Why in Heat Stroke there is Low BP and High Heart Rate
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
I now have everything needed for a thorough, well-sourced answer. Here is the full explanation:
Why Heat Stroke Causes Low BP (Hypotension) and High Heart Rate (Tachycardia)
The cardiovascular changes in heat stroke are driven by three interconnected mechanisms working simultaneously:
1. Massive Peripheral (Cutaneous) Vasodilation
The body's primary strategy to cool itself is to shunt large volumes of blood toward the skin, where heat can radiate to the environment. This causes marked generalized vasodilation with peripheral pooling of blood and a decreased effective circulating blood volume - even if total blood volume hasn't actually dropped yet.
"The hyperthermia is accompanied by marked generalized vasodilation, with peripheral pooling of blood and a decreased effective circulating blood volume."
- Robbins, Cotran & Kumar Pathologic Basis of Disease
This vasodilation dramatically lowers systemic vascular resistance (SVR), which is a primary determinant of blood pressure:
BP = Cardiac Output × SVR
When SVR collapses, blood pressure falls, no matter how hard the heart tries to compensate.
From Medical Physiology (Boron & Boulpaep):
"Excessive cutaneous vasodilation can lead to a fall in arterial pressure and therefore to a decrease in brain perfusion."
2. Dehydration and Volume Depletion
Before thermoregulation fails completely, the body produces enormous amounts of sweat. This causes:
- Loss of intravascular fluid volume
- Reduced venous return to the heart (preload falls)
- Less blood available to fill the ventricles, so stroke volume drops
- Blood pressure falls further
Harrison's Principles (22e, 2025) directly states:
"The hypotension that is initially common among patients with heat-stroke results from both dehydration and high-output cardiac failure caused by peripheral vasodilation."
3. Tachycardia - the Compensatory Response
The heart detects the drop in blood pressure (via baroreceptors in the aortic arch and carotid sinus) and responds by increasing heart rate. This is a reflex sympathetic activation designed to maintain cardiac output:
Cardiac Output = Heart Rate × Stroke Volume
Since stroke volume is low (due to reduced venous return), the heart compensates by increasing rate. However, despite this tachycardia, the cardiac output often remains inadequate because:
- Tachycardia shortens diastolic filling time, limiting stroke volume further
- High temperatures directly impair myocardial contractility
- Right-sided heart failure can develop due to the volume overload from peripheral pooling
This is why Harrison's describes it as a "high-output cardiac failure" state - the heart is beating fast but cannot maintain adequate perfusion because the vascular resistance has collapsed.
4. Direct Myocardial Damage (Late Stage)
Braunwald's Heart Disease adds another layer:
"ECG abnormalities are common in heat stroke; pulmonary edema and transient right and/or left ventricular dysfunction may occur, along with hypotension and circulatory collapse. Sinus tachycardia is invariably present."
High temperatures (>41°C) directly damage myocardial muscle fibers, causing necrosis, subendocardial hemorrhages, and ventricular dysfunction - worsening the already failing hemodynamics.
Summary Diagram of the Mechanism
High ambient temperature
↓
Hypothalamus triggers thermoregulation
↓
Massive cutaneous vasodilation + profuse sweating
↓ ↓
Low SVR Volume depletion (dehydration)
↓ ↓
└─────────→ ↓ Venous return (preload) ←─────┘
↓
↓ Stroke Volume
↓
Baroreceptor reflex activated
↓
↑ Heart Rate (tachycardia) ← sympathetic drive
↓
Still → ↓ Blood Pressure (hypotension)
(because SVR collapse dominates)
↓
High-output cardiac failure
Clinical Note
This hemodynamic picture is called a "hyperdynamic circulation" in early heat stroke (high heart rate, high cardiac index, low vascular resistance). In late or severe heat stroke, as myocardial damage accumulates, it transitions to low-output failure with falling cardiac index - the most dangerous phase.
Importantly, treatment with norepinephrine is relatively contraindicated in heat stroke because its alpha-adrenergic vasoconstriction would shut down cutaneous blood flow and impede cooling - the exact opposite of what's needed.
Sources:
- Harrison's Principles of Internal Medicine, 22e, p. 3819
- Robbins, Cotran & Kumar - Pathologic Basis of Disease
- Braunwald's Heart Disease, p. 272
- Medical Physiology (Boron & Boulpaep)
- Tintinalli's Emergency Medicine, A Comprehensive Study
- Miller's Anesthesia, 10e
Exertional heat stroke
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive textbook content. Here is a full, well-organized breakdown of Exertional Heat Stroke:
Exertional Heat Stroke (EHS)
Definition
EHS is a life-threatening emergency characterized by:
- Core body temperature >40°C (>104°F)
- Profound central nervous system (CNS) dysfunction (confusion, ataxia, coma, seizures)
- Occurring during or immediately after vigorous physical exertion
It is distinguished from classic (non-exertional) heat stroke primarily by the patient population and by distinct biochemical and organ-damage profiles.
Who Gets It?
| Feature | Exertional HS | Classic HS |
|---|---|---|
| Age | 15-55 years (young, healthy) | Very young or elderly |
| Health baseline | Usually healthy | Chronic illness |
| Trigger | Exercise in heat | Passive heat exposure |
| Sweating | Often present (wet skin) | Anhidrosis (dry skin) |
| Onset | Rapid (hours) | Gradual (days) |
| Lactic acidosis | Prominent | Less common |
| Rhabdomyolysis | Common and severe | Mild/rare |
| Renal failure | Common | Uncommon |
| DIC | Prominent | Less common |
| Hypoglycemia | Yes | No (hyperglycemia) |
| Hyperphosphatemia, hypocalcemia | Yes | No |
Goldman-Cecil Medicine, Table 95-2
Pathophysiology
EHS follows a cascade triggered by the combination of endogenous metabolic heat from exercising muscle + exogenous environmental heat:
Step 1 - Heat Stress Inputs
- Physical exercise generates massive metabolic heat
- High ambient temperature and humidity prevent dissipation
- Heavy clothing, equipment, lack of air movement compound the load
Step 2 - Physiological Strain
- Cardiovascular system is challenged: blood must simultaneously supply working muscles AND perfuse the skin for cooling
- Blood pressure regulation fails as peripheral vasodilation overwhelms cardiac reserve
- Tissue hyperthermia, ischemia, and oxidative/nitrosative stress develop
Step 3 - Pathophysiology (the gut-endotoxemia axis)
A key mechanism unique to EHS:
- Gut permeability increases - splanchnic blood flow is diverted to working muscle and skin, making the gut ischemic
- Intestinal barrier breaks down → endotoxemia (bacterial LPS enters blood)
- This triggers an exaggerated acute-phase response
- Leads to Systemic Inflammatory Response Syndrome (SIRS)
- SIRS drives coagulopathy → DIC
- Then necrosis/apoptosis of cells across multiple organs
Goldman-Cecil Medicine
Three Clinical Phases of Severe EHS
-
Hyperthermic-neurologic acute phase: Elevated tissue temperature → GI dysfunction + CNS dysfunction (confusion, ataxia, seizure, coma)
-
Hematologic-enzymatic phase: Mild-to-severe DIC + elevated CK and aminotransferases (liver/muscle damage)
-
Late renal-hepatic phase: Diffuse end-organ failure (AKI, hepatic failure, ARDS)
Clinical Features
Vital Signs
- Core temperature >40°C (must be measured rectally - oral/axillary/tympanic are unreliable in EHS)
- Tachycardia, widened pulse pressure, arrhythmia
- Hypotension
- Tachypnea
CNS (most important diagnostic feature)
- Inability to continue exercise, disorientation, emotional lability
- Ataxia, altered gait (cerebellar sensitivity to heat)
- Confusion, delirium, behavioral changes, aggression
- Seizures (common, especially during cooling)
- Coma
Skin
- Profuse sweating (unlike classic HS where skin is dry) - absence of sweating is NOT required
- Pallor
GI
- Nausea, vomiting, diarrhea
Musculoskeletal
- Muscle flaccidity, cramps
- Rhabdomyolysis (muscle breakdown)
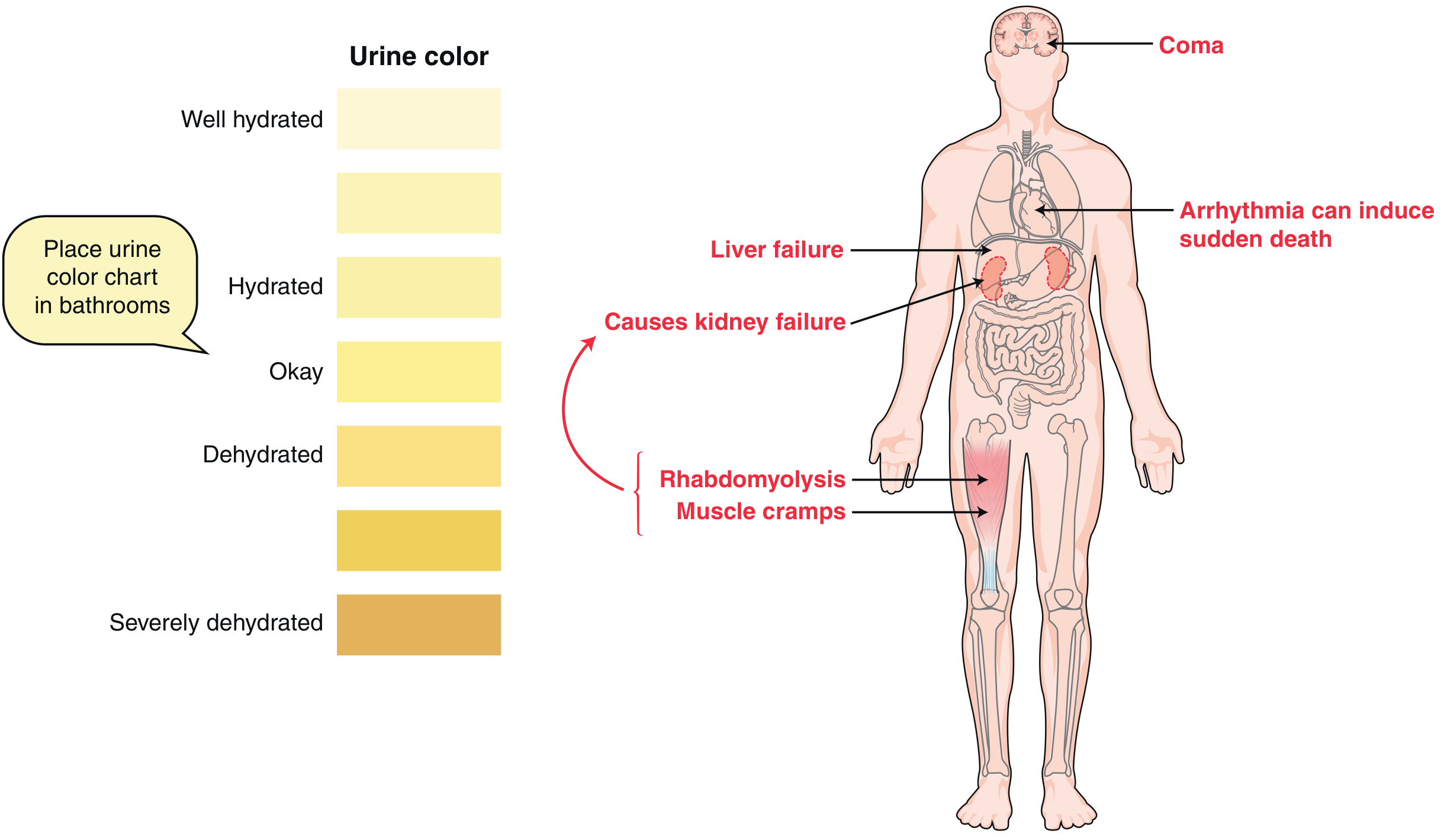
Urine
- Oliguria; dark/brown urine (myoglobinuria from rhabdomyolysis)
Laboratory Findings
| Lab | Finding in EHS |
|---|---|
| CK | Markedly elevated (rhabdomyolysis) |
| Creatinine / BUN | Elevated (AKI) |
| AST / ALT | Elevated (liver injury) |
| Electrolytes | Hyperphosphatemia, hypocalcemia, hypokalemia |
| Blood glucose | Hypoglycemia (contrast with classic HS) |
| ABG | Metabolic acidosis + lactic acidosis + respiratory alkalosis |
| PT/PTT, D-dimer, fibrinogen | Coagulopathy, DIC |
| Urinalysis | Myoglobinuria (tea-colored urine) |
| paCO₂ | Often <20 mmHg (hyperventilation) |
Miller's Anesthesia 10e; Goldman-Cecil Medicine
Treatment
Golden Rule: Cool First, Transport Second
Every minute of delay in cooling worsens outcome. Field cooling before transport saves lives.
1. Immediate Cooling (highest priority)
Target: Core temperature <38.8°C (102°F)
| Method | Notes |
|---|---|
| Ice water/cold water immersion | Most effective for EHS - gold standard in young athletes |
| Cold water dousing + skin massage | Highly effective, more practical |
| Evaporative cooling (wet skin + fans) | Good but less effective than immersion |
| Ice packs to groin, axillae, neck | Adjunct |
| Cold IV saline (~4°C) | Simultaneous volume + cooling |
| Gastric/colonic/bladder lavage with cold saline | Invasive, for refractory cases |
| Intravascular cooling catheters | Most invasive, last resort |
- Cooling rate of ≥0.155°C/min is the target
- Stop cooling at 39°C to avoid overcooling/hypothermia
- Cooling causes peripheral vasoconstriction, which helps redirect blood to the heart - a beneficial side effect
2. Airway
- Endotracheal intubation if unconscious or altered airway reflexes
- Avoid depolarizing agents (succinylcholine) - risk of hyperkalemia from rhabdomyolysis
3. IV Fluid Resuscitation
- EHS patients require far more aggressive isotonic crystalloid (normal saline) than classic HS
- Monitor urine output closely
- If rhabdomyolysis + myoglobinuria: maintain urine flow to protect kidneys
4. Seizure Management
- Lorazepam 1-2 mg IV (safe - low hepatotoxicity)
- Avoid: chlorpromazine (lowers seizure threshold, anticholinergic, worsens hypotension)
5. Cardiovascular Support
- Dopamine or dobutamine if cardiac output remains depressed despite adequate CVP
- Avoid norepinephrine - alpha-adrenergic vasoconstriction impedes skin cooling
- Cardiac arrhythmias during hyperthermia usually resolve spontaneously with cooling; antiarrhythmics rarely needed
6. Monitoring for Complications
Serial labs every few hours:
- ECG monitoring for arrhythmia
- Watch for hyperkalemia (from rhabdomyolysis)
- DIC monitoring: PT/PTT, fibrinogen, platelets, d-dimer
- Liver and renal function
- Glucose (hypoglycemia common)
What NOT to Use
- Antipyretics (NSAIDs, aspirin, acetaminophen) - completely ineffective; aspirin worsens coagulopathy; acetaminophen is hepatotoxic in this setting
- Dantrolene - effective in malignant hyperthermia but not heat stroke
- Anticholinergic drugs (including atropine) - inhibit sweating
Complications
| System | Complication |
|---|---|
| CNS | Cerebellar atrophy, persistent ataxia, dysarthria |
| Cardiac | Arrhythmias, myocardial necrosis, sudden death |
| Renal | Acute kidney injury (from rhabdomyolysis + hypoperfusion) |
| Liver | Acute hepatic failure |
| Lung | ARDS, pulmonary infarction, pneumonitis |
| Hematologic | DIC, uncontrolled hemorrhage |
| Muscle | Rhabdomyolysis |
Prognosis
- EHS mortality: 3-5% (much better than classic HS, because patients are young and healthy with rapid recognition)
- Classic HS: up to 60% die before reaching hospital; ICU mortality 10-65%
- 10-28% mortality at 1-2 years post-treatment
- Persistent neurologic deficits (ataxia, cerebellar signs) in a significant proportion
Miller's Anesthesia, 10e
Key Teaching Point: EHS = young, exercising, sweating, hot + confused. The sweating does NOT exclude the diagnosis. Rectal temperature is the only reliable measure. Cool immediately, everywhere, by any means available.
Sources:
- Goldman-Cecil Medicine, International Edition - Chapter 95
- Miller's Anesthesia, 10e
- Miller's Review of Orthopaedics, 9th Ed
- Harrison's Principles of Internal Medicine, 22e
- Tintinalli's Emergency Medicine
This is a shared conversation. Sign in to Orris to start your own chat.