CROHNS DISEASES
Reading File
Finding Sources
Searching PubMed
"Crohn's disease"[MeSH Terms] AND "management"[MeSH Terms]
Searching Images
Crohn's disease pathology histology colonoscopy
Reading File
Reading File
Reading File
Searching PubMed
"Crohn disease"[MeSH Terms] AND "biological therapy"[MeSH Terms]
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
I now have comprehensive information to provide a thorough, well-structured answer on Crohn's disease. Let me compose it.
Crohn's Disease
Overview
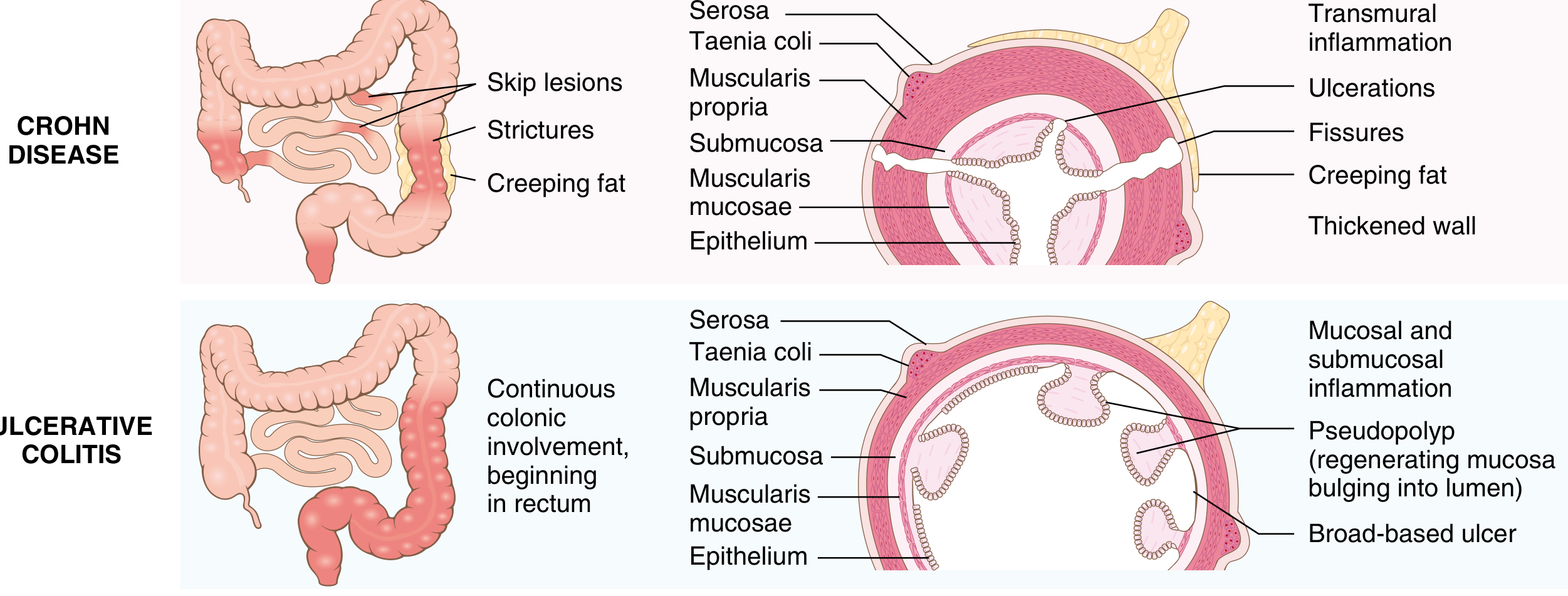
Crohn's disease (CD) is a chronic, relapsing transmural inflammatory bowel disease (IBD) that can affect any segment of the gastrointestinal tract from mouth to anus. Together with ulcerative colitis (UC), it forms the two main forms of idiopathic IBD. Unlike UC, which is confined to the colonic mucosa, CD is characterized by transmural, patchy (skip lesion) inflammation that can occur anywhere along the GI tract.
Epidemiology
- Bimodal age of onset: peak in the 2nd–3rd decade, with a smaller peak in the 5th–6th decade
- Most common in North America, northern Europe, and Australia; incidence rising in Africa, South America, and Asia
- Higher prevalence among Ashkenazi Jewish populations (3–5× general population)
- Equal sex distribution; slight female predominance in some series
- The hygiene hypothesis links rising incidence to improved food storage, decreased microbial exposure, and altered gut microbiome composition, predisposing to dysregulated mucosal immunity
— Robbins, Cotran & Kumar Pathologic Basis of Disease
Etiology and Pathogenesis
CD results from the intersection of genetic susceptibility, environmental triggers, and dysregulated immune-microbiome interactions:
Genetics
-
200 IBD-associated risk alleles identified, but account for <20% of CD risk
- NOD2 (intracellular sensor of muramyl dipeptide — a bacterial cell wall component) is the strongest genetic risk factor; 3 major NOD2 risk alleles are found in ~30% of CD patients vs. 5% of healthy individuals
- CD is polygenic; accumulated polymorphisms impact susceptibility (disease location, stricturing vs. penetrating behavior)
- PTPN22 and NOD2 variants increase CD risk but are protective in UC
- Rare monogenic early-onset IBD involves mutations in IL-10 and IL-10 receptor subunits
Environmental Factors
- Smoking doubles the risk of CD (opposite effect in UC)
- NSAIDs, appendectomy, dietary factors (processed foods, emulsifiers), and alterations in gut microbiome (dysbiosis) are implicated
- Stress, enteric infections can trigger relapses
Immunobiology
- CD4+ Th1 and Th17 cells drive inflammation; key cytokines: TNF-α, IL-12, IL-23, IFN-γ, IL-17
- Defective mucosal barrier and impaired clearance of bacteria allow luminal antigens to perpetuate immune activation
- Dysfunctional regulatory T-cell responses fail to suppress the inflammatory cascade
— Robbins, Cotran & Kumar; Sleisenger and Fordtran's GI and Liver Disease
Pathology (Gross and Microscopic)
Common Sites
- Terminal ileum ± cecum: most common (~40% small intestine only)
- Small intestine + colon: ~30%
- Colon only: ~30%
- Rarely: esophagus, stomach, duodenum
Gross Features
| Feature | Description |
|---|---|
| Skip lesions | Multiple separate diseased areas with intervening normal mucosa |
| Aphthous ulcers | Earliest lesion; may coalesce into serpentine ulcers |
| Cobblestone mucosa | Edematous mucosa between deep ulcers/fissures |
| Creeping fat | Mesenteric fat encasing the serosal surface |
| Strictures | From transmural fibrosis and hypertrophy of muscularis propria |
| Fistulae | Deep fissures extending into adjacent organs/skin |
| Wall thickening | Transmural edema, fibrosis, muscular hypertrophy |
Microscopic Features
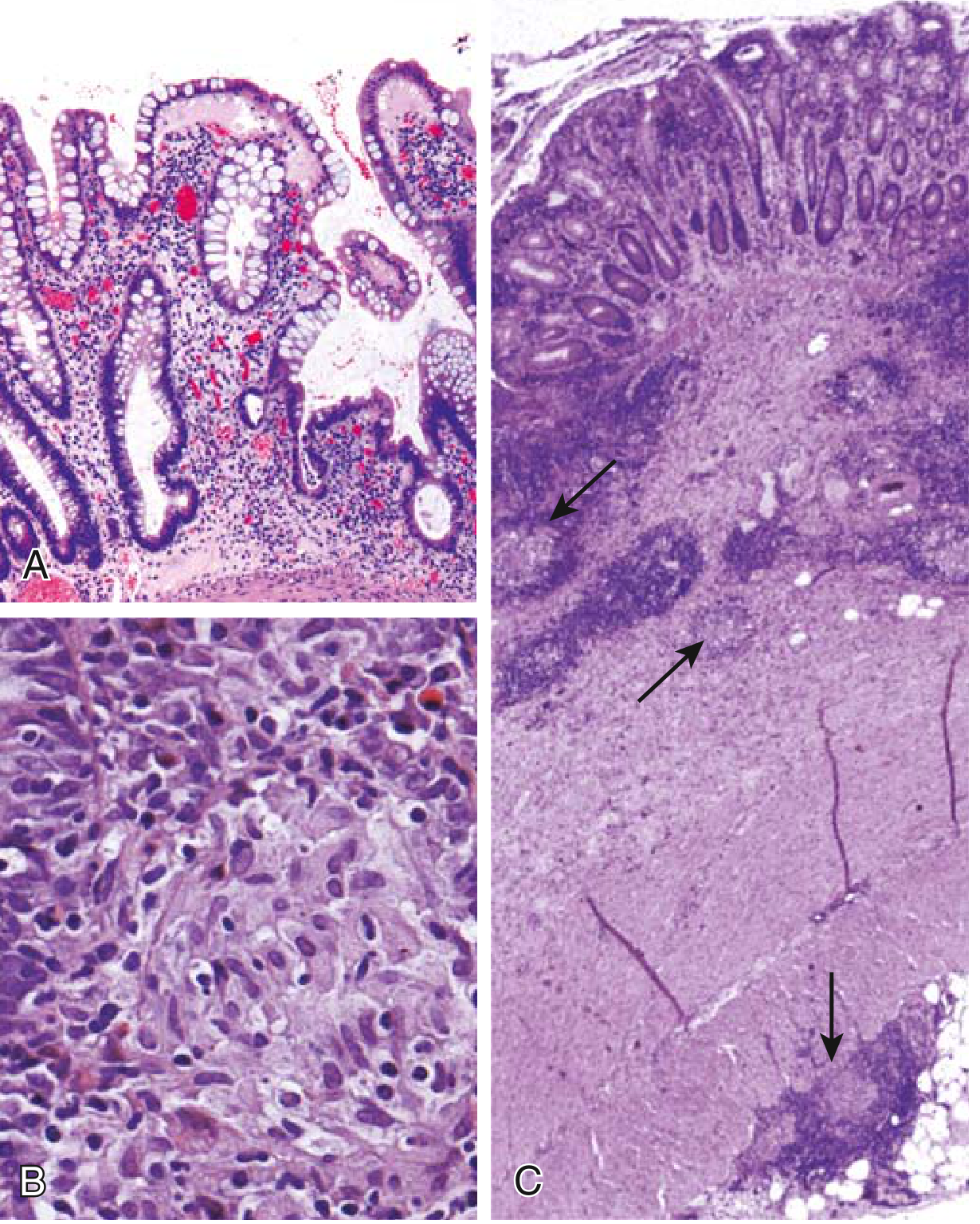
- Transmural inflammation (entire bowel wall) — key distinction from UC
- Neutrophil infiltration of crypts → crypt abscesses
- Crypt architectural distortion (branching, irregular)
- Noncaseating granulomas (~35% of cases) — hallmark, though absence does not exclude diagnosis
- Pyloric gland metaplasia and Paneth cell metaplasia
- Ulcers: deep, knife-like (vs. UC's broad-based, superficial ulcers)
— Robbins & Kumar Basic Pathology; Robbins, Cotran & Kumar Pathologic Basis of Disease
CD vs. UC: Key Distinctions
| Feature | Crohn Disease | Ulcerative Colitis |
|---|---|---|
| Bowel region | Ileum ± colon (any GI) | Colon only |
| Distribution | Skip lesions | Diffuse, continuous |
| Wall | Thick (transmural) | Normal thickness |
| Inflammation | Transmural | Mucosal/submucosal only |
| Ulcers | Deep, knife-like | Superficial, broad-based |
| Granulomas | Yes (~35%) | No |
| Fistulae/sinuses | Yes | No |
| Strictures | Common | Rare |
| Fibrosis | Marked | Mild to none |
| Toxic megacolon | No | Yes |
| Perianal disease | Yes (colonic involvement) | No |
| Fat/vitamin malabsorption | Yes | No |
| Recurrence after surgery | Common | No |
Clinical Features
Intestinal Manifestations
- Symptoms: intermittent diarrhea (may be non-bloody), crampy abdominal pain (especially RLQ), fever, weight loss, anorexia, malaise
- ~20% present acutely with RLQ pain/fever mimicking appendicitis
- Disease behavior (Montreal classification):
- B1 (Inflammatory/non-stricturing, non-penetrating): most common early
- B2 (Stricturing): fibrosis → partial or complete bowel obstruction
- B3 (Penetrating/Fistulizing): fistulae (enterocutaneous, enterovesical, rectovaginal), abscesses, free perforation
Perianal Disease
- Perianal fistulae, skin tags, anal fissures, abscesses
- Especially prominent in colonic CD
Extraintestinal Manifestations (~30% of patients)
- Joints: migratory peripheral arthritis, sacroiliitis, ankylosing spondylitis
- Skin: erythema nodosum, pyoderma gangrenosum
- Eyes: uveitis, episcleritis
- Liver/biliary: primary sclerosing cholangitis (more common in UC but occurs in CD)
- Thromboembolic: DVT/PE due to hypercoagulable state
- Nutrition: malabsorption → B12 deficiency (terminal ileal disease), fat-soluble vitamin deficiency, iron-deficiency anemia
Diagnosis
Endoscopy
- Ileocolonoscopy with biopsies is the gold standard
- Findings: aphthous ulcers, cobblestoning, skip lesions, deep fissuring ulcers
- Upper GI endoscopy if upper GI symptoms
Radiology
- MR enterography (MRE): modality of choice for small bowel evaluation; shows mural thickening, hyperenhancement, the "comb sign" (engorged peri-enteric vasculature), fistulae, abscesses
- CT enterography: faster, accessible, good for complications
- Capsule endoscopy: mucosal evaluation of small bowel (avoid if strictures suspected)
Biomarkers
- C-reactive protein (CRP): correlates with disease activity; elevated in active disease
- Fecal calprotectin: pooled sensitivity 88%, specificity 67% for active CD endoscopy; useful for monitoring
- Fecal lactoferrin: another neutrophil marker of intestinal inflammation
- Complete blood count: anemia, leukocytosis
- Serology: ASCA (anti-Saccharomyces cerevisiae antibody) positive in ~50–60% CD; pANCA typically negative
Disease Activity
- Crohn Disease Activity Index (CDAI): Remission = CDAI <150; clinical response = decrease ≥100 points
- Mucosal healing is now a therapeutic target beyond symptom control
Treatment
Mild to Moderate CD
| Drug | Use |
|---|---|
| Budesonide (enteric-coated, 9 mg/day) | Distal ileal/right colonic disease; ~70% response at 8 weeks |
| Sulfasalazine (3–6 g/day) | Ileocolonic/colonic CD; not effective for small bowel disease alone |
| Metronidazole / Ciprofloxacin | Perianal fistulae (primary inductive therapy); not for luminal CD |
Moderate to Severe CD
| Drug Class | Examples | Notes |
|---|---|---|
| Corticosteroids | Prednisone, methylprednisolone | Induction only; not maintenance; ~50–70% response |
| Immunomodulators | Azathioprine, 6-mercaptopurine, methotrexate | Maintenance; 50–70% remission rate |
| Anti-TNF biologics | Infliximab, adalimumab, certolizumab pegol | Induction + maintenance; fistula healing |
| Anti-integrin | Vedolizumab | Gut-selective; good safety profile |
| Anti-IL-12/23 | Ustekinumab | Effective for induction and maintenance |
| Anti-IL-23 | Risankizumab | Newer; approved for moderate-severe CD |
| JAK inhibitors | Upadacitinib | Small molecule; emerging role |
- Combination therapy: Infliximab + azathioprine > either alone (SONIC trial); early combined immunosuppression preferred in high-risk disease
- ~50% of patients relapse within 1 year of discontinuing infliximab + azathioprine
- Avoid long-term corticosteroids (lymphoma risk with thiopurines + anti-TNF combination must be weighed)
Perianal/Fistulizing Disease
- Antibiotics (metronidazole/ciprofloxacin) for acute management
- Infliximab: fistula healing rates up to 60% in RCTs
- Azathioprine/cyclosporine: ~30% success
- Surgical drainage of abscesses prior to biologic therapy
Surgery
- ~75% of CD patients require surgery within 20 years of symptom onset
- Surgery rates at 1, 5, 10 years: 16%, 33%, 47% (population-based meta-analysis)
- Guiding principle: preservation of intestinal length (wide margins do not reduce recurrence)
- Most common procedure: ileocecal resection with primary anastomosis (often laparoscopic)
- Bowel-sparing: strictureplasty for scattered strictures
- Indications: intra-abdominal abscess, medically intractable fistula, fibrotic stricture with obstruction, cancer, growth failure in children, glucocorticoid-refractory disease
- Surgery rates have declined significantly over 6 decades with better medical therapy
— Goldman-Cecil Medicine; Sleisenger and Fordtran's GI and Liver Disease; Mulholland and Greenfield's Surgery
Complications
| Complication | Notes |
|---|---|
| Bowel obstruction (SBO) | Acute (active inflammation) or chronic (fibrotic stricture) |
| Fistulae | Enteroenteric, enterovesical, rectovaginal, enterocutaneous |
| Intra-abdominal abscess | Percutaneous drainage preferred; IV antibiotics |
| Malabsorption & nutritional deficiency | B12, D, K, iron, zinc; short bowel syndrome post-resection |
| Colorectal cancer | Elevated risk with longstanding colonic involvement (less than UC) |
| Perianal disease | Fistulae, abscesses, strictures |
| Osteoporosis | From malabsorption and corticosteroid use |
Monitoring & Targets
- Treat-to-target: goal is mucosal healing (endoscopic remission) + symptom resolution
- Monitor CRP, fecal calprotectin, and periodic ileocolonoscopy
- Screen for lymphoma, skin cancers with long-term immunosuppressant use
- Colorectal cancer surveillance colonoscopy for long-standing colonic disease
Recent Evidence
A 2024 systematic review and meta-analysis (PMID 37506265, Inflamm Bowel Dis) confirmed that early biologic treatment significantly decreases the risk of surgery in Crohn's disease — reinforcing the shift toward early aggressive therapy for high-risk patients.
Sources: Robbins & Kumar Basic Pathology; Robbins, Cotran & Kumar Pathologic Basis of Disease; Sleisenger and Fordtran's Gastrointestinal and Liver Disease; Goldman-Cecil Medicine; Mulholland and Greenfield's Surgery; Law et al., Inflamm Bowel Dis 2024 [PMID 37506265]
EXPLAIN SURGICAL ANATOMY OF INGUINAL CANAL AND ETIOPATHOLOGY AND CLASSIFICATION OF HERNIA
Reading File
Finding Sources
Finding Sources
Searching Images
inguinal canal surgical anatomy hernia
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Finding Sources
Finding Sources
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
This is a shared conversation. Sign in to Orris to start your own chat.