis (End-Stage Liver Disease)
| Test | Finding | Significance |
|---|---|---|
| ALT/AST | Normal or mildly elevated | Few hepatocytes left to lyse |
| AST:ALT ratio | >1 (reversal) | Fibrosis causes this flip |
| ALP/GGT | Elevated (biliary involvement) | |
| Albumin | Low | Best marker of chronicity/severity |
| PT/INR | Prolonged | Synthetic failure |
| Bilirubin | Elevated | Reflects severity |
| Platelets | Low (hypersplenism) | Portal hypertension |
| Ammonia | Elevated | Hepatic encephalopathy |
Mnemonic for cirrhosis: "LAPP" - Low albumin, AST>ALT, Prolonged PT, Platelets low
- Bilirubin, Albumin, PT, plus Ascites and Encephalopathy
- Score A (5-6) = compensated; Score C (10-15) = decompensated
6. Obstructive (Extrahepatic) Cholestasis
| Test | Finding |
|---|---|
| ALP | Markedly elevated (often >3-4× ULN) |
| GGT | Elevated in parallel with ALP |
| Conjugated bilirubin | Markedly elevated ("Can't get out") |
| ALT/AST | Mildly elevated or normal |
| Albumin | Normal early |
| PT | May be prolonged - corrects with vitamin K (malabsorption of fat-soluble vitamins) |
PT correction with Vitamin K = cholestasis, not hepatocellular failure. This is the key clinical differentiator.
7. Intrahepatic Cholestasis
| Test | Finding |
|---|---|
| ALP | Markedly elevated |
| GGT | Elevated |
| Bilirubin | Elevated (conjugated) |
| ALT/AST | Mildly elevated |
| Anti-mitochondrial Ab (AMA) | Positive in PBC (>90% sensitivity) |
| IgM | Elevated in PBC |
| ANCA, ANA | May be positive in PSC/AIH |
- PBC: Middle-aged woman, itching, fatigue, elevated ALP + AMA positive.
- PSC: Young man with IBD, elevated ALP + beaded appearance on MRCP.
8. Ischemic Hepatitis ("Shock Liver")
| Test | Finding |
|---|---|
| AST/ALT | Extreme elevation >2000-10,000 U/L (can mimic paracetamol overdose) |
| LDH | Also extremely elevated |
| Bilirubin | Rises later |
| PT | Prolonged |
LDH + ALP both elevated = think malignant hepatic infiltration (metastases, lymphoma). LDH rises disproportionately.
9. Wilson Disease
| Test | Finding |
|---|---|
| AST:ALT | Elevated, often AST > ALT |
| ALP | Paradoxically LOW or normal (unique!) |
| Bilirubin | Elevated (Coombs-negative haemolytic anemia) |
| Ceruloplasmin | Low |
Low ALP in a young patient with hepatitis = think Wilson disease. This is a classic exam clue.
Summary Table: LFT Patterns at a Glance
| Disease | ALT/AST | ALP/GGT | Bili | Albumin | PT | Key Clue |
|---|---|---|---|---|---|---|
| Acute viral hepatitis | ↑↑↑ (ALT≥AST) | Normal/↑ | ↑ | Normal | Normal | ALT>500 U/L |
| Alcoholic hepatitis | ↑↑ (AST≥2×ALT) | ↑ GGT | ↑ | ↓ | ↑ | AST:ALT ≥2:1, AST<300 |
| NAFLD/NASH | ↑ (ALT>AST) | ↑ mild | Normal/↑ | Normal | Normal | Metabolic risk factors |
| Cirrhosis | Normal/↑ mild (AST>ALT) | ↑ | ↑ | ↓↓ | ↑↑ | Low albumin + reversed ratio |
| Extrahepatic obstruction | Normal/↑ mild | ↑↑↑ | ↑ conj | Normal | ↑ (corrects with vit K) | Dilated ducts on US |
| PBC/PSC | ↑ mild | ↑↑↑ | ↑ conj | ↓ late | ↑ late | AMA+ (PBC), IBD (PSC) |
| Ischemic hepatitis | ↑↑↑↑ | ↑ | ↑ | ↓ | ↑↑ | LDH also extreme; rapid fall |
| Wilson disease | ↑↑ (AST>ALT) | ↓ or normal | ↑ | ↓ | ↑ | Young patient, low ceruloplasmin |
| Liver metastases | ↑ mild | ↑↑↑ | ↑ | ↓ | ↑ | LDH + ALP both ↑↑ |
Quick Interpretation Algorithm
Abnormal LFTs
|
├── ALT/AST >> ALP? → HEPATOCELLULAR
│ |
│ ├── ALT ≥ AST + >500 U/L → Viral / toxic hepatitis
│ ├── AST:ALT ≥2:1, AST <300 → Alcoholic hepatitis
│ ├── AST:ALT >1, low albumin → Cirrhosis
│ ├── Extreme >2000 U/L → Ischemic or paracetamol
│ └── AST>ALT + LOW ALP → Wilson disease
│
└── ALP/GGT >> ALT/AST? → CHOLESTATIC
|
├── PT corrects with Vit K → Extrahepatic obstruction
│ └── US → dilated ducts → stone/stricture/tumour
└── Normal ducts on imaging → Intrahepatic cholestasis
├── AMA+ → PBC
├── IBD history → PSC
└── Drug history → Drug-induced cholestasis
Generate a diagnostic flowchart poster (ALP vs AST for rapid diagnosis)
A clean medical diagnostic flowchart poster titled "LFT Rapid Diagnosis: ALP vs AST Pattern" for clinical use. The poster uses a white background with a professional medical color scheme (deep navy, crimson red, teal green, amber yellow). At the top: bold title "LFT RAPID DIAGNOSIS" with subtitle "ALP vs AST Pattern Recognition" The flowchart starts with a central box "ABNORMAL LIVER FUNCTION TESTS" in navy blue. It splits into TWO main branches with arrows: LEFT BRANCH (crimson/red): - Box: "AST > 3× URL AND ALP < 2× URL" - Label below: "HEPATOCELLULAR PATTERN" - Splits into two sub-branches: LEFT: "Normal Albumin" → green box "ACUTE HEPATITIS" with bullet points: "• Viral (ALT ≥ AST, >500 U/L)", "• Toxic/Drug-induced", "• Ischemic (>2000 U/L)" RIGHT: "Low Albumin" → orange box "CHRONIC HEPATITIS / CIRRHOSIS" with bullets: "• AST:ALT ratio >1", "• Alcoholic (AST:ALT ≥2:1)", "• NASH/NAFLD" RIGHT BRANCH (teal/green): - Box: "AST < 3× URL AND ALP > 2× URL" - Label below: "CHOLESTATIC PATTERN" - Splits into two sub-branches: LEFT: "PT corrects with Vit K" → teal box "EXTRAHEPATIC CHOLESTASIS" with bullets: "• Gallstones", "• Pancreatic cancer", "• Bile duct stricture" and note "→ Ultrasound: dilated ducts" RIGHT: "Normal ducts on imaging" → purple box "INTRAHEPATIC CHOLESTASIS" with bullets: "• PBC (AMA+)", "• PSC (IBD history)", "• Drug-induced" At the bottom: a SPECIAL CASES section in amber/yellow banner: "⚠ SPECIAL PATTERNS: Wilson Disease = LOW ALP + elevated AST in young patient | Liver Mets = LDH + ALP both markedly elevated | Shock Liver = extreme AST/ALT >2000 U/L, rapid rise and fall" Bottom footer: "De Ritis Ratio (AST:ALT): >2:1 = Alcoholic | <1 = Viral/NAFLD | >1 with low albumin = Cirrhosis" The flowchart has clean arrows, rounded rectangle boxes, clear hierarchy, bold labels, and is suitable for printing as an A3 clinical reference poster.
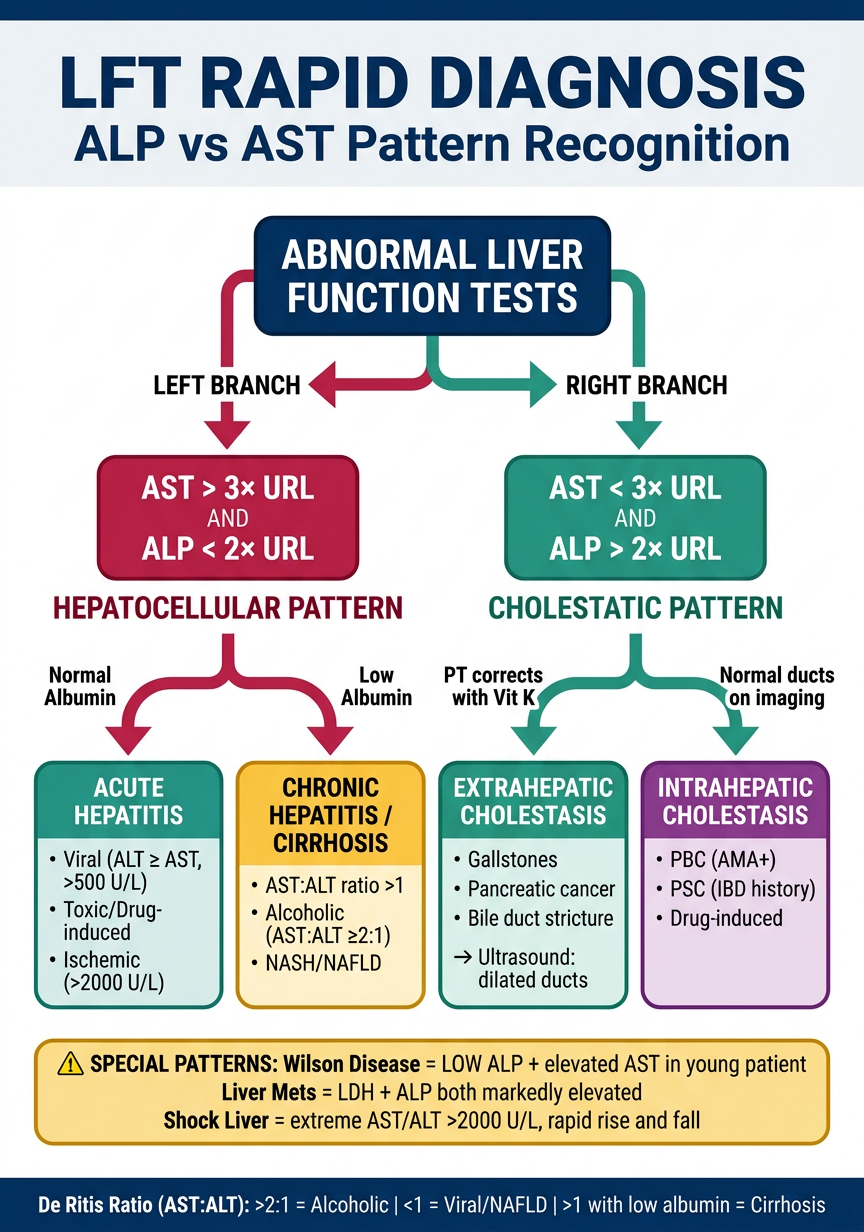
- Two core branches - Hepatocellular (AST >3× URL, ALP <2× URL) vs Cholestatic (ALP >2× URL, AST <3× URL)
- Sub-classification using albumin level (acute vs chronic hepatocellular) and PT response to Vitamin K (extra- vs intrahepatic cholestasis)
- Special patterns highlighted at the bottom - Wilson disease (paradoxically low ALP), liver metastases (LDH + ALP both elevated), and shock liver (extreme transaminases >2000 U/L)
- De Ritis ratio guide as a quick footer reference
Kidney function test (add mnemonic if possible) Identification of abnormalities
Kidney Function Tests (KFTs)
Mnemonic: "CUBAGE" - to remember all KFT components:
Letter Test C Creatinine (serum) / Creatinine clearance U Urea / BUN (Blood Urea Nitrogen) B Blood electrolytes (Na⁺, K⁺, HCO₃⁻, Cl⁻) A Albumin / Acid-base status (pH, bicarbonate) G GFR (eGFR - estimated glomerular filtration rate) E Electrolytes + Examination of urine (urinalysis, casts, protein)
Overview
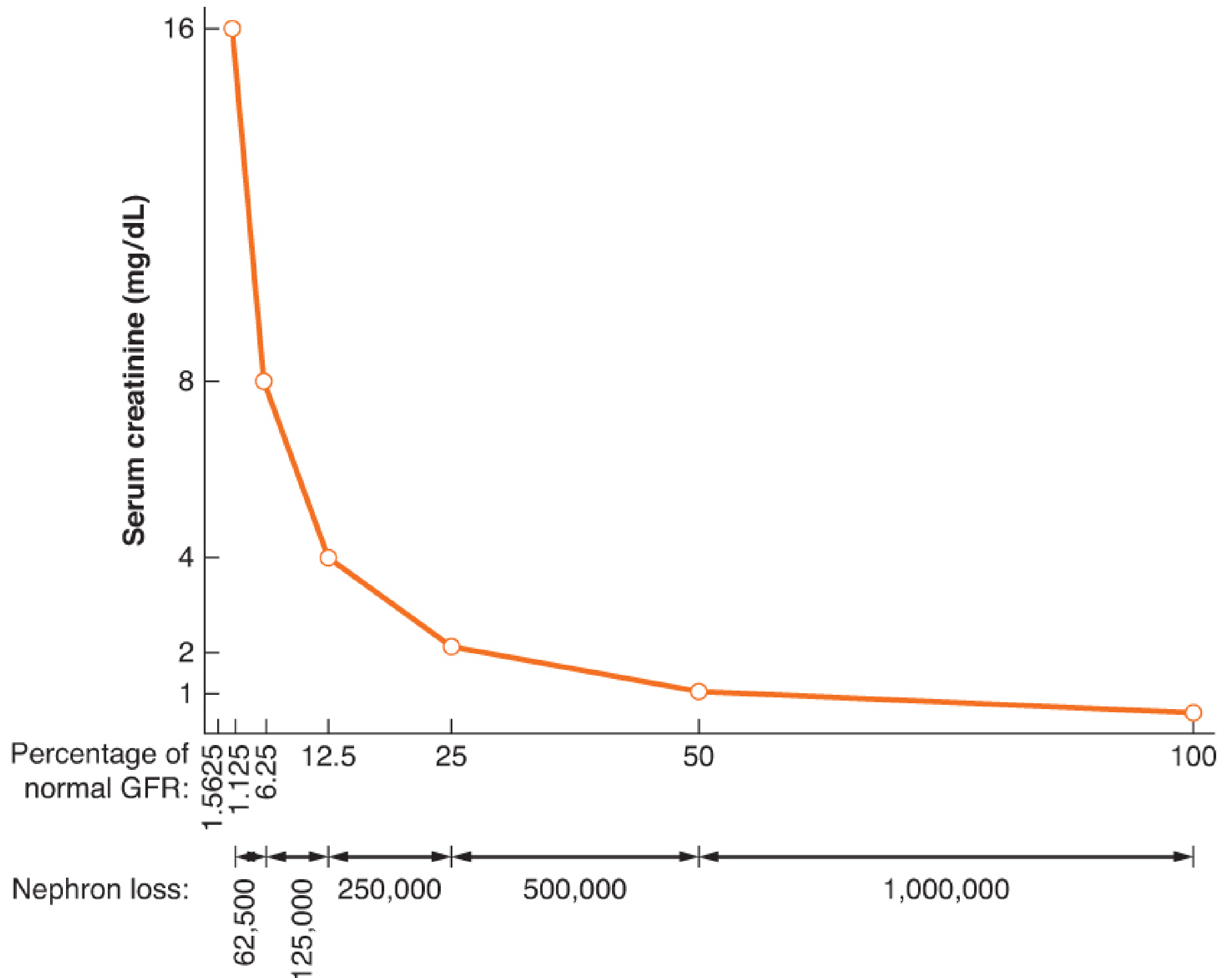
Key concept: A 75% reduction in GFR (from 120 to 30 mL/min) corresponds to only a modest rise in serum creatinine. This is why creatinine is a late marker of kidney injury.
Tests Grouped by Category
1. Glomerular Filtration Tests
Serum Creatinine
- End product of muscle creatine phosphate metabolism
- Freely filtered; minimally secreted by tubules
- Normal: Males ~0.7-1.3 mg/dL; Females ~0.5-1.1 mg/dL
- Limitations: Confounded by muscle mass, age, sex, drugs (e.g. trimethoprim blocks tubular secretion), fluid status, and laboratory technique
- Not renal-specific alone - must interpret with clinical context
eGFR (Estimated GFR)
- Calculated using CKD-EPI or MDRD equations from serum creatinine, age, sex, race
- The single best overall marker of kidney function in clinical practice
- Normal: 100-120 mL/min/1.73 m²
| GFR Stage | eGFR (mL/min) | Interpretation |
|---|---|---|
| Normal | >90 | With markers of kidney damage |
| Mildly reduced | 60-89 | |
| Mildly-moderately reduced | 45-59 | CKD G3a |
| Moderately-severely reduced | 30-44 | CKD G3b |
| Severely reduced | 15-29 | CKD G4 |
| Kidney failure | <15 | ESRD - consider dialysis |
Creatinine Clearance (CrCl)
- 24-hour urine collection method
- Formula: CrCl = (U × V) / P where U = urine creatinine, V = urine volume (mL/min), P = plasma creatinine
- Slightly overestimates GFR (due to tubular secretion of creatinine)
- Normal: 100-120 mL/min
2. BUN / Blood Urea Nitrogen
- Urea is the main end product of protein catabolism (urea cycle in liver)
- Normal: 5-20 mg/dL (1.8-7.2 mmol/L)
- Not purely renal - confounded by:
- Protein intake (high protein diet raises BUN)
- Liver disease (impaired synthesis lowers BUN)
- GI bleed, catabolic states, dehydration (raise BUN disproportionately)
BUN:Creatinine Ratio - Clinically Vital
| Ratio | Interpretation |
|---|---|
| >20:1 | Prerenal azotemia (dehydration, GI bleed, heart failure) |
| 10-20:1 | Normal / Intrinsic renal disease |
| <10:1 | Low protein intake, liver failure, SIADH |
Mnemonic: "Twenty-to-One = Pre-Renal Run" - BUN:Cr >20 = prerenal
3. Electrolytes
| Electrolyte | Normal | Significance in Renal Disease |
|---|---|---|
| Sodium (Na⁺) | 135-145 mEq/L | Hyponatremia in SIADH, dilutional states; altered in CKD |
| Potassium (K⁺) | 3.5-5.0 mEq/L | Hyperkalemia is a cardinal feature of AKI/CKD - life-threatening |
| Bicarbonate (HCO₃⁻) | 22-26 mEq/L | Low in metabolic acidosis from CKD (failure to excrete H⁺) |
| Chloride (Cl⁻) | 98-106 mEq/L | Raised in hyperchloremic metabolic acidosis |
| Phosphate | 2.5-4.5 mg/dL | Elevated in CKD (kidneys fail to excrete phosphate) |
| Calcium | 8.5-10.5 mg/dL | Low in CKD (reduced vitamin D activation) |
| Uric Acid | 2.4-7.0 mg/dL (M) | Elevated in gout, CKD; low in Fanconi syndrome |
4. Urinalysis (Urine Examination)
Dipstick Analysis
| Parameter | Normal | Abnormal Finding | Significance |
|---|---|---|---|
| Protein | Negative (<150 mg/day) | Positive | Glomerular damage, nephrotic syndrome |
| Blood/Hematuria | Negative | Positive | GN, stones, UTI, malignancy |
| Glucose | Negative | Positive with normal blood sugar | Tubular dysfunction (Fanconi syndrome) |
| Nitrites | Negative | Positive | Bacterial UTI |
| Leukocyte esterase | Negative | Positive | Pyuria, UTI, AIN |
| pH | 4.5-8.0 | Alkaline in RTA | Renal tubular acidosis |
| Specific Gravity | 1.001-1.035 | Fixed at 1.010 | Isosthenuria = tubular damage (AKI) |
| Ketones | Negative | Positive | DKA, starvation |
Urine Microscopy - Casts and What They Mean
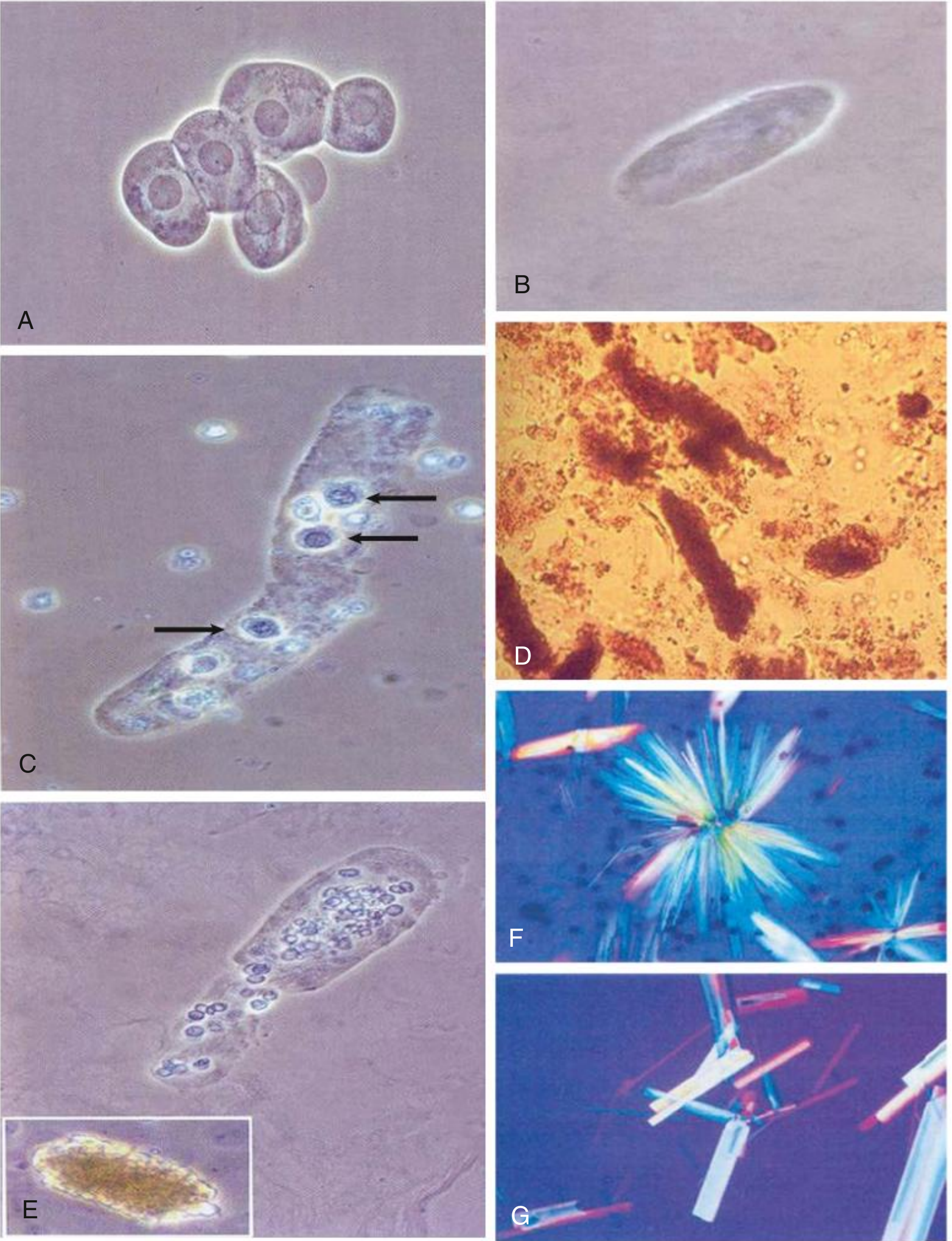
Mnemonic for casts: "Hyaline = Fine; RBC = Glomerulonephritis; WBC = interstitial; Muddy Brown = ATN; Broad Waxy = CKD"
| Cast Type | Diagnosis |
|---|---|
| Hyaline casts | Normal or prerenal AKI (dehydration, mild) |
| RBC (red cell) casts | Glomerulonephritis, vasculitis (GOLD STANDARD finding) |
| WBC (white cell) casts | Acute interstitial nephritis (AIN), pyelonephritis |
| Granular "muddy brown" casts | Acute tubular necrosis (ATN) - >10/LPF = 100% PPV for ATN |
| Fatty casts / oval fat bodies | Nephrotic syndrome (heavy proteinuria) |
| Broad / waxy casts | Chronic kidney disease (dilated tubules) |
| Epithelial cell casts | Early ATN |
5. Proteinuria Quantification
| Amount | Category | Significance |
|---|---|---|
| <150 mg/day | Normal | |
| 150-3500 mg/day | Non-nephrotic | CKD, hypertensive nephropathy |
| >3.5 g/day | Nephrotic range | Minimal change, FSGS, membranous nephropathy, diabetic nephropathy |
- Glomerular - filtered proteins (albumin predominant; failure of filtration barrier)
- Overflow - excess production saturates reabsorption (Bence-Jones proteins in myeloma)
- Tubular - failed reabsorption of normally filtered small proteins
- Secretory/tissue - inflammation (Tamm-Horsfall protein)
6. Fractional Excretion of Sodium (FENa)
| FENa | Interpretation |
|---|---|
| <1% | Prerenal AKI (tubules intact, avidly reabsorbing Na) |
| >3% | ATN (tubular damage, can't reabsorb Na) |
| 1-3% | Indeterminate |
Caveat: FENa <1% can occur in ATN with contrast, myoglobin, sepsis, or heart failure. If patient is on diuretics, use FEUrea <35% = prerenal instead.
Identifying Abnormalities: Disease Patterns
AKI vs CKD - First Differentiation
| Feature | AKI | CKD |
|---|---|---|
| Onset | Sudden (hours-days) | Gradual (months-years) |
| Urine output | Often oliguria | Normal initially |
| Kidney size on US | Normal or enlarged | Small, echogenic |
| Anaemia | Absent early | Present (low EPO) |
| Broad waxy casts | Absent | Present |
| Calcium/Phosphate | Usually normal initially | Hyperphosphatemia, hypocalcemia |
| Prior creatinine | Normal | Chronically elevated |
KDIGO Classification of AKI
| Stage | Serum Creatinine Criteria | Urine Output |
|---|---|---|
| 1 | Rise ≥0.3 mg/dL within 48h OR 1.5-1.9× baseline | <0.5 mL/kg/h for 6-12h |
| 2 | 2.0-2.9× baseline | <0.5 mL/kg/h for ≥12h |
| 3 | ≥3× baseline OR ≥4.0 mg/dL OR dialysis | <0.3 mL/kg/h for ≥24h or anuria ≥12h |
Distinguishing Prerenal, Intrinsic, and Postrenal AKI
| Parameter | Prerenal | Intrinsic (ATN) | Postrenal |
|---|---|---|---|
| BUN:Cr ratio | >20:1 | 10-15:1 | Variable |
| FENa | <1% | >3% | Variable |
| Urine Na | <20 mEq/L | >40 mEq/L | Variable |
| Urine osmolality | >500 mOsm/kg | ~300 (isosthenuria) | Variable |
| Urine specific gravity | >1.020 | ~1.010 | Variable |
| Urine casts | Hyaline (or none) | Muddy brown granular | None |
| Response to fluids | Improves | No improvement | Improves with relief |
Mnemonic: "Prerenal LOVES sodium - holds it tight (FENa <1%, UNa <20)" "ATN LOSES sodium - can't hold it (FENa >3%, UNa >40)"
Nephrotic vs Nephritic Syndrome
| Feature | Nephrotic | Nephritic |
|---|---|---|
| Proteinuria | >3.5 g/day | <3.5 g/day |
| Haematuria | Absent/mild | Present (RBC casts) |
| Hypertension | Mild/absent | Prominent |
| Oedema | Severe (anasarca) | Mild-moderate |
| GFR | Near normal early | Reduced |
| Serum albumin | Low | Normal/mildly low |
| Serum cholesterol | High | Normal |
| Urine casts | Fatty, oval fat bodies | RBC casts |
Mnemonic - Nephrotic = "PALE": Protein (massive), Albumin (low), Lipids (high), Edema (severe) Mnemonic - Nephritic = "PHARH": Protein (mild), Haematuria, Azotemia, RBC casts, Hypertension
Reference Ranges Summary
| Test | Normal Value |
|---|---|
| Serum Creatinine (M/F) | 0.7-1.3 / 0.5-1.1 mg/dL |
| BUN | 5-20 mg/dL |
| BUN:Creatinine ratio | 10-20:1 |
| eGFR | >90 mL/min/1.73m² (normal) |
| Creatinine Clearance | 100-120 mL/min |
| Urine Protein | <150 mg/day |
| Urine specific gravity | 1.001-1.035 |
| Serum K⁺ | 3.5-5.0 mEq/L |
| Serum Na⁺ | 135-145 mEq/L |
| Serum HCO₃⁻ | 22-26 mEq/L |
| FENa (prerenal) | <1% |
| FENa (ATN) | >3% |