Procedure of giving catheter
Reading File
Finding Sources
Finding Sources
Searching Images
urinary catheterization procedure
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Now I have comprehensive information from the textbooks. Let me compile a thorough answer.
Urinary Catheterization — Procedure
Overview
Urethral catheterization is the most frequently performed retrograde manipulation of the urinary tract; over 100 million Foley catheters are used annually. The procedure drains the bladder during and after surgical procedures, monitors urine output in critically ill patients, collects sterile urine specimens, and relieves urinary obstruction.
— Smith and Tanagho's General Urology, 19th Ed.
Indications
- Acute urinary retention
- Urethral or prostatic obstruction compromising renal function
- Urine output monitoring in critically ill/injured patients
- Collection of a sterile urine specimen
- Intermittent bladder catheterization in neurogenic bladder dysfunction
- Urologic study of the lower urinary tract
Contraindications
- Suspected urethral disruption from pelvic trauma (blood at the meatus, perineal hematoma, high-riding prostate)
- Recent reconstructive surgery of the urethra or bladder neck (relative)
- Known urethral stricture (relative — may dilate)
- Acute infection of the prostate/urethra (relative)
- Combative or uncooperative patient (relative)
Equipment
| Item | Purpose |
|---|---|
| Foley catheter (16–18 Fr adult) | Self-retaining indwelling catheter; 2-lumen (drainage + balloon) or 3-lumen (+ irrigation port) |
| Robinson catheter | Non-retaining, for intermittent/single-use drainage |
| Coudé catheter | Curved tip for males >50 yr with enlarged prostate or elevated bladder neck |
| Sterile drapes & gloves | Aseptic field |
| Antiseptic solution (povidone-iodine or chlorhexidine) | Meatal cleansing |
| Water-soluble lubricant / 2% lidocaine gel | Lubrication and local anesthesia |
| 10 mL syringe + sterile water | Balloon inflation |
| Drainage bag | Closed-system collection |
Anatomical Considerations
Female urethra: Short (~4 cm), straight, wide-caliber tube lying on top of the vagina. The meatus is oval/slit-like, ~2.5 cm inferior to the clitoris, immediately superior to the vaginal introitus. It may recede intravaginally in postmenopausal or post-surgical patients.
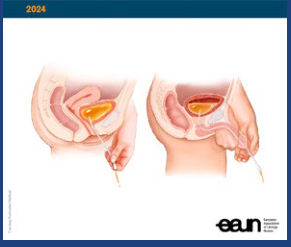
Male urethra: ~20 cm long from meatus to bladder neck. The prostatic and membranous urethra together can span up to 7 cm. The penis must be held taut and directed toward the umbilicus to straighten the urethral folds — otherwise the catheter will kink and fail to advance even without an anatomic blockage.
Step-by-Step Procedure
Preparation
- Explain the procedure to the patient and obtain consent. Apprehension is common — reassurance about positioning reduces patient anxiety.
- Position the patient:
- Female: Supine, frog-leg or lithotomy (stirrups preferred). Adequate hip abduction is essential — adducted legs make catheterization very difficult.
- Male: Supine.
- Gather all equipment before starting. Once the genitalia have been touched with the nondominant hand, that hand is contaminated and must not handle sterile equipment.
- Open the catheterization tray and establish a sterile field at the bedside.
- Don sterile gloves.
Cleansing
- With the nondominant hand, expose the meatus:
- Female: Separate the labia minora and hold throughout the procedure.
- Male: Retract the foreskin (if present), expose the glans.
- With the dominant hand, cleanse the meatus and surrounding area with antiseptic solution in a circular motion from the meatus outward. Use separate swabs for each wipe.
Lubrication & Anesthesia
- Lubricate the catheter generously with water-soluble jelly.
- Males: Instill 5 mL of 2% viscous lidocaine (or anesthetic lubricant gel) into the urethra via syringe before passing the catheter — this provides topical anesthesia and distends the urethra. Warn the patient of mild urethral discomfort and the urge to void.
Catheter Insertion
Female:
- Identify the urethral meatus (first opening superior to the vaginal introitus).
- Gently pass the catheter ~7–8 cm (3 inches) following the slight posterior-to-downward urethral course toward the bladder.
- Urine flow confirms correct bladder placement. Any catheter that inadvertently enters the vagina must be discarded and a fresh catheter used.
Male:
- Hold the penis taut and directed toward the umbilicus with the nondominant hand to straighten urethral folds.
- With the dominant hand, pass the catheter slowly and gently up the full length of the catheter — advance to the junction of the catheter and the balloon inflation port (the "hilt"). This is critical: inflating the balloon within the urethra causes significant injury.
- Urine flow confirms bladder placement.
- For men >50 years or known BPH, a coudé catheter with the curved tip directed at 12 o'clock (anterior) is preferred to navigate the prostatic urethra.
Balloon Inflation & Securing
- Inflate the balloon with 10 mL of sterile water or tap water (not saline — it can crystallize in the valve over time; however, either is acceptable clinically).
- If resistance or perineal/penile discomfort occurs during inflation → immediately deflate, reposition or advance the catheter further, then re-inflate. Resistance indicates the balloon is still in the urethra.
- Gently withdraw the catheter until you feel resistance — the balloon is now seated at the bladder neck.
- Connect to a closed-drainage bag. Secure the catheter to the inner thigh (female) or lower abdomen/thigh (male) with tape to prevent traction injury.
- Replace the foreskin (if retracted in uncircumcised males) to prevent iatrogenic paraphimosis — this is a commonly missed step.
Post-Procedure
- Document the residual urine volume drained.
- If >500–1000 mL is obtained acutely, clamp temporarily to prevent decompression haematuria (some clinicians); evidence is mixed.
- Maintain a closed drainage system at all times; keep the bag below bladder level to prevent reflux.
- Use the smallest suitable catheter bore to minimize urethral trauma.
Complications
| Complication | Notes |
|---|---|
| Urinary tract infection (CAUTI) | Most common; risk increases with catheter dwell time |
| Urethral trauma / false passage | From forced passage, especially in males |
| Iatrogenic paraphimosis | Foreskin not replaced after insertion |
| Balloon inflation in urethra | Occurs when catheter not fully advanced in males |
| Transient hematuria | Common after difficult catheterization |
| Bladder spasm | From balloon irritation |
Catheter Care Guidelines (CDC Category I — Strongly Recommended)
- Use catheters only when indicated; remove as soon as possible
- Maintain a closed sterile drainage system
- Obtain urine specimens aseptically (via sampling port, not by breaking the circuit)
- Maintain unobstructed urine flow
- Hand hygiene before and after any catheter manipulation
— Pfenninger and Fowler's Procedures for Primary Care; Roberts and Hedges' Clinical Procedures in Emergency Medicine
Insulin synringe giving procedure
Reading File
Finding Sources
Finding Sources
Searching Images
insulin syringe subcutaneous injection technique sites
You've run out of free credits. Sign up for a free account to continue using Orris.
This is a shared conversation. Sign in to Orris to start your own chat.