Bsc nursing cancer total topics
Reading File
Finding Sources
Searching the Web
BSc Nursing oncology cancer syllabus topics India 2024
Finding Sources
Reading Web Page
https://indiannursingcouncil.org/uploads/pdf/161483504517442…
Finding Sources
Searching the Web
BSc Nursing 3rd year medical surgical nursing cancer chapter topics India INC syllabus
Reading Web Page
https://www.moscmm.org/uploads/userfiles/Sylabus%203%20rd%20…
Finding Sources
Here is a complete, structured breakdown of all cancer/oncology topics covered in the BSc Nursing curriculum (as per Indian Nursing Council guidelines, primarily under Medical-Surgical Nursing II in 3rd Year):
BSc Nursing - Cancer / Oncology: Complete Topic List
UNIT 1: Introduction & Epidemiology of Cancer
- Definition of cancer
- Prevalence and incidence statistics (national and global)
- Risk factors - chemical, physical, biological, lifestyle, genetic
- Causes and contributing factors
- Cancer prevention strategies
- Health promotion and early detection
- Screening programs (PAP smear, mammography, BSE, FNAC)
- Warning signs of cancer (CAUTION signs)
UNIT 2: Biology & Pathophysiology of Cancer
- Cell cycle - phases (G1, S, G2, M)
- Characteristics of normal cells vs. cancer cells
- Carcinogenesis - initiation, promotion, progression stages
- Definitions: dysplasia, metaplasia, anaplasia, neoplasia
- Benign vs. malignant tumor characteristics
- Genomics and genetics of cancer - oncogenes, tumor suppressor genes
- Metastasis - modes and mechanisms (direct spread, lymphatic, hematogenous, transcoelomic)
- Molecular biology of cancer
- Tumor microenvironment
UNIT 3: Classification, Staging & Grading
- Classification of tumors - by tissue of origin (carcinoma, sarcoma, lymphoma, leukemia, mixed)
- Staging - TNM staging system (Tumor, Node, Metastasis)
- Grading - Grade I to IV (degree of differentiation)
- Cancer staging I to IV
- Nurses' responsibilities in staging and grading
UNIT 4: Diagnostic Tests & Investigations
- Tumor markers and biomarkers (CEA, PSA, AFP, CA-125, CA-19.9, etc.)
- Cytology tests (PAP smear, FNAC)
- Biopsy - excisional, incisional, needle
- Bone marrow aspiration and trephine biopsy
- Endoscopy and laparoscopy
- Histopathology and immunohistochemistry
- Imaging: CT scan, MRI, PET scan, ultrasound
- Radionuclide imaging and use of radioisotopes
- Functional and metabolic imaging
- Mammography
- Nurses' responsibilities during diagnostic procedures
UNIT 5: Treatment Modalities
A. Surgery
- Types of cancer surgery - curative, palliative, prophylactic, reconstructive
- Pre- and post-operative nursing management
- Principles of surgical oncology
B. Chemotherapy
- Classification of chemotherapeutic agents:
- Alkylating agents
- Antimetabolites
- Plant alkaloids (vinca alkaloids, taxanes)
- Antitumor antibiotics
- Topoisomerase inhibitors
- Targeted therapy agents
- Mechanism of action
- Routes of administration - oral, IV, intrathecal, intravesical
- Side effects and toxicities: myelosuppression, mucositis, alopecia, nausea, peripheral neuropathy
- Nursing management during chemotherapy
- Safe handling of cytotoxic drugs
- Central Venous Access Devices (CVADs) - PICC line, Hickman catheter, Chemo port, central lines
- Extravasation management
C. Radiotherapy
- Types: external beam, brachytherapy, stereotactic
- Mechanism of action (ionizing radiation, DNA damage)
- Side effects: skin reactions, fatigue, radiation mucositis, bone marrow suppression
- Nursing care during radiotherapy
- Radiation safety and protection (ALARA principle)
D. Immunotherapy
- Concept of immune surveillance
- Types: monoclonal antibodies, checkpoint inhibitors, cytokines (IL-2, interferon)
- CAR-T cell therapy
- Side effects and nursing management
E. Hormone Therapy
- Hormone-responsive cancers (breast, prostate, endometrial)
- Drugs: Tamoxifen, Aromatase inhibitors, LHRH agonists
- Nursing responsibilities
F. Targeted Therapy
- Tyrosine kinase inhibitors (Imatinib, Erlotinib)
- HER2-targeted therapy (Trastuzumab)
- VEGF inhibitors (Bevacizumab)
G. Gene Therapy
- Concept and current status
- Types: gene replacement, gene silencing, oncolytic viruses
H. Stem Cell & Bone Marrow Transplantation (BMT)
- Types: autologous, allogeneic, syngeneic
- Hematopoietic stem cell collection and preservation
- Nursing care of transplant recipient
- Engraftment syndrome management
- Graft-vs-host disease (GVHD)
- Preparation for discharge and home care
I. Other/Alternative Therapies
- Complementary therapies (yoga, meditation, acupuncture)
- Herbal and nutritional therapies
UNIT 6: Common Malignancies (System-wise)
| System | Cancers Covered |
|---|---|
| Head & Neck | Oral cancer, Laryngeal cancer |
| Respiratory | Lung cancer |
| GI Tract | Stomach cancer, Colorectal cancer, Liver cancer |
| Hematological | Leukemias (ALL, AML, CLL, CML), Lymphomas (Hodgkin's, Non-Hodgkin's), Multiple myeloma |
| Female Reproductive | Breast cancer, Cervical cancer, Ovarian cancer, Uterine/Endometrial cancer |
| Male Reproductive | Prostate cancer, Testicular cancer |
| Urinary | Renal cell carcinoma, Bladder cancer |
| Neurological | Brain tumors (Gliomas, Meningiomas) |
| Musculoskeletal | Osteosarcoma, Ewing's sarcoma |
| Skin | Melanoma, Basal cell carcinoma, Squamous cell carcinoma |
| Pediatric | Wilms' tumor, Neuroblastoma, Retinoblastoma, ALL in children |
For each cancer, the following are covered:
- Epidemiology and etiology
- Pathophysiology
- Classification / staging
- Clinical manifestations (signs and symptoms)
- Diagnostic investigations
- Medical and surgical management
- Nursing assessment and nursing diagnoses
- Nursing care plan (pre-op, intra-op, post-op)
- Patient and family education
- Prognosis
UNIT 7: Nursing Assessment of Cancer Patients
- Comprehensive history taking
- Physical examination (head-to-toe)
- Psychological, social, cultural and spiritual assessment
- Symptom assessment: pain, fatigue, nutritional status
- Nursing diagnosis formulation
- Assessment in pediatric and adult patients
UNIT 8: Oncological Emergencies
- Superior Vena Cava Syndrome (SVCS)
- Spinal cord compression
- Cardiac tamponade
- Hypercalcemia of malignancy
- Tumor lysis syndrome (TLS)
- Disseminated Intravascular Coagulation (DIC)
- Septic shock in neutropenic patients (Febrile neutropenia)
- Syndrome of Inappropriate ADH secretion (SIADH)
- Pathologic fractures
UNIT 9: Infection Control in Oncology
- Immunity in cancer patients (immunosuppression)
- Principles of asepsis, sterilization and disinfection
- Standard precautions and barrier nursing
- Protective/reverse isolation
- Biomedical waste management
- Fumigation
- Safe handling of cytotoxic waste
- Standard Operating Procedures (SOPs) for infection control and chemotherapy
UNIT 10: Psychosocial, Cultural & Spiritual Aspects
- Human behavior and coping with cancer
- Stages of grief (Kubler-Ross model) applied to cancer
- Factors influencing psychosocial adjustment
- Sociocultural attitudes toward cancer
- Anxiety, depression, and body image disturbances
- Guidance and counselling techniques
- Spiritual and cultural care
- Communication with cancer patients and families
- Breaking bad news
UNIT 11: Palliative Care & Pain Management
- Concept and philosophy of palliative care
- WHO analgesic ladder for cancer pain
- Pharmacological management: NSAIDs, Opioids, adjuvants
- Non-pharmacological pain management
- Symptom management - dyspnea, nausea, constipation, anorexia, fatigue
- Hospice care - concept and principles
- Care of the dying patient
- Care of the dead body
- Bereavement counselling for families
UNIT 12: Rehabilitation, Nutritional Support & Home Care
- Principles of cancer rehabilitation
- Physical rehabilitation (mastectomy, laryngectomy, ostomy care)
- Nutritional assessment and support - enteral and parenteral nutrition
- Dietary management in cancer
- Home care of cancer patients
- Discharge planning
- Community resources and cancer support groups
UNIT 13: Procedures & Equipment in Oncology (Clinical Skills)
- Bone marrow aspiration and biopsy (assist)
- Hematopoietic stem cell collection and preservation
- Insertion and care of CVADs (PICC, Hickman, Chemo port, central lines)
- Apheresis machine
- Platelet agitator
- Bio-safety cabinet
- Thawing machine
- Cryopreservation
- Blood component refrigerator
- Conducting unit audits
UNIT 14: Quality Control & SOP Preparation
- Preparation of SOP for infection control in oncology
- Preparation of SOP for chemotherapy administration
- Conducting unit audit
UNIT 15: Professionalism & Evidence-Based Practice in Oncology Nursing
- Scope of oncology nursing practice
- Roles and responsibilities of cancer nurses in different settings (OPD, inpatient, ICU, palliative, home)
- Evidence-based practice in oncology
- Research in oncology nursing
- Patient education and counselling methods
- Clinical leadership and resource management
Quick Reference: Key Cancer Nursing Skills (Practical)
- Comprehensive assessment of adult and pediatric cancer patients
- Writing nursing care plans for cancer patients
- Counselling patients and families
- Screening for common cancers (PAP smear, BSE, FNAC assist)
- Assisting in biopsies and bone marrow aspiration
- Chemotherapy administration (safety, extravasation management)
- Radiation safety practices
- Pain assessment tools (VAS, NRS, FACES scale)
- Stoma care (colostomy, urostomy)
- Central line care and CVAD maintenance
- Palliative care and EOL nursing
- Breast self-examination (BSE) demonstration and teaching
This covers the complete cancer/oncology topic list as per the Indian Nursing Council (INC) BSc Nursing syllabus, primarily in 3rd Year Medical-Surgical Nursing II (100 theory hours) along with related clinical postings (400 practical hours). Topics may also appear in related chapters of Child Health Nursing (pediatric cancers), Pharmacology, and Pathology.
Comman pathology physiology of eye
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Loading Image
Here is a complete, well-structured breakdown of the common pathology and physiology of the eye as covered in nursing and medical curricula:
Common Pathology & Physiology of the Eye
PART A: PHYSIOLOGY OF THE EYE
1. Structure & Function Overview
The eye is the organ of vision. Key functional structures:
| Structure | Function |
|---|---|
| Cornea | Transparent outer covering; refracts light (~70% of total refraction) |
| Lens | Fine-focuses light onto retina (accommodation); ~30% of refraction |
| Aqueous humor | Nourishes cornea and lens; maintains intraocular pressure (IOP) |
| Vitreous humor | Fills posterior segment; maintains eye shape |
| Retina | Contains photoreceptors (rods and cones); converts light to nerve signals |
| Optic nerve | Transmits visual signals to the brain |
| Iris | Controls pupil size; regulates light entry |
| Ciliary body | Produces aqueous humor; controls lens shape for accommodation |
| Macula/fovea | Area of highest visual acuity (color vision via cones) |
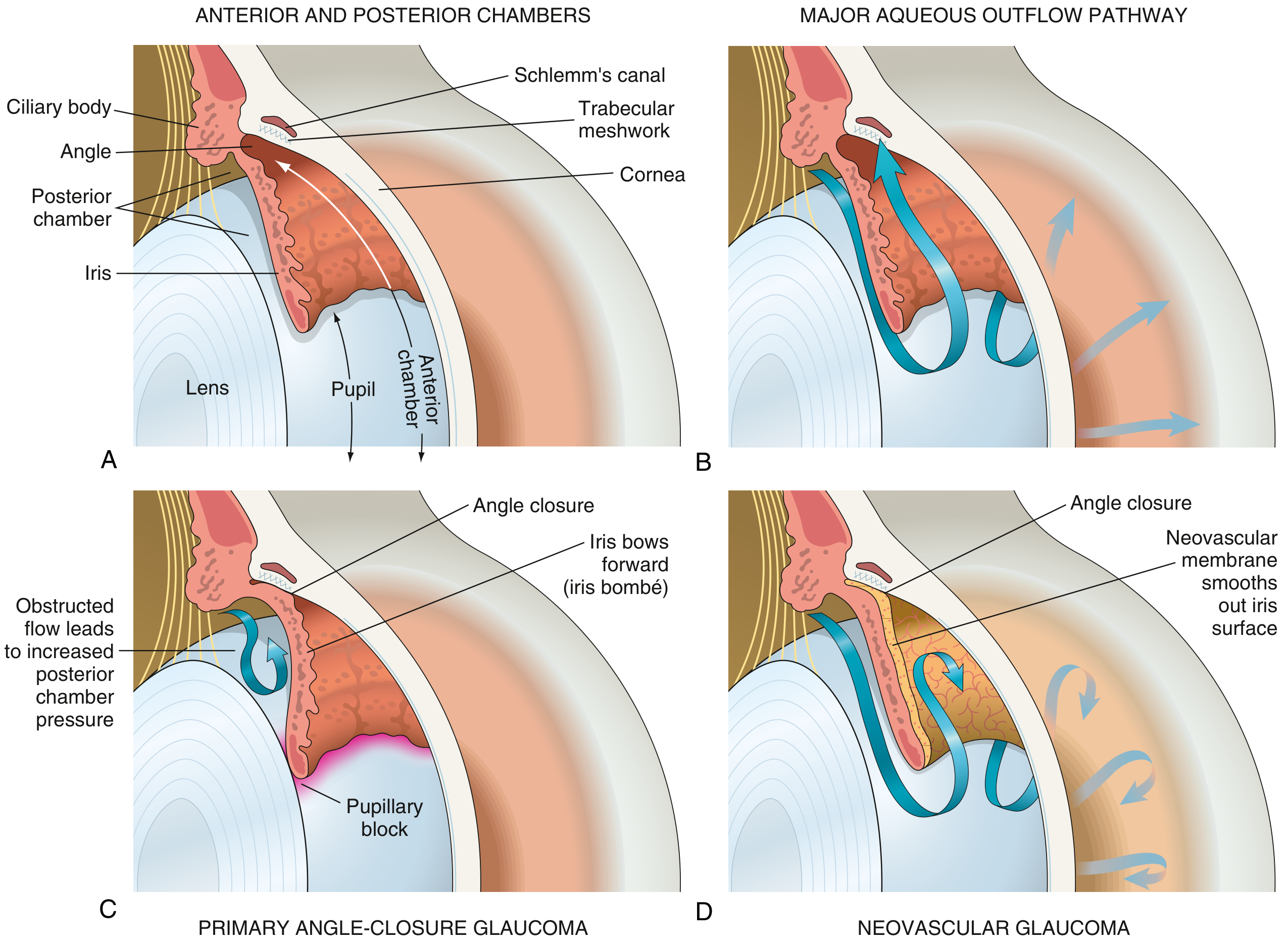
2. Aqueous Humor Dynamics (Critical for Glaucoma)
- Produced by the pars plicata of the ciliary body in the posterior chamber
- Flows through the pupil into the anterior chamber
- Drains primarily through the trabecular meshwork into Schlemm's canal
- Normal IOP: 10-21 mmHg
- If drainage is impaired → IOP rises → optic nerve damage
3. Visual Pathway (Physiology of Sight)
- Light enters cornea → refracted
- Passes through aqueous humor → pupil → lens (fine focus) → vitreous → retina
- Photoreceptors - rods (dim light/peripheral vision) and cones (color/central vision) convert light to electrical signals
- Signals travel via optic nerve → optic chiasm → optic tract → lateral geniculate nucleus → visual cortex (occipital lobe)
4. Accommodation Reflex
- Near vision: ciliary muscle contracts → suspensory ligaments relax → lens becomes more convex (more powerful)
- Far vision: ciliary muscle relaxes → lens flattens
5. Pupillary Light Reflex
- Light hits retina → optic nerve (afferent) → Edinger-Westphal nucleus → oculomotor nerve (efferent) → pupil constriction (miosis)
- Tests integrity of CN II (afferent) and CN III (efferent)
PART B: COMMON EYE PATHOLOGIES
1. CATARACT
Definition: Opacity (clouding) of the lens that impairs vision.
Types:
- Nuclear (most common): Aging-related opacification of the lens nucleus (nuclear sclerosis)
- Cortical: Spoke-like opacities from the periphery inward
- Posterior subcapsular: Near the back of the lens; common with steroid use
Causes / Risk Factors:
- Aging (most common)
- Diabetes mellitus
- Corticosteroid use (long-term)
- Radiation / UV exposure
- Trauma
- Congenital (galactosemia, rubella)
- Wilson disease, atopic dermatitis
Pathophysiology:
- Normal lens epithelium does NOT shed dead cells - cells accumulate in the lens center with aging
- Protein aggregation and oxidation make lens fibers opaque
- Liquefaction of lens cortex and urochrome pigment accumulation also contribute
Clinical Features:
- Gradual, painless loss of vision
- Glare/halos around lights
- Faded or yellowed colors
- Frequent change in glasses prescription
- "Second sight" (temporary improvement in near vision in early nuclear cataract)
Treatment:
- Surgery: Phacoemulsification + intraocular lens (IOL) implantation (most common)
- The lens capsule is left intact; prosthetic IOL inserted
(Robbins Basic Pathology, p. 868)
2. GLAUCOMA
Definition: A group of diseases causing optic neuropathy, usually associated with elevated IOP. Results in irreversible vision loss.
Normal IOP: 10-21 mmHg. Glaucoma typically >21 mmHg (but normal-tension glaucoma also exists).
Classification:
| Type | Mechanism |
|---|---|
| Primary Open-Angle (POAG) | Most common type. Trabecular meshwork resistance increases; angle remains open. Gradual, painless |
| Primary Angle-Closure (PACG) | Iris occludes trabecular meshwork; common in hyperopia (shallow anterior chamber). Can be acute (emergency) |
| Secondary Open-Angle | Particulate debris (RBCs post-trauma, necrotic tumor) blocks meshwork |
| Neovascular | VEGF-driven neovascular membrane covers iris and closes angle; occurs in diabetic retinopathy, retinal vein occlusion |
| Congenital | Developmental anomaly of drainage angle (trabeculodysgenesis) |
Pathophysiology:
- Aqueous humor cannot drain → IOP rises → pressure damages optic nerve head
- Ganglion cells and retinal nerve fiber layer are lost
- Results in progressive peripheral visual field loss → tunnel vision → blindness
Clinical Features:
- POAG: Insidious, asymptomatic until late. Peripheral field loss first
- Acute angle-closure: Sudden severe eye pain, headache, nausea/vomiting, colored halos, red eye, mid-dilated fixed pupil - EMERGENCY
Investigations:
- Tonometry (IOP measurement)
- Gonioscopy (angle assessment)
- Visual field testing (perimetry)
- Optic disc assessment (cup-to-disc ratio >0.6 suspicious)
- OCT (retinal nerve fiber layer thickness)
Treatment:
- Eye drops: Beta-blockers (Timolol), Prostaglandin analogues (Latanoprost), Alpha-2 agonists (Brimonidine), Carbonic anhydrase inhibitors (Dorzolamide)
- Laser: Laser trabeculoplasty (open-angle), Laser iridotomy (angle-closure)
- Surgery: Trabeculectomy, glaucoma drainage devices
(Robbins Basic Pathology, p. 869-870)
3. DIABETIC RETINOPATHY
Most common cause of blindness in working-age adults (20-60 years).
Pathophysiology:
- Chronic hyperglycemia → basement membrane thickening of retinal capillaries → pericyte loss → microaneurysms → increased vascular permeability → retinal ischemia → VEGF upregulation → neovascularization
Stages / Classification:
| Stage | Features |
|---|---|
| Non-Proliferative DR (NPDR) - Mild | Microaneurysms only |
| NPDR - Moderate | Microaneurysms, dot-blot hemorrhages, hard exudates |
| NPDR - Severe | Venous beading, IRMA (intraretinal microvascular abnormalities), >20 hemorrhages in 4 quadrants |
| Proliferative DR (PDR) | New blood vessel formation (neovascularization) on disc/retina; risk of vitreous hemorrhage and tractional retinal detachment |
| Diabetic Macular Edema (DME) | Can occur at any stage; major cause of visual impairment |
Clinical Features:
- Gradual blurring of vision
- Floaters (vitreous hemorrhage)
- Sudden vision loss (retinal detachment or vitreous hemorrhage)
Treatment:
- Tight glycemic and BP control (prevention)
- Laser photocoagulation (NPDR and PDR)
- Anti-VEGF injections (Ranibizumab, Bevacizumab) for DME and PDR
- Vitrectomy for vitreous hemorrhage / traction detachment
4. RETINAL DETACHMENT
Definition: Separation of the neurosensory retina from the retinal pigment epithelium (RPE).
Types:
| Type | Mechanism |
|---|---|
| Rhegmatogenous | Tear/hole in retina allows fluid to enter; most common |
| Tractional | Fibrovascular bands pull retina away (e.g., PDR, sickle cell) |
| Exudative | Fluid from inflamed/tumorous vessels accumulates (no tear) |
Risk Factors: High myopia, previous trauma, cataract surgery, family history, diabetic retinopathy
Clinical Features:
- Flashes of light (photopsia)
- Floaters (sudden increase)
- "Curtain coming down" / shadow in visual field
- Painless loss of vision
- Macular detachment = central vision loss
Treatment: Surgical urgency - Laser retinopexy, cryotherapy, scleral buckle, pneumatic retinopexy, vitrectomy
5. CONJUNCTIVITIS ("Pink Eye")
Definition: Inflammation of the conjunctiva.
Types & Causes:
| Type | Cause | Key Features |
|---|---|---|
| Bacterial | S. pneumoniae, H. influenzae, S. aureus, Pseudomonas | Purulent discharge, crusting, no lymphadenopathy |
| Viral | Adenovirus (most common), Herpes, Enterovirus | Watery discharge, preauricular lymphadenopathy, highly contagious |
| Allergic | Allergens (pollen, dust mites) | Itching (hallmark), bilateral, clear watery discharge, seasonal |
| Chlamydial (Trachoma) | Chlamydia trachomatis | Leading cause of preventable blindness worldwide; follicular conjunctivitis, pannus formation |
| Neonatal (Ophthalmia neonatorum) | N. gonorrhoeae (hyperacute), C. trachomatis | Severe in gonorrheal - can perforate cornea |
| Chemical/Toxic | Drugs, chlorine, UV | Acute, exposure history |
Clinical Features common to all:
- Red eye (conjunctival injection)
- Discharge (purulent/watery/mucoid)
- Foreign body sensation, gritty feeling
- Photophobia
- Blurred vision (usually mild)
Treatment:
- Bacterial: Topical antibiotics (ciprofloxacin, chloramphenicol eye drops)
- Viral: Self-limiting; lubricants, cold compresses
- Allergic: Topical antihistamines, mast cell stabilizers, avoid allergens
- Trachoma: Azithromycin (SAFE strategy - Surgery, Antibiotics, Facial cleanliness, Environmental improvement)
6. UVEITIS
Definition: Inflammation of the uveal tract (iris, ciliary body, choroid).
Classification:
- Anterior uveitis (iritis/iridocyclitis) - most common
- Intermediate uveitis (pars planitis)
- Posterior uveitis (choroiditis, retinitis)
- Panuveitis (all layers)
Causes:
- Autoimmune: Juvenile idiopathic arthritis (JIA), ankylosing spondylitis, sarcoidosis
- Infectious: Toxoplasmosis (most common cause of posterior uveitis), CMV (in AIDS), TB, HSV
- Sympathetic ophthalmia - bilateral granulomatous uveitis after penetrating eye injury (trauma to one eye triggers immune reaction in both)
Clinical Features (Anterior):
- Deep aching eye pain
- Photophobia (characteristic)
- Lacrimation (watery eye)
- Ciliary flush (redness around cornea)
- Keratic precipitates (KPs) on corneal endothelium
- Hypopyon (pus in anterior chamber)
- Posterior synechiae (adhesion of iris to lens)
Treatment: Topical/systemic steroids, cycloplegics (atropine to prevent synechiae), treat underlying cause
(Robbins Basic Pathology)
7. REFRACTIVE ERRORS
| Condition | Defect | Correction |
|---|---|---|
| Myopia (near-sightedness) | Eyeball too long / cornea too curved; image focuses in front of retina | Concave (diverging) lens |
| Hyperopia (far-sightedness) | Eyeball too short; image focuses behind retina | Convex (converging) lens |
| Astigmatism | Irregular curvature of cornea/lens; multiple focal points | Cylindrical lens |
| Presbyopia | Age-related loss of accommodation (lens stiffening, ciliary muscle weakness); difficulty reading | Reading glasses (convex) |
8. AGE-RELATED MACULAR DEGENERATION (AMD)
Leading cause of irreversible central vision loss in adults >50 years.
Types:
- Dry AMD (Atrophic): 85-90% of cases. Drusen deposits under macula → gradual geographic atrophy of RPE. Slow central vision loss.
- Wet AMD (Neovascular/Exudative): 10-15% of cases but causes 90% of severe vision loss. Choroidal neovascularization → fluid/blood under retina. Rapid loss.
Symptoms:
- Blurred central vision
- Metamorphopsia (straight lines appear wavy - Amsler grid test)
- Central scotoma (blank spot)
- Colors appear washed out
- Peripheral vision preserved
Treatment:
- Dry: No cure; AREDS2 vitamins (antioxidants) slow progression
- Wet: Anti-VEGF injections (Ranibizumab, Aflibercept, Bevacizumab) - intravitreal; first-line
9. CORNEAL PATHOLOGY
| Condition | Key Features |
|---|---|
| Keratitis | Corneal inflammation; bacterial (S. aureus, Pseudomonas), viral (HSV - dendritic ulcer), fungal, acanthamoeba (contact lens users). Severe pain, photophobia, reduced vision |
| Corneal Ulcer | Loss of corneal epithelium with underlying stromal involvement; emergency |
| Keratoconus | Progressive thinning and cone-shaped deformity of cornea; irregular astigmatism; managed with rigid contact lenses or corneal transplant |
| Pterygium | Triangular growth of fibrovascular tissue from conjunctiva onto cornea; linked to UV exposure |
10. STRABISMUS (SQUINT)
Definition: Misalignment of the eyes; failure of binocular vision.
Types:
- Esotropia (convergent - eye turns inward)
- Exotropia (divergent - eye turns outward)
- Hypertropia/hypotropia (vertical deviation)
Complication: Amblyopia ("lazy eye") - suppression of visual input from misaligned eye leads to irreversible poor vision if untreated in childhood
Treatment: Patching (amblyopia), glasses, orthoptic exercises, surgery
11. RETINOBLASTOMA (Pediatric)
Most common intraocular malignancy in children. Mutation of RB1 gene (chromosome 13q14) - classic example of tumor suppressor gene loss.
Clinical Features:
- Leukocoria (white pupillary reflex/"cat's eye") - most common presenting sign
- Strabismus
- Painful red eye (advanced disease)
Treatment: Chemotherapy, laser, cryotherapy, enucleation for advanced cases
PART C: QUICK SUMMARY TABLE
| Disease | Key Mechanism | Vision Loss Pattern | Key Sign |
|---|---|---|---|
| Cataract | Lens protein aggregation | Gradual, painless blurring | Absent red reflex |
| POAG | Trabecular outflow resistance | Peripheral → central | Increased cup:disc ratio |
| Acute Angle-Closure | Pupillary block → angle occlusion | Sudden, severe | Mid-dilated fixed pupil, hard eye |
| Diabetic Retinopathy | Microangiopathy + VEGF | Variable | Microaneurysms, neovascularization |
| AMD | Drusen/RPE atrophy or CNV | Central vision only | Drusen on fundus, Amsler grid distortion |
| Retinal Detachment | Separation of neuroretina | "Curtain" shadow | Billowing retina on fundoscopy |
| Conjunctivitis | Infection/allergy of conjunctiva | Mild blurring | Red eye, discharge |
| Uveitis | Intraocular inflammation | Variable | Photophobia, KPs, hypopyon |
| Myopia | Elongated axial length | Distant objects blurred | Corrected with concave lens |
Sources: Robbins Basic Pathology (p. 868-870), Kanski's Clinical Ophthalmology 10th Ed., Ganong's Review of Medical Physiology 26th Ed., Goldman-Cecil Medicine.
This is a shared conversation. Sign in to Orris to start your own chat.