
Screenshot_20260619-203246.png
Explain ovarian cancer
Reading File
Finding Sources
Finding Sources
Searching PubMed
"ovarian neoplasms"[MeSH Terms] AND "classification"[MeSH Terms]
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive content from multiple authoritative sources to write a thorough answer covering all aspects of PA 29.4. Let me compose the full response:
Ovarian Tumors - Complete Classification, Etiology, Pathogenesis, Morphology, Clinical Course, Spread & Complications
Sources: Berek & Novak's Gynecology, Harrison's Principles of Internal Medicine 22E, Robbins Pathologic Basis of Disease, Bailey & Love's Surgery
1. Overview & Epidemiology
Ovarian cancer is the sixth most common malignancy in women. An American woman has approximately a 1-in-72 lifetime risk (1.6%) of developing ovarian cancer. In 2024, ~19,710 new cases and >13,270 deaths are expected in the US. The peak incidence for sporadic tumors is in women in their fifties and sixties. The overall 5-year survival is <50% because approximately two-thirds of women present with advanced (Stage III-IV) disease.
2. Classification of Ovarian Tumors
Ovarian tumors are classified by their cell of origin into three broad groups:
| Category | Proportion | Age Group |
|---|---|---|
| Epithelial tumors | ~65-70% of all ovarian tumors | Postmenopausal (50-70 yrs) |
| Germ cell tumors | 15-20% | Children & young adults |
| Sex cord-stromal tumors | ~8% | Any age |
Each category is further divided into benign, borderline (low malignant potential), and malignant subtypes.
3. Epithelial Ovarian Tumors (Most Important)
These arise from the surface epithelium of the ovary (or, more accurately, from the fallopian tube epithelium and endometriosis).
Histologic Subtypes (WHO Classification)
| Type | Cell Resemblance | Frequency |
|---|---|---|
| Serous | Fallopian tube (endosalpingeal) | 75-80% of malignant epithelial |
| Endometrioid | Endometrial glands | 10% |
| Mucinous | GI/endocervical epithelium | 5% |
| Clear cell | Mullerian / secretory endometrium | 5% |
| Brenner | Transitional (urothelium) | <1% |
| Undifferentiated | - | <1% |
Each type can be: A. Benign / B. Borderline / C. Malignant
Key Concept: Type 1 vs. Type 2 Serous Tumors
| Feature | Type 1 | Type 2 |
|---|---|---|
| Grade | Low-grade | High-grade |
| Behavior | Indolent | Rapidly progressive |
| Mutations | KRAS, BRAF, PTEN, PIK3CA | TP53 (95%), BRCA1/2 |
| Genetic stability | Stable | Highly unstable |
| Stage at diagnosis | Often early | Usually advanced |
| Includes | Borderline tumors, low-grade serous, mucinous, endometrioid | High-grade serous carcinoma |
4. Etiology & Risk Factors
Genetic / Hereditary Factors
- BRCA1 (chromosome 17q12-21): Lifetime ovarian cancer risk 39-63%; BRCA2 (13q12-13): 16.5-27%
- BRCA1/2 are components of the homologous DNA double-strand break repair machinery
- Women with BRCA1 mutations typically develop ovarian cancer in their 40s-50s; BRCA2 carriers in their 50s-60s
- Lynch syndrome (MLH1, MSH2, MSH6, PMS2 mutations) - associated with endometrioid ovarian tumors
- PALB2 and other homologous repair genes also confer risk
Hormonal / Reproductive Factors ("Incessant Ovulation" Hypothesis)
- Nulliparity and infertility - increased risk
- Early menarche and late menopause (longer ovulatory career) - increased risk
- Hormone replacement therapy (controversial)
- Protective: Oral contraceptive use (50% risk reduction with 5+ years use), multiparity (0.3-0.4 risk reduction per child), tubal ligation, breast-feeding, aspirin use
Environmental Factors
- Obesity, high-fat diet
- Talc exposure (controversial, peritoneal route)
- Infertility treatments
5. Pathogenesis
Modern Understanding: Fallopian Tube Origin
Previously thought to arise from coelomic epithelium of the ovary or ovarian inclusion cysts, it is now established that:
- Most high-grade serous carcinomas originate from the fimbriated end of the fallopian tube
- Serous tubal intraepithelial carcinoma (STIC) lesions are identifiable in risk-reducing salpingo-oophorectomy specimens from BRCA carriers
- Clear cell and endometrioid types arise from endometriosis
Molecular Pathogenesis
Type 2 (high-grade serous):
- Germline or somatic loss of BRCA1/2 function in fallopian tube epithelium
- TP53 mutation (seen in ~95% of cases) - the earliest detectable change
- Intraepithelial carcinoma (STIC) forms in the tubal fimbriae
- Tumor cells shed from the tube, spread to the ovarian surface and peritoneal cavity
- MUC16 (CA-125) expression on cancer cells facilitates binding to mesothelin on peritoneal cells
- Widespread genomic instability: amplifications, deletions (NF1, RB1, CDK12)
Type 1 (low-grade/borderline):
- Stepwise progression: benign → borderline → invasive (the "adenoma-carcinoma sequence")
- Driven by activating mutations in KRAS, BRAF (MAP kinase pathway), PTEN, PIK3CA
6. Pathology & Morphology
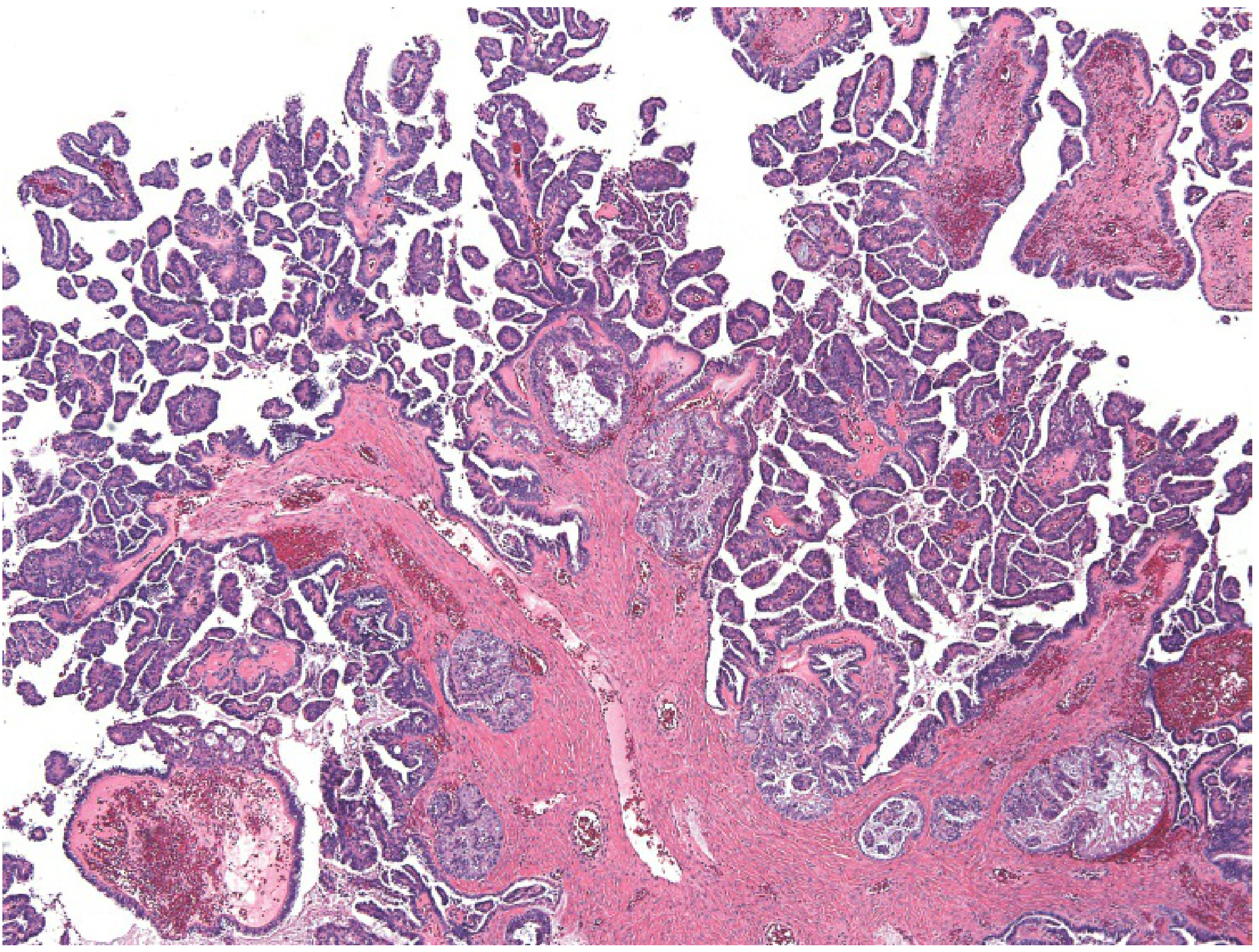
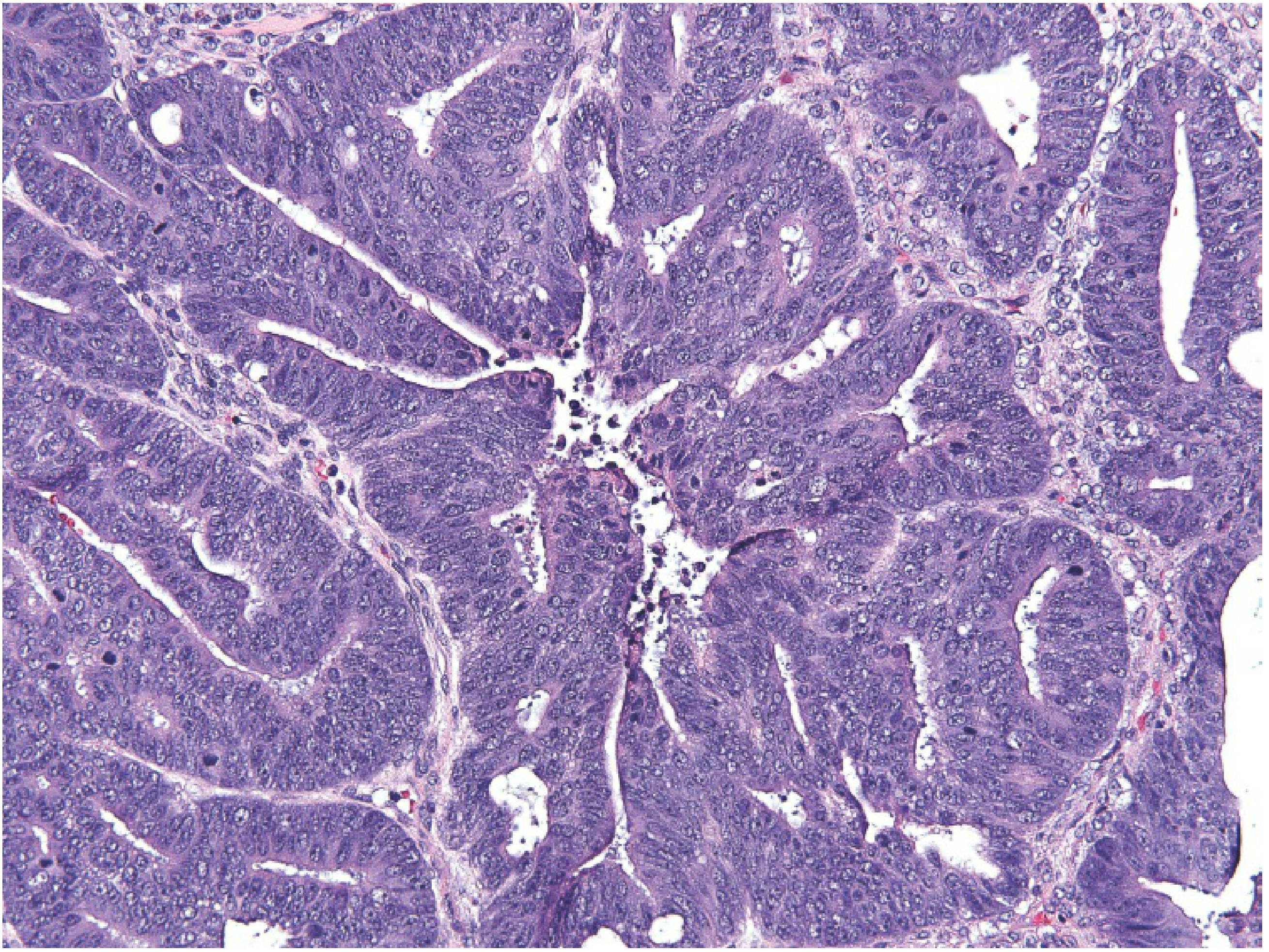
Serous Tumors
Gross: Bilateral cystic masses with papillary projections; may be large. High-grade tumors have solid areas, necrosis, and hemorrhage.
Microscopy:
- Borderline: Complex papillary fronds with hierarchical branching, lined by pseudostratified columnar cells; NO stromal invasion
- Malignant (high-grade): Marked nuclear atypia, brisk mitoses, stromal invasion, gland formation and solid areas
- Psammoma bodies (concentric calcification rings) - characteristic but not exclusive to serous tumors
Endometrioid Tumors
- Represent 6-8% of epithelial tumors
- Associated with endometriosis (Sampson's theory, 1925)
- Histology: markedly complex glandular pattern resembling proliferative endometrium; confluent back-to-back glands
- 15-20% are synchronous with endometrial carcinoma - if both are well-differentiated with superficial endometrial invasion, these are considered independent primaries (75-80% 5-year survival vs. 30-40% for metastases)
Mucinous Tumors
- Lined by mucin-secreting epithelium resembling GI or endocervical epithelium
- Often very large, multiloculated cysts
- Pseudomyxoma peritonei - accumulation of gelatinous mucinous material in the abdominal cavity; most commonly from appendiceal mucinous neoplasms, rarely from primary ovarian mucinous tumors
Clear Cell Carcinoma
- Patterns: tubulocystic, papillary, reticular, solid
- Cells have abundant clear/vacuolated cytoplasm; "hobnail cells" project nuclei apically
- Almost invariably high-grade nuclei
- Strongly associated with endometriosis; histologically identical to clear cell carcinoma of DES-exposed uteri
Borderline Tumors (Low Malignant Potential)
- Show increased cell proliferation but lack stromal invasion (this is the defining criterion separating borderline from invasive)
- Occur predominantly in premenopausal women (ages 30-50)
- Very good prognosis
- Extraovarian implants may occur; invasive implants (analogous to low-grade serous carcinoma) have higher risk of progression and can cause intestinal obstruction from fibrosis
7. Germ Cell Tumors (15-20% of all ovarian tumors)
Found principally in children and young adults. Bear molecular similarity to testicular germ cell tumors.
| Tumor | Key Features | Tumor Marker |
|---|---|---|
| Mature (dermoid) cyst/teratoma | Most common GCT; unilocular cyst with hair, sebaceous material, teeth; bilateral in 10-15%; ~1% malignant transformation (usually SCC) | None |
| Immature teratoma | Malignant; contains immature neural elements | AFP |
| Dysgerminoma | Least differentiated GCT; bilateral in 10-15%; highly radiosensitive and chemo-sensitive; ~90% survival with complete resection | LDH |
| Yolk sac tumor (endodermal sinus) | Schiller-Duval bodies on histology | AFP |
| Choriocarcinoma | Trophoblastic differentiation | β-hCG |
| Monodermal teratoma | e.g., struma ovarii (thyroid tissue) | - |
8. Sex Cord-Stromal Tumors (~8%)
Arise from the stromal elements (granulosa cells, theca cells, Sertoli cells, Leydig cells). Many are hormonally active.
| Tumor | Hormone | Clinical Effect |
|---|---|---|
| Granulosa cell tumor | Estrogen | Abnormal uterine bleeding, endometrial hyperplasia/carcinoma, precocious puberty (in children) |
| Thecoma-fibroma | Estrogen (thecoma) | Meigs' syndrome (fibroma + ascites + pleural effusion) |
| Sertoli-Leydig (androblastoma) | Androgens (testosterone) | Virilization, elevated serum testosterone |
| Gonadoblastoma | - | In patients with dysgenetic gonads/Y chromosome |
Sex cord tumors are associated with Peutz-Jeghers syndrome.
9. Clinical Course & Presentation
Symptoms (Notoriously Vague and Late)
- Abdominal distension and/or pain
- Change in appetite, early satiety
- Weight gain and increased girth (ascites)
- Urinary frequency/obstruction
- Over half present to non-gynecological specialties first with GI disturbance, shortness of breath, or change in bowel habit from metastatic disease
Physical Examination
- Pelvic mass (often detected late)
- Ascites
- Pelvic mass + ascites = ovarian cancer until proven otherwise (but consider Meigs' syndrome - benign fibroma with ascites and pleural effusion)
10. Spread & Metastasis
Ovarian cancer spreads primarily by three routes:
1. Direct Peritoneal Seeding (Most Common Route)
- Malignant cells shed from the tumor surface into the peritoneal cavity
- Implant throughout the peritoneum: undersurface of the right hemidiaphragm, omentum, paracolic gutters, bowel serosa, bladder reflection, cul-de-sac
- Omental caking - characteristic matted omental metastasis
- Facilitated by MUC16 (CA-125) binding to mesothelin on peritoneal cells
2. Lymphatic Spread
- To pelvic and para-aortic lymph nodes
- Less common initially but present in advanced disease
3. Hematogenous Spread
- Late; to liver parenchyma, lungs (Stage IV)
- Pleural effusion also common in advanced disease
FIGO Staging
| Stage | Description |
|---|---|
| I | Growth limited to the ovaries |
| II | Involves one or both ovaries with pelvic extension (uterus, bladder, sigmoid, rectum) |
| III | Peritoneal implants outside the pelvis and/or retroperitoneal lymph nodes (pelvic/para-aortic) |
| IV | Distant metastases (liver parenchyma, pleural effusion with positive cytology, lungs) |
~70% of patients present at Stage III or IV, explaining the poor overall survival.
11. Complications
- Intestinal obstruction - from peritoneal/omental metastases and adhesions (especially borderline tumors with invasive implants); a major cause of death
- Malignant ascites - massive fluid accumulation, abdominal discomfort, dyspnea
- Pleural effusion - from diaphragmatic involvement or pleural seeding
- Hydronephrosis / ureteral obstruction - from retroperitoneal disease
- Ovarian torsion - complication of large benign/malignant ovarian masses
- Tumor rupture - peritoneal contamination, upstages disease
- Hormonal effects - endometrial hyperplasia/carcinoma (from estrogen-secreting granulosa cell tumors); virilization (Sertoli-Leydig tumors); precocious puberty (granulosa cell tumors in children)
- Paraneoplastic syndromes - e.g., inflammatory limbic encephalitis (associated with mature teratomas)
- Pseudomyxoma peritonei - gelatinous ascites from mucinous tumors
12. Investigations
- Ultrasound (transvaginal) - first-line; characterizes morphology (IOTA criteria)
- CA-125 - elevated in 50% of Stage I and >90% of advanced serous disease; non-specific (also elevated in endometriosis, PID, other cancers); normal cut-off 35 U/mL
- CT/MRI - staging; assesses peritoneal disease, lymphadenopathy, distant spread
- Tumor markers by age/type:
- AFP + β-hCG + LDH: women <40 to exclude germ cell tumors
- Inhibin: granulosa cell tumor marker
- CA-19-9, CEA: for mucinous tumors
- Risk of Malignancy Index (RMI) = menopausal status × ultrasound score × CA-125 level
13. Management Overview
Surgery
- Cytoreductive (debulking) surgery via midline laparotomy is the cornerstone
- Includes: peritoneal washings, infracolic omentectomy, pelvic/para-aortic lymphadenectomy, bilateral salpingo-oophorectomy + total abdominal hysterectomy, biopsy of suspicious lesions
- Appendicectomy for mucinous tumors
- Goal: no residual disease (optimal cytoreduction)
- Fertility-sparing (unilateral oophorectomy) allowed for Stage IA/IB low-grade or borderline tumors
Chemotherapy
- Platinum-based (carboplatin/paclitaxel) combination: standard first-line for advanced disease
- BRCA1/2-mutated tumors respond to PARP inhibitors (olaparib, niraparib, rucaparib)
Prevention
- Oral contraceptives: 50% risk reduction with >5 years of use; 70% reduction in women with 2+ children who used OCPs >5 years
- Prophylactic bilateral salpingo-oophorectomy for BRCA1/2 carriers (ideally before age 40 after childbearing complete)
- Note: prophylactic salpingo-oophorectomy does not completely eliminate risk - peritoneal carcinoma can still occur in 2-3% of cases
Quick Reference Summary Table
| Feature | Epithelial | Germ Cell | Sex Cord-Stromal |
|---|---|---|---|
| Frequency | 65-70% | 15-20% | ~8% |
| Age | Postmenopausal | Children/young adults | Any |
| Most common malignant | High-grade serous Ca | Dysgerminoma | Granulosa cell tumor |
| Key markers | CA-125 | AFP, β-hCG, LDH | Inhibin, testosterone |
| Key genetics | BRCA1/2, TP53 | - | - |
| Spread pattern | Peritoneal seeding | Lymphatic > peritoneal | Local |
Sources: Berek & Novak's Gynecology, pp. 2303-2380; Harrison's Principles of Internal Medicine 22E, pp. 748-757; Robbins Pathologic Basis of Disease 10E, pp. 3347-3385; Bailey & Love's Short Practice of Surgery 28E, pp. 3310-3440
This is a shared conversation. Sign in to Orris to start your own chat.