Clinical presentation of breast disease Types of epithelial lesions TNM Staging of breast diseases references from standard pathology textbook
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Here is the complete, referenced coverage of all three topics from standard pathology textbooks.
Breast Disease: Pathology Reference Guide
Primary Sources:
- Robbins, Cotran & Kumar - Pathologic Basis of Disease (10th Ed.)
- Robbins & Kumar Basic Pathology (10th Ed.)
- Schwartz's Principles of Surgery (11th Ed.) - AJCC 8th Edition TNM
1. Clinical Presentations of Breast Disease
The predominant symptoms and signs of breast disease are:
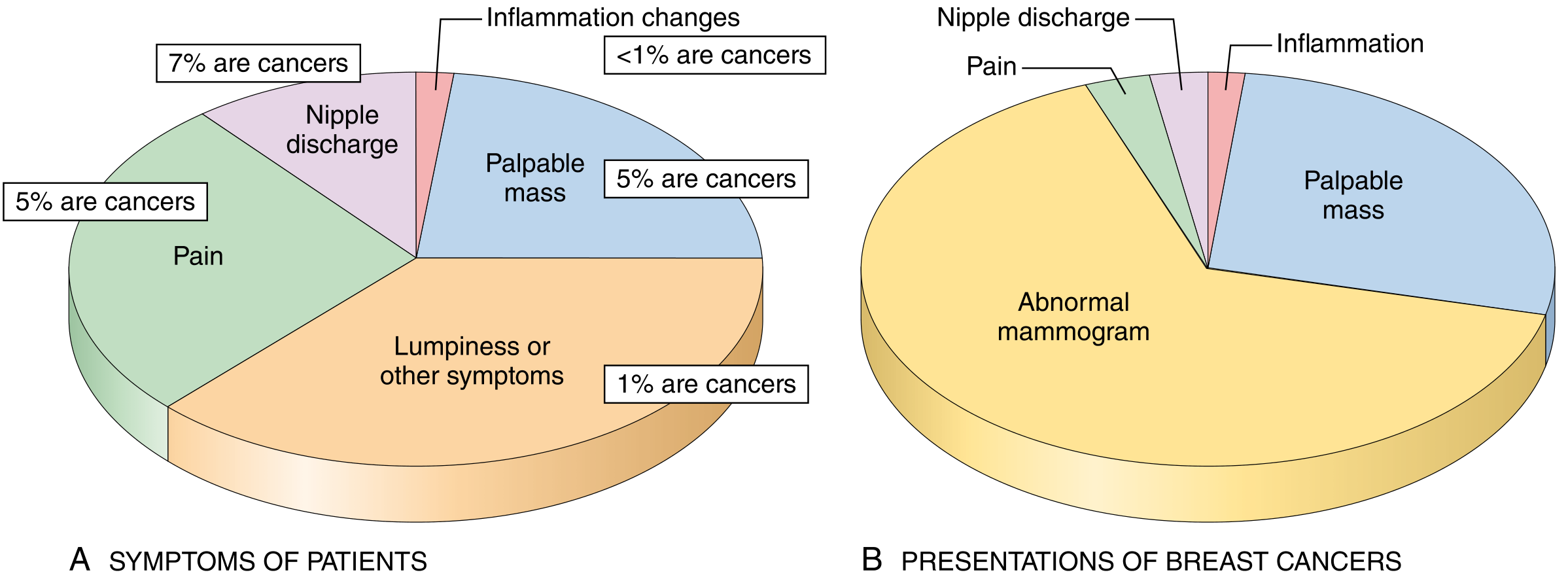
Greater than 90% of symptomatic breast lesions are benign. Of females with cancer, about 45% have symptomatic disease, while the remainder come to attention through mammographic screening.
1.1 Lumpiness (Diffuse Nodularity)
- Usually a manifestation of normal glandular tissue or fibrocystic changes
- When pronounced, imaging studies may be needed to exclude a discrete mass
- This is the most common presenting symptom, but only 1% of such cases represent cancers
1.2 Pain (Mastalgia / Mastodynia)
- Very common; may be cyclic (with menses - due to premenstrual edema) or noncyclic
- Noncyclic pain is usually localized and may be caused by: ruptured cyst, physical injury, infection, or fat necrosis
- Often no specific lesion is identified
- Important: in approximately 5% of cases, the underlying cause is breast cancer
1.3 Palpable Mass
- Detected when 2-3 cm in size
- About 95% of palpable masses are benign
- Benign features: discrete, round or oval, rubbery, mobile (e.g., fibroadenoma, cyst)
- Malignant features: irregular (spiculated), hard (scirrhous), nonmobile - because malignant tumors invade across tissue planes
- Likelihood of malignancy increases with age:
- Under age 40: ~10% chance of malignancy
- Over age 50: ~60% chance of malignancy
- Distribution of carcinomas by quadrant:
- Upper outer quadrant: ~50%
- Each remaining quadrant: ~10%
- Central/subareolar region: ~20%
1.4 Nipple Discharge
- Normal in small quantities if bilateral
- Milky discharge (galactorrhea): associated with elevated prolactin (pituitary adenoma), hypothyroidism, anovulatory syndromes, oral contraceptives, tricyclic antidepressants, methyldopa, phenothiazines - not a feature of malignancy
- Bloody or serous discharge: most commonly due to large duct papillomas and cysts
- Discharge of greatest concern for malignancy: spontaneous, unilateral, bloody, in an older patient
- Discharge associated with malignancy (most commonly DCIS) accounts for 7% of cases in women under 60, and 30% in women 60 years or older
1.5 Inflammatory Changes
- Erythema and edema involving all or part of a breast
- Most often caused by infections, usually in the setting of lactation/breastfeeding (acute bacterial mastitis)
- Critical mimic: "Inflammatory" breast carcinoma - must always be considered when evaluating breast inflammation
1.6 Mammographic Abnormalities (Asymptomatic)
- Most cancers in women over 50 are now detected by mammography
- Principal mammographic signs of breast carcinoma: densities and calcifications
- Sensitivity and specificity of mammography increase with age
- Likelihood that an abnormal mammographic finding is malignant:
- Age 40: ~10%
- Over age 50: >25%
1.7 Gynecomastia (Males)
- The only common breast symptom in males
- Increase in both stroma and epithelial cells due to an imbalance between estrogens (stimulatory) and androgens (inhibitory)
2. Types of Epithelial Lesions of the Breast
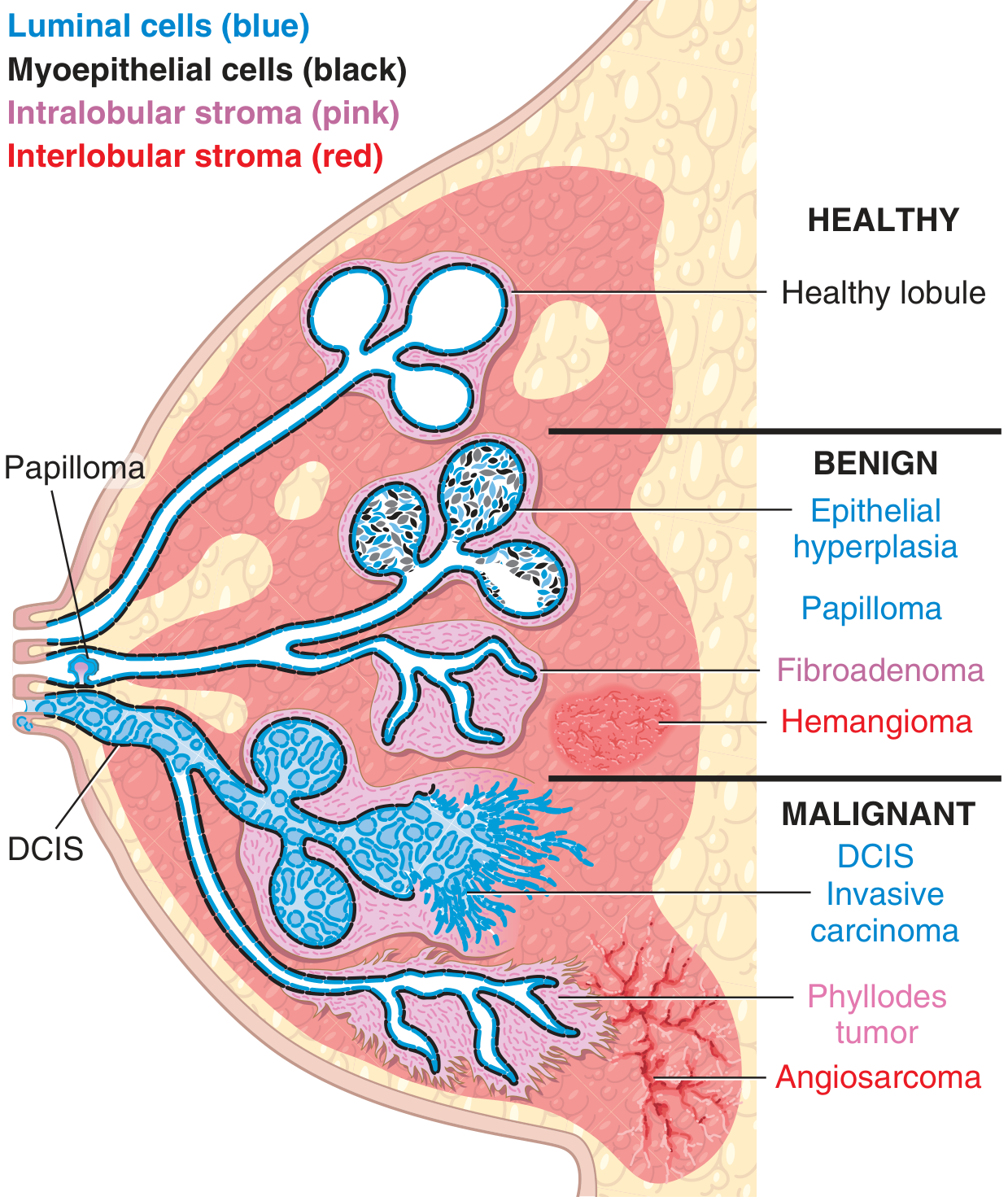
Most benign epithelial lesions arise in the terminal duct lobular unit (TDLU) and are classified into three groups based on the risk of subsequent breast cancer development:
Group 1: Nonproliferative Breast Changes (Fibrocystic Changes)
No increased risk of breast cancer
- Most common between ages 30-50 years, possibly due to cyclic hormonal changes
Three principal morphologic features:
a) Cystic Change
- Small cysts form by dilation of lobules and terminal ducts, lined by flattened atrophic epithelium
- Large cysts (>3 mm) have a blue-dome appearance grossly (tension cysts)
- Apocrine metaplasia is common - cells with abundant granular eosinophilic cytoplasm resembling apocrine sweat gland cells
b) Fibrosis
- Cyst rupture releases secretions into stroma, causing chronic inflammation and fibrosis
- Dense fibrous tissue replaces normal breast stroma
c) Adenosis
- Increase in the number of acini per lobule
- Regular form is normal during pregnancy; in pathological adenosis, acini may be enlarged
- Sclerosing adenosis: a specific variant - enlarged terminal duct lobular unit with compressed and distorted acini in dense fibrotic stroma; can mimic carcinoma clinically and radiologically; calcifications may be present
Group 2: Proliferative Breast Disease Without Atypia
Slightly increased risk (1.5-2x) of breast cancer
a) Epithelial Hyperplasia (Usual Ductal Hyperplasia)
- Increase in the number of cells in acini and ducts relative to the basement membrane
- Cells fill and distend the lumen; irregular "streaming" pattern of cells with overlapping nuclei
- Variable cell morphology
b) Sclerosing Adenosis (can also fall here depending on extent)
- Florid form associated with slightly increased cancer risk
c) Radial Scar (Complex Sclerosing Lesion)
- Central nidus of small tubules entrapped in a densely fibrotic stroma with long radiating projections
- Radiographically mimics carcinoma (irregular central mass with spiculated projections)
- Microscopically: epithelium shows varying degrees of cyst formation, hyperplasia, and adenosis in projections
d) Intraductal Papilloma
- Papillary growth within a large duct, with a central fibrovascular core lined by myoepithelial and luminal cells
- Presents as spontaneous, often bloody nipple discharge
- Usually solitary (central), located in the large ducts below the nipple
- Multiple peripheral papillomas carry a slightly higher cancer risk
Group 3: Proliferative Breast Disease With Atypia (Atypical Hyperplasia)
Moderately increased risk (4-5x) of breast cancer; risk rises to 10x with a positive family history
a) Atypical Ductal Hyperplasia (ADH)
- Monomorphic proliferation that partially fills ducts
- Has some but not all histologic features of low-grade ductal carcinoma in situ (DCIS)
- Differs from DCIS: smaller in extent, incompletely fills duct spaces, or lacks high-grade nuclear features
- Found in ~10% of biopsies performed to evaluate calcifications
b) Atypical Lobular Hyperplasia (ALH)
- Clonal proliferation of cells with features similar to lobular carcinoma in situ (LCIS), but incompletely fills or distends fewer than 50% of the acini in a lobule
- Incidental finding; found in <5% of biopsies
- Identical cytology to LCIS (small, uniform, discohesive cells lacking E-cadherin expression)
Group 4: Carcinoma In Situ (High Risk / Precursor Lesions)
a) Ductal Carcinoma In Situ (DCIS)
- Malignant epithelial cells confined within the basement membrane
- Most common form of noninvasive carcinoma (~80% of carcinoma in situ)
- Classified by architectural pattern (comedo, cribriform, solid, papillary, micropapillary) and nuclear grade (low, intermediate, high)
- Comedo DCIS: high-grade cells with central necrosis; calcifications are common (detected on mammography)
- Without treatment, ~50% will progress to invasive carcinoma within 10 years
b) Lobular Carcinoma In Situ (LCIS)
- Clonal proliferation of cells with lobular cytology that fills and distends acini
- Generally incidental finding; not usually detectable on mammography
- Cells are small, uniform, round/discohesive, with intracytoplasmic mucin vacuoles
- Lack E-cadherin (diagnostic immunohistochemical marker)
- Removed from TNM staging in AJCC 8th edition - classified as a benign entity / risk indicator
- Bilateral in ~20-40% of patients
Columnar Cell Lesions and Flat Epithelial Atypia
- Thought to be the earliest morphologically recognizable precursors in the low-grade breast neoplasia pathway
- Present as calcifications on mammographic screening
- Columnar cell lesions: variably dilated acini lined by columnar epithelial cells, often with apical snouts, with microcalcifications
- Flat epithelial atypia (FEA): columnar cell lesion with cytologic atypia but without architectural complexity (distinguishes it from ADH)
3. TNM Staging of Breast Cancer (AJCC 8th Edition)
Reference: Schwartz's Principles of Surgery, 11th Ed., Table 17-10, citing AJCC Cancer Staging Manual, 8th Ed. (2017)
T - Primary Tumor
| Stage | Definition |
|---|---|
| TX | Primary tumor cannot be assessed |
| T0 | No evidence of primary tumor |
| Tis (DCIS) | Ductal carcinoma in situ |
| Tis (Paget) | Paget disease of the nipple NOT associated with invasive carcinoma and/or DCIS in the underlying breast parenchyma |
| T1 | Tumor ≤20 mm in greatest dimension |
| T1mi | Tumor ≤1 mm (microinvasion) |
| T1a | Tumor >1 mm but ≤5 mm |
| T1b | Tumor >5 mm but ≤10 mm |
| T1c | Tumor >10 mm but ≤20 mm |
| T2 | Tumor >20 mm but ≤50 mm |
| T3 | Tumor >50 mm |
| T4 | Tumor of any size with direct extension to chest wall and/or skin (ulceration or macroscopic nodules); invasion of dermis alone does NOT qualify |
| T4a | Extension to chest wall (invasion/adherence to pectoralis muscle alone does not qualify) |
| T4b | Ulceration and/or ipsilateral macroscopic satellite nodules and/or edema (including peau d'orange) not meeting criteria for inflammatory carcinoma |
| T4c | Both T4a and T4b |
| T4d | Inflammatory carcinoma |
Note: LCIS is removed from TNM staging in the AJCC 8th edition - classified as a benign entity.
N - Regional Lymph Nodes
Clinical N (cN)
| Stage | Definition |
|---|---|
| cNX | Regional lymph nodes cannot be assessed |
| cN0 | No regional lymph node metastases (by imaging or clinical examination) |
| cN1 | Metastases to movable ipsilateral Level I, II axillary lymph node(s) |
| cN1mi | Micrometastases (>0.2 mm and/or >200 cells, but ≤2 mm) |
| cN2 | Metastases in fixed/matted ipsilateral Level I, II axillary nodes; OR clinically detected internal mammary nodes in absence of axillary node metastases |
| cN2a | Fixed or matted axillary lymph node metastases |
| cN2b | Internal mammary nodes by imaging, without axillary node metastases |
| cN3 | Metastases to ipsilateral infraclavicular (Level III axillary) nodes; OR internal mammary nodes + axillary nodes; OR ipsilateral supraclavicular nodes |
Pathologic N (pN)
| Stage | Definition |
|---|---|
| pNX | Regional lymph nodes cannot be assessed |
| pN0 | No regional lymph node metastasis or ITCs only |
| pN0(i+) | ITCs only (malignant cell clusters ≤0.2 mm) |
| pN0(mol+) | Positive by RT-PCR; no ITCs detected |
| pN1 | Micrometastases; OR metastases in 1-3 axillary nodes; AND/OR clinically negative internal mammary nodes with micrometastases or macrometastases by sentinel node biopsy |
| pN1mi | Micrometastases (>0.2 mm but ≤2 mm, ~200 cells) |
| pN1a | Metastases in 1-3 axillary nodes (at least one >2 mm) |
| pN1b | Metastases in ipsilateral internal mammary sentinel nodes, excluding ITCs |
| pN1c | pN1a + pN1b combined |
| pN2 | Metastases in 4-9 axillary nodes; OR positive ipsilateral internal mammary nodes by imaging in absence of axillary node metastases |
| pN2a | 4-9 axillary nodes (at least one deposit >2 mm) |
| pN2b | Clinically detected internal mammary nodes with/without microscopic confirmation; with pathologically negative axillary nodes |
| pN3 | ≥10 axillary nodes; OR infraclavicular (Level III) nodes; OR internal mammary nodes by imaging + ≥1 positive Level I/II axillary nodes; OR >3 axillary nodes + micrometastases by sentinel biopsy; OR ipsilateral supraclavicular nodes |
| pN3a | ≥10 axillary nodes (at least one >2 mm); OR infraclavicular (Level III) nodes |
| pN3b | Internal mammary nodes + axillary node involvement as per criteria |
| pN3c | Ipsilateral supraclavicular nodes |
M - Distant Metastasis
| Stage | Definition |
|---|---|
| M0 | No clinical or radiographic evidence of distant metastases |
| cM0(i+) | No clinical/radiographic evidence of distant metastases, but tumor cells/deposits ≤0.2 mm detected microscopically or by molecular techniques in blood, bone marrow, or other non-regional nodal tissue |
| M1 | Distant detectable metastases as determined by classic clinical and radiographic means, and/or histologically confirmed >0.2 mm |
Anatomic Stage Groups (AJCC 8th Edition)
| Stage | T | N | M |
|---|---|---|---|
| 0 | Tis | N0 | M0 |
| IA | T1 | N0 | M0 |
| IB | T0 or T1 | N1mi | M0 |
| IIA | T0 or T1 | N1 | M0 |
| IIA | T2 | N0 | M0 |
| IIB | T2 | N1 | M0 |
| IIB | T3 | N0 | M0 |
| IIIA | T0, T1, or T2 | N2 | M0 |
| IIIA | T3 | N1 or N2 | M0 |
| IIIB | T4 | N0, N1, or N2 | M0 |
| IIIC | Any T | N3 | M0 |
| IV | Any T | Any N | M1 |
Special notations:
- "c" or "p" prefix denotes clinical vs. pathologic staging (pathologic takes precedence for T)
- "sn" suffix = sentinel node biopsy confirmation
- "f" suffix = FNA/core needle biopsy confirmation (no further node resection)
- Staging after neoadjuvant therapy uses "yc" or "yp" prefix
- No anatomic stage group is assigned for complete pathological response (pCR): ypT0ypN0cM0
Key Concepts Summary
| Epithelial Lesion | Risk of Breast Cancer |
|---|---|
| Nonproliferative changes (fibrocystic) | No increased risk |
| Proliferative disease without atypia (usual hyperplasia, papilloma, radial scar) | 1.5-2x |
| Atypical hyperplasia (ADH or ALH) | 4-5x (10x with family history) |
| LCIS | 8-10x (risk indicator, bilateral) |
| DCIS | Direct precursor; ~50% progress to invasive carcinoma |
References:
- Robbins, Cotran & Kumar. Pathologic Basis of Disease, 10th Ed. Chapter 23: The Breast, pp. 961-966
- Kumar, Abbas & Aster. Robbins & Kumar Basic Pathology, 10th Ed. Chapter 17, pp. 705-706
- Schwartz. Principles of Surgery, 11th Ed. Table 17-10 (AJCC Cancer Staging Manual, 8th Ed., 2017)
This is a shared conversation. Sign in to Orris to start your own chat.