Explain spinal cord
Reading File
Finding Sources
Searching Images
spinal cord anatomy cross section diagram
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
I now have comprehensive content. Let me compile a thorough, well-organized response:
The Spinal Cord
Overview
The spinal cord is the most caudal portion of the central nervous system (CNS). It extends from the foramen magnum (base of skull) to approximately the level of the L1–L2 intervertebral disc in adults (range: T12 to the L2–L3 disc). In neonates, it extends to about L3–L4, as the vertebral column grows faster than the cord postnatally.
The distal, cone-shaped end is the conus medullaris, from which a fine connective tissue filament — the filum terminale — continues inferiorly to the coccyx.
- Gray's Anatomy for Students, p. 119
Gross Structure
Enlargements
The cord is not uniform — it has two bulges corresponding to limb innervation:
| Enlargement | Segments | Innervates |
|---|---|---|
| Cervical | C5–T1 | Upper limbs |
| Lumbosacral | L1–S3 | Lower limbs |
External Surface Markings
- Anterior median fissure — runs the full anterior length
- Posterior median sulcus — runs the full posterior length
- Posterolateral sulci (bilateral) — where posterior rootlets enter the cord
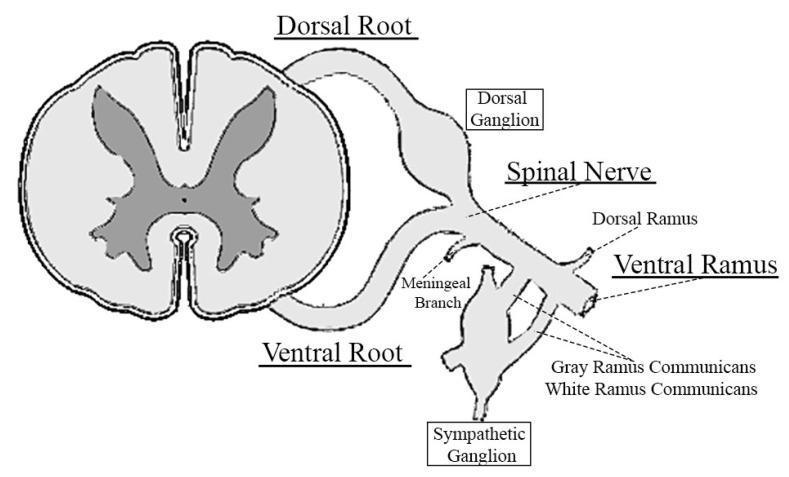
Spinal Segments & Nerves
The spinal cord has 31 segments, each giving rise to a pair of spinal nerves:
- 8 cervical (C1–C8)
- 12 thoracic (T1–T12)
- 5 lumbar (L1–L5)
- 5 sacral (S1–S5)
- 1 coccygeal
Because the cord ends at L1–L2 but the vertebral column continues to the sacrum, the lumbar and sacral nerve roots descend within the spinal canal as the cauda equina before exiting.
Internal Organization
In cross-section, the cord has two distinct zones:
Gray Matter (Central)
- Rich in neuronal cell bodies; forms a characteristic H-shaped (butterfly) appearance
- Divided into:
- Dorsal (posterior) horn — receives sensory input
- Ventral (anterior) horn — contains motor neurons
- Intermediolateral (lateral) horn — present at T1–L2 (sympathetic preganglionic neurons) and S2–S4 (parasympathetic)
- Gray commissure — connects the two halves, enclosing the central canal
Rexed's Laminae
The gray matter is further divided into 10 cytoarchitectural zones (Rexed's laminae):
| Lamina | Region | Key Function |
|---|---|---|
| I | Posteromarginal nucleus | Pain/temp modulation |
| II | Substantia gelatinosa (Rolando) | Pain modulation (gate control) |
| III–IV | Nucleus proprius | General sensory processing |
| V–VI | Base of dorsal horn / nucleus reticularis | Sensory convergence |
| VII | Intermediate zone (Clarke's nucleus) | Spinocerebellar pathways |
| VIII–IX | Ventral horn | Motor output |
| X | Around central canal | Gray commissure zone |
The ventral horn contains two motor neuron types:
- Alpha (α) motor neurons → innervate extrafusal skeletal muscle fibers
- Gamma (γ) motor neurons → innervate intrafusal fibers of muscle spindles (stretch reflex receptors)
- Somatotopic arrangement: flexor neurons are dorsal to extensor neurons; hand muscles are lateral to trunk muscles.
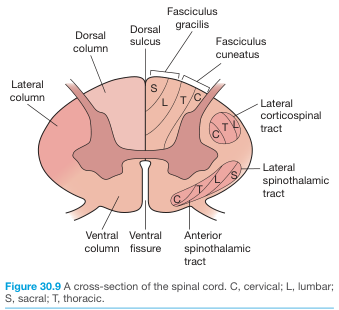
White Matter (Peripheral)
Surrounds the gray matter; rich in myelinated axons organized into three funiculi per side:
| Funiculus | Location | Contents |
|---|---|---|
| Dorsal (posterior) | Between dorsomedian and dorsolateral sulci | Ascending sensory tracts |
| Lateral | Between dorsolateral and ventrolateral sulci | Mixed ascending + descending tracts |
| Ventral (anterior) | Between ventrolateral sulcus and anterior fissure | Descending motor tracts |
- Localization in Clinical Neurology, 8th ed., p. 242–244
- Gray's Anatomy for Students
Ascending (Sensory) Tracts
Two major somatosensory pathways ascend to the cortex:
1. Posterolateral (Anterolateral) Pathway — Spinothalamic Tract
- Modalities: Pain, temperature, crude touch, pressure
- 1st neuron: Dorsal root ganglion → enters posterior horn
- 2nd neuron: Crosses in the anterior commissure (contralateral, 2–3 segments above entry) → ascends in the lateral funiculus as the lateral spinothalamic tract
- 3rd neuron: Ventral posterior lateral (VPL) nucleus of thalamus → primary somatosensory cortex (S1)
- The spinoreticular and spinomesencephalic tracts accompany this pathway for arousal and affective pain responses.
2. Posterior Column–Medial Lemniscal Pathway (Dorsal Columns)
- Modalities: Fine/discriminative touch, vibration, conscious proprioception
- 1st neuron: Dorsal root ganglion → ascends ipsilaterally in the dorsal funiculus:
- Fasciculus gracilis (medial) — lower limb and trunk (below T6)
- Fasciculus cuneatus (lateral) — upper limb and neck (above T6)
- 2nd neuron: Crosses in the caudal medulla as internal arcuate fibers → ascends as the medial lemniscus (contralateral)
- 3rd neuron: VPL nucleus thalamus → S1 cortex
Key clinical rule: Spinothalamic decussates within the cord (contralateral signs at the level of injury); dorsal columns decussate in the medulla (ipsilateral signs at cord level).
- Gray's Anatomy for Students; Localization in Clinical Neurology, 8th ed.
Descending (Motor) Tracts
Lateral Motor System
| Tract | Origin | Decussation | Location in cord | Function |
|---|---|---|---|---|
| Lateral corticospinal tract | Motor cortex (UMN) | Pyramidal decussation (caudal medulla, ~85%) | Lateral funiculus | Voluntary fine motor, especially distal limb |
| Rubrospinal tract | Red nucleus (midbrain) | Ventral tegmental decussation | Lateral funiculus | Flexor facilitation; minor in humans |
Medial Motor System
| Tract | Origin | Projection |
|---|---|---|
| Anterior corticospinal tract | Motor cortex (~15% non-decussated) | Descends ipsilaterally; crosses at segmental level; controls axial/proximal muscles |
| Tectospinal tract | Superior colliculus | Cervical cord; reflex postural responses to visual stimuli |
| Vestibulospinal tract (medial + lateral) | Vestibular nuclei (pons/medulla) | Postural tone, balance, extensor facilitation |
| Reticulospinal tracts | Pontine + medullary reticular formation | Gait, posture, autonomic modulation |
- Gray's Anatomy for Students, p. 1327–1332
Autonomic Outflow
- Sympathetic: Preganglionic cell bodies in the intermediolateral column, segments T1–L2 → exit via anterior roots → synapse in paravertebral or prevertebral ganglia
- Parasympathetic (sacral): Preganglionic neurons in the S2–S4 intermediate gray → form the pelvic splanchnic nerves → innervate pelvic viscera (bladder, bowel, genitalia)
Blood Supply
The spinal cord is supplied by three longitudinal arteries:
| Artery | Number | Origin | Territory |
|---|---|---|---|
| Anterior spinal artery (ASA) | 1 (midline) | Vertebral arteries at craniocervical junction | Anterior 2/3 of cord — corticospinal, spinothalamic tracts, anterior horn |
| Posterior spinal arteries (PSA) | 2 (posterolateral) | PICA or vertebral arteries | Posterior 1/3 — dorsal columns |
These are reinforced by radiculomedullary arteries segmentally from the aorta. The most important is the artery of Adamkiewicz (artery of the lumbar enlargement), arising from the lower thoracic/upper lumbar aorta (usually T9–T12, left side), which is the dominant supply to the lower thoracic and lumbosacral cord.
Blood supply is sparse in the mid-thoracic region (T4–T8), making it a watershed zone vulnerable to ischemia.
Anterior Spinal Artery Syndrome: Infarction of the ASA territory (aortic dissection, surgery, embolism) causes:
-
Bilateral motor paralysis below the lesion (corticospinal tract)
-
Loss of pain and temperature below the lesion (spinothalamic tract)
-
Preserved vibration and proprioception (dorsal columns, supplied by PSA)
-
Autonomic dysfunction (bladder/bowel incontinence, hypotension)
-
Miller's Anesthesia, 10th ed., p. 8016–8018
Key Images
Clinical Summary: Spinal Cord Syndromes
| Syndrome | Lesion | Features |
|---|---|---|
| Complete transection | All tracts | Complete loss of motor + all sensation + autonomic below level |
| Brown-Séquard | Hemisection | Ipsilateral motor loss + proprioception; contralateral pain/temp loss |
| Anterior cord syndrome | ASA infarction | Bilateral motor + pain/temp loss; proprioception spared |
| Central cord syndrome | Central gray/commissure | Upper > lower limb weakness; dissociated sensory loss |
| Posterior cord syndrome | Dorsal columns | Loss of proprioception + vibration; motor/pain preserved |
| Conus medullaris | L1–L2 | Mixed UMN/LMN; bladder/bowel prominent |
| Cauda equina | Below L2 | Pure LMN; radicular pain; saddle anesthesia |
Sources: Gray's Anatomy for Students | Localization in Clinical Neurology, 8th ed. | Costanzo Physiology, 7th ed. | Miller's Anesthesia, 10th ed. | Bailey & Love's Surgery, 28th ed.
This is a shared conversation. Sign in to Orris to start your own chat.