Septic arthritis
Reading File
Finding Sources
Searching PubMed
"septic arthritis"[MeSH Terms] AND management
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Excellent. I now have comprehensive content to deliver a thorough answer. Let me compile everything:
Septic Arthritis
Definition and Overview
Septic arthritis (infectious arthritis) is a joint space infection - an orthopedic emergency with potentially devastating consequences. Even with prompt, appropriate management, it leads to permanent loss of function in 25-50% of patients. Incidence in native joints is 2-10/100,000 in the general population, rising to 30-70/100,000 in patients with rheumatoid arthritis.
- Rosen's Emergency Medicine, p. 2730
Pathophysiology
The synovium lacks a basement membrane, which allows bacteria to spread easily into the joint space. Infection reaches the joint by:
- Hematogenous seeding - most common route; bacteremia seeds the synovial membrane
- Direct inoculation - trauma, joint aspiration, or surgery
- Contiguous spread - from adjacent osteomyelitis or soft tissue infection
The synovial membrane extends beyond the epiphysis and attaches to the metaphysis in the knee, hip, and shoulder - this anatomic fact explains why septic arthritis and osteomyelitis can coexist or trigger each other.
Once bacteria enter the joint, neutrophils, synovial cells, and bacteria release proteolytic enzymes causing rapid cartilage and subchondral bone destruction. Delay in diagnosis leads to permanent disability.
- Rosen's Emergency Medicine, p. 2730; Grainger & Allison's Diagnostic Radiology, p. 1198
Microbiology
The most common organism overall is Staphylococcus aureus, including MRSA strains.
| Population | Likely Organisms |
|---|---|
| Adolescents / young sexually active adults | Neisseria gonorrhoeae (most common in this group) |
| Adults >40 yrs / chronic illness | S. aureus, Streptococcus |
| Children | S. aureus, Streptococcus, E. coli |
| Neonates | Staphylococci, Enterobacteriaceae, Group B Strep, N. gonorrhoeae |
| IV drug users | S. aureus, Pseudomonas aeruginosa (sternoclavicular joint) |
| Sickle cell disease | Salmonella (though common organisms still predominate) |
| Post-operative / prosthetic joint | S. aureus, S. epidermidis, Enterobacteriaceae, Pseudomonas |
| Immunocompromised | Fungal, mycobacterial organisms |
Note: H. influenzae was previously a leading pediatric cause but has been nearly eliminated by the conjugate vaccine.
- Roberts & Hedges' Clinical Procedures in Emergency Medicine, p. 1263
Risk Factors
- Diabetes mellitus
- Rheumatoid arthritis (highest risk of any systemic disease)
- Recent joint surgery or prosthetic joint
- IV drug use
- Immunosuppression / corticosteroid use
- Prior joint disease (osteoarthritis, gout)
- Infective endocarditis
- Skin infections / cellulitis near a joint
Clinical Features
Joints Affected
- Typically monoarticular (<20% polyarticular in adults; <10% in children)
- Knee: most common in adults (~50%), most easily aspirated
- Hip: ~25% in adults (referred pain to thigh/knee may mislead)
- Shoulder: ~15%
- IV drug users: sternoclavicular, sacroiliac joints
- S. aureus has a particular predilection for sternoclavicular, sacroiliac, and symphysis pubis joints
Symptoms and Signs
-
Acute onset joint pain, worsened with any range of motion
-
Joint swelling, erythema, warmth - cardinal signs of inflammation
-
Fever: present in >80% of children but only ~40% of adults
-
Constitutional symptoms (malaise, myalgias, anorexia) are inconsistently reported
-
Joint held in position of least tension (slight flexion)
-
Pseudoparalysis in neonates/infants - may mimic neurologic disorders
-
Children who cannot bear weight or move a joint spontaneously must be investigated urgently
-
Immunosuppressed patients (especially on steroids) may have minimal joint pain despite active infection
-
Rosen's Emergency Medicine, p. 2730-2731
Differential Diagnosis
| Condition | Key Differentiating Features |
|---|---|
| Crystal arthritis (gout/pseudogout) | Can be clinically indistinguishable - synovial fluid analysis required |
| Transient/toxic synovitis | Children 3mo-6yr; self-limited; normal WBC/ESR; no fever; less pain with passive motion |
| Reactive arthritis | Migratory polyarthritis; sterile joint fluid; WBC usually <50,000/mm³; history of preceding infection |
| Juvenile rheumatoid arthritis | More gradual onset; polyarticular pattern |
| Hemarthrosis | Trauma or hemophilia history |
| Osteomyelitis | Metaphyseal infection; adjacent joint effusion; may coexist |
| Lyme arthritis | Endemic area; less systemic toxicity; check serology |
| Rheumatic fever | Migratory polyarthritis; can mimic gonococcal bacteremia |
| Legg-Calvé-Perthes / SCFE | Hip in children; not as acutely disabling |
- Rosen's Emergency Medicine, p. 2731-2732
Diagnosis
Lab Tests
- WBC (serum): elevated >10,000/mm³ in only ~50% of cases - not reliable alone
- ESR: elevated in ~90% of cases; sensitivity 98% at cutoff ≥10 mm/hr, 96% at >30 mm/hr
- CRP: sensitivity 92% at threshold >20 mg/L
- Procalcitonin: >0.5 ng/mL suggestive but nonspecific and not always available
- Blood cultures: two sets - positive in only a minority; still important to obtain
Arthrocentesis and Synovial Fluid Analysis
Joint aspiration is mandatory - it is the cornerstone of diagnosis. Aseptic technique is essential. Inoculate blood culture bottles immediately after aspiration to maximize yield.
| Test | Finding in Septic Arthritis |
|---|---|
| WBC (synovial) | Usually >50,000/mm³ (range 25,000-150,000+); PMN predominance (>90%) |
| Gram stain | Positive in only 29-55% of cases - negative does NOT exclude infection |
| Culture | Most definitive test; tissue cultures from OR superior to fluid |
| Glucose | Low synovial glucose (<40 mg/dL, or >40 mg/dL below serum) |
| Crystal analysis | May coexist with crystals (gout + infection possible) |
| Lactate | Elevated in bacterial arthritis |
A WBC >50,000/mm³ with >90% PMNs is highly suspicious for septic arthritis; however, crystal arthropathy can also produce counts in this range. Culture remains the gold standard.
- Rosen's Emergency Medicine, p. 2733-2734; Roberts & Hedges', p. 1262-1263
Imaging
Plain radiographs: non-diagnostic early in disease; may show joint effusion. Later findings include joint space narrowing, subchondral bone plate lysis, erosions, and adjacent bone destruction - by which point, significant damage has already occurred.
Ultrasound: detects joint effusion and synovial thickening, especially useful for superficial or small joints; can guide aspiration.
CT: useful if MRI contraindicated; reveals joint effusions, bone erosions, synovial enhancement; good for fluoroscopy-guided aspiration of deep joints.
MRI with gadolinium: the preferred modality.
-
Sensitivity 100%, specificity 77% for septic arthritis
-
Can detect changes as early as 24 hours after infection onset
-
Especially valuable for deep joints (shoulder, hip) and fibrocartilaginous joints
-
Shows joint effusion, synovial thickening/enhancement, bone marrow edema, adjacent soft tissue involvement
-
Grainger & Allison's Diagnostic Radiology, p. 1198-1199
Management
Antibiotics
Start empirical IV antibiotics immediately after arthrocentesis - do not delay for culture results.
| Scenario | Empirical Antibiotic Choice |
|---|---|
| Most adults (likely S. aureus) | IV anti-staphylococcal agent: nafcillin/oxacillin or vancomycin if MRSA risk |
| MRSA risk (healthcare-associated, prior MRSA, IV drug use) | Vancomycin IV |
| Gonococcal arthritis (sexually active young adult) | Ceftriaxone IV; often responds well clinically |
| Gram-negative / immunocompromised | Add anti-pseudomonal beta-lactam (piperacillin-tazobactam, cefepime) |
| Children | Age-appropriate coverage targeting S. aureus, Streptococcus |
Tailor antibiotics once culture and sensitivity results return. Duration is typically 2-4 weeks IV followed by oral step-down (total 4-6 weeks for native joints; longer for prosthetic joints).
Joint Drainage
Joint drainage is essential alongside antibiotics. Options:
- Serial arthrocentesis - repeated needle aspiration (daily or every other day) is adequate for many native joints, especially the knee
- Arthroscopic lavage and debridement - preferred for hip, shoulder, and cases where needle aspiration fails to control infection
- Open surgical drainage - for neonates (always), hip infections in children, joints difficult to access, and cases failing less invasive approaches
Disposition
All patients with suspected or confirmed septic arthritis should be admitted for IV antibiotics and orthopaedic consultation. Empirical IV antibiotics after aspiration should begin in the ED.
Prosthetic joint infections require orthopaedic surgery input and typically involve implant removal or exchange.
- Rosen's Emergency Medicine, p. 2734-2735; Roberts & Hedges', p. 1263
Prognosis
- 50-75% of patients recover completely with full painless range of motion
- ~1/3 develop complications: decreased mobility, ankylosis, chronic infection, or death from overwhelming sepsis
- Outcomes are best when treatment begins within 1 week of symptom onset
Poor prognostic factors:
-
Delay in diagnosis and treatment
-
Underlying rheumatoid arthritis
-
Polyarticular septic arthritis
-
Positive blood cultures (implies more severe bacteremia)
-
Extremes of age (infants and elderly)
-
Hip joint involvement in children (risk of avascular necrosis of femoral head)
-
Rosen's Emergency Medicine, p. 2735
Special Situations
Gonococcal Arthritis
N. gonorrhoeae is the leading cause of septic arthritis in sexually active young adults. It often presents as a disseminated gonococcal infection (DGI) with two patterns:
- Bacteremic phase: migratory polyarthralgia/polyarthritis, tenosynovitis, pustular skin lesions
- Joint-localized phase: frank septic monoarthritis (classically knee, wrist, ankle)
Culture of synovial fluid is often negative in gonorrhea; clinical response to ceftriaxone is often the only diagnostic criterion. Cultures of genitourinary, pharyngeal, and rectal sites improve yield.
Prosthetic Joint Infection
Classified by timing:
- Early (<3 months post-op): S. aureus, gram-negatives
- Delayed (3-24 months): coagulase-negative staphylococci
- Late (>24 months): hematogenous seeding, any organism
Management requires orthopaedic surgery; often involves two-stage revision with implant removal.
Pediatric Hip: Kocher Criteria
Used to differentiate septic arthritis from transient synovitis in children:
- Fever >38.5°C
- Non-weight-bearing
- ESR >40 mm/hr
- WBC >12,000/mm³
Probability of septic arthritis: 0 factors = <0.2%; 4 factors = ~99.6%
Sources: Goldman-Cecil Medicine (27th ed.) | Rosen's Emergency Medicine (9th ed.) | Roberts & Hedges' Clinical Procedures in Emergency Medicine (7th ed.) | Grainger & Allison's Diagnostic Radiology (7th ed.)
Spetic arthritis in elbow joint
Reading File
Finding Sources
Finding Sources
Searching PubMed
"septic arthritis"[MeSH Terms] AND "elbow"[MeSH Terms]
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Loading Image
I now have comprehensive, elbow-specific content from multiple authoritative sources. Here is the full answer:
Septic Arthritis of the Elbow
Overview
The elbow is an uncommon but clinically significant site for septic arthritis. It accounts for roughly 7-15% of all septic arthritis cases, ranking behind the knee, hip, and shoulder in frequency. Despite being less common than knee or hip septic arthritis, it carries the same risk of rapid cartilage destruction and permanent loss of function if not treated promptly.
A key anatomical point: the elbow joint is a compound hinge joint involving the humeroulnar, humeroradial, and proximal radioulnar articulations - all sharing a single synovial cavity. Infection in one compartment quickly spreads to all three.
- Campbell's Operative Orthopaedics, 15th Ed, 2026, p. 1036
Causes and Mechanisms
Routes of infection
- Hematogenous spread - most common; bacteremia seeds the synovial membrane
- Direct inoculation - trauma (e.g., laceration over the elbow), animal bites, iatrogenic (post-injection or post-arthroscopy)
- Contiguous spread - from adjacent olecranon bursitis, osteomyelitis of the distal humerus or proximal ulna/radius
Clinical pearl: A laceration or puncture wound over the elbow is a classic precipitating factor - the joint lies superficially and is easily inoculated.
Microbiology
S. aureus (including MRSA) is the most common causative organism. The elbow is also listed among the large joints commonly infected by N. gonorrhoeae in sexually active adults.
| Group | Likely Organism |
|---|---|
| General adult population | S. aureus (MSSA or MRSA) |
| Sexually active young adults | N. gonorrhoeae |
| Post-traumatic / post-injection | S. aureus, skin flora, gram-negatives |
| IV drug users | S. aureus, Pseudomonas |
| Immunocompromised | Unusual organisms, fungi, mycobacteria |
| Post-operative / prosthetic elbow | S. epidermidis, S. aureus, Enterobacteriaceae |
- Medical Microbiology 9e, p. 2330; Roberts & Hedges', p. 1263
Clinical Features
Presentation
- Acute-onset elbow pain exacerbated by any movement, especially extension
- Swelling, erythema, warmth over the joint
- The elbow is typically held in semiflexion - the position that maximizes joint volume and minimizes capsular tension
- Fever (present in >80% of children, ~40% of adults)
- Systemic symptoms: malaise, rigors
Critical clinical sign - distinguishing from olecranon bursitis
This is one of the most important distinctions at the elbow:
"Unlike septic arthritis, in which the elbow must be kept in semiflexion, the elbow may be brought into full passive extension in septic bursitis."
- Goldman-Cecil Medicine, 27th Ed, p. 2777
| Feature | Septic Arthritis | Septic Olecranon Bursitis |
|---|---|---|
| Swelling location | Diffuse, periarticular | Localized to olecranon tip |
| Passive extension | Restricted and painful | Full and painless |
| Fever / systemic signs | Usually present | Less prominent |
| WBC in aspirate | >50,000/mm³ (joint) | Variable (bursal fluid) |
This distinction matters because the management differs - septic bursitis requires bursal drainage and antibiotics, while septic arthritis of the joint requires formal joint drainage.
Diagnosis
Laboratory
- Serum WBC: elevated in ~50% - not reliable alone
- ESR and CRP: elevated in ~90% of cases; most sensitive serum markers
- Blood cultures: two sets - positive in a minority but essential
- Procalcitonin: >0.5 ng/mL supports infection
Arthrocentesis and Synovial Fluid Analysis
Joint aspiration is mandatory. At the elbow, this is the key diagnostic and initial therapeutic step.
Aspiration Technique
The elbow is flexed at 90 degrees and the needle is inserted on the posterior aspect just lateral to the olecranon (Fig. 24.14 from Campbell's below). This is the standard approach used in clinical practice.
- Campbell's Operative Orthopaedics, 15th Ed, 2026
Alternative approaches (from Rheumatology, 2-Volume Set):
- Inferolateral approach: midpoint cleft between the olecranon tip and lateral epicondyle; needle inserted perpendicularly toward the center of the joint
- Lateral (radiocapitellar) approach: proximal to the radial head; needle passed perpendicular to skin between radius and capitellum
- If palpation-guided aspiration fails: ultrasound-guided aspiration from anterior or posterior recess
Synovial Fluid Interpretation
| Test | Septic Arthritis |
|---|---|
| WBC | Usually >50,000/mm³, often >100,000; >90% PMNs |
| Gram stain | Positive in only 29-55%; negative does NOT exclude infection |
| Culture | Definitive test; inoculate blood culture bottles immediately |
| Glucose | Low (<40 mg/dL or >40 mg/dL below serum) |
| Lactate | Elevated |
Imaging
- Plain radiographs: early infection shows only soft tissue swelling and possible joint effusion (posterior fat pad sign, anterior sail sign); later reveals joint space narrowing, subchondral erosions
- Ultrasound: identifies effusion, guides aspiration; can detect synovial thickening
- MRI with gadolinium: preferred modality; sensitivity 100%, specificity 77%; detects changes within 24 hours; shows extent of infection, adjacent osteomyelitis, and soft tissue involvement
- CT: useful if MRI contraindicated; shows effusion, bone erosions, guides aspiration of difficult joints
Staging - Gächter Classification
This arthroscopic staging system (commonly used for elbow and shoulder) guides the aggressiveness of intervention:
| Stage | Findings | Radiographic Changes |
|---|---|---|
| I | Fluid opacity, synovial redness, possible petechial bleeding | None |
| II | Severe inflammation, fibrinous deposition, frank pus | None |
| III | Synovial thickening, compartment formation | None |
| IV | Aggressive pannus, cartilage infiltration, subchondral osteolysis, bone erosions/cysts | Present |
Arthroscopic treatment is most effective in Stages I and II (ideally within 2 weeks of onset). Stage IV indicates advanced destruction with a poorer functional prognosis.
- Campbell's Operative Orthopaedics, 15th Ed, 2026, p. 1036
Management
Step 1: Antibiotics
Start empirical IV antibiotics immediately after joint aspiration - never delay antibiotics waiting for culture results.
| Clinical Scenario | Antibiotic Choice |
|---|---|
| Most adults (gram-positive cocci on Gram stain) | Vancomycin 15-20 mg/kg/dose every 8-12 hours IV (covers MRSA) |
| MSSA confirmed | Nafcillin or oxacillin IV (or cefazolin) |
| Gram-negative organisms / immunocompromised | Add anti-pseudomonal coverage: piperacillin-tazobactam or cefepime |
| Gonorrhea suspected (young adult, tenosynovitis, skin lesions) | Ceftriaxone 2g IV |
| Inconclusive Gram stain | Vancomycin + ceftriaxone |
Duration: typically 2-4 weeks IV followed by oral step-down, total 4-6 weeks for native joints.
Important: Intra-articular antibiotics have NO role in treatment of septic arthritis. IV antibiotics achieve excellent synovial fluid levels.
- Rosen's Emergency Medicine, 9th Ed
Step 2: Joint Drainage
This is where the elbow has specific surgical considerations. The elbow cannot be adequately drained by serial needle aspiration alone in most cases due to its anatomical complexity. Formal surgical drainage is frequently required.
Option A: Arthroscopic Lavage and Synovectomy (preferred in early-stage disease)
"Arthroscopic irrigation and synovectomy are safe and effective in the elbow, producing good functional results in immunocompetent patients with septic arthritis."
- Campbell's Operative Orthopaedics, 15th Ed, 2026, p. 1038
- Indicated for Gächter Stages I and II (ideally <2 weeks from onset)
- Allows thorough joint lavage and debridement with less surgical morbidity
- Motorized synovial resector used; drains placed through portal sites
- Permits early active mobilization, which is critical for elbow function
Option B: Open Surgical Drainage
Indicated when arthroscopy is not available, infection is advanced (Gächter Stage III-IV), or there is failure of less invasive management.
Approaches (Campbell's Operative Orthopaedics):
Medial drainage (Technique 24.19):
- Incision over the medial humeral epicondyle, extending 5 cm proximally and 2.5 cm distally
- Develop interval between triceps (posterior) and brachialis (anterior)
- Protect the ulnar nerve as it crosses the posterior medial epicondyle
- Elevate periosteum laterally and distally to expose the capsule
- Incise capsule, evacuate pus, irrigate copiously with saline
- Close loosely over drains
Lateral drainage (Technique 24.20):
- Incision over lateral humeral epicondyle
- Separate triceps (posteriorly) from extensor carpi radialis longus (anteriorly)
- Expose joint capsule (dissect close to bone to protect the radial nerve)
- Incise capsule, evacuate pus, irrigate with saline
- Close loosely over drains
- This incision also allows posterior compartment drainage by dissecting posteriorly on the humerus and elevating the triceps attachment
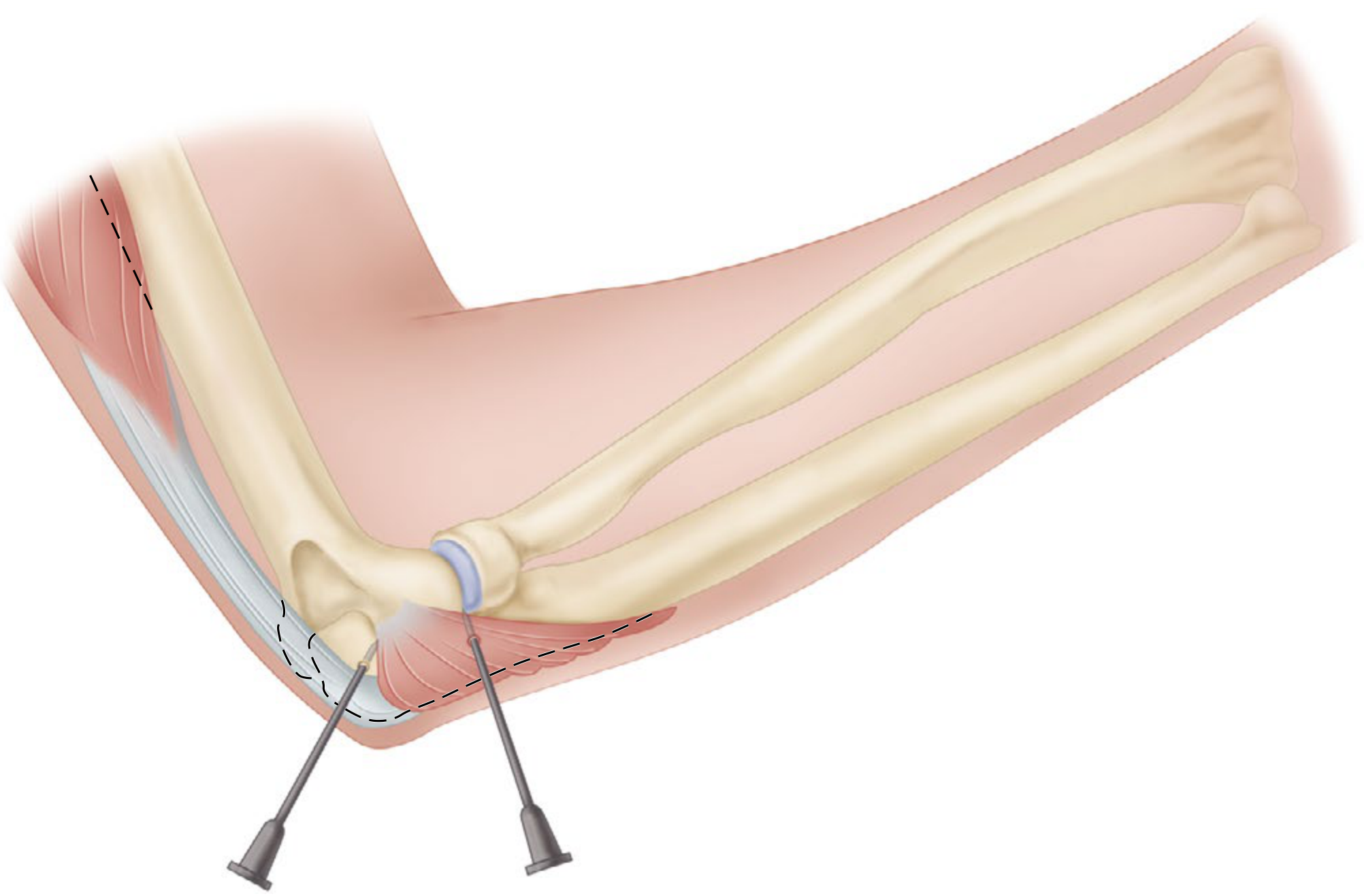
Posterior drainage (Technique 24.21):
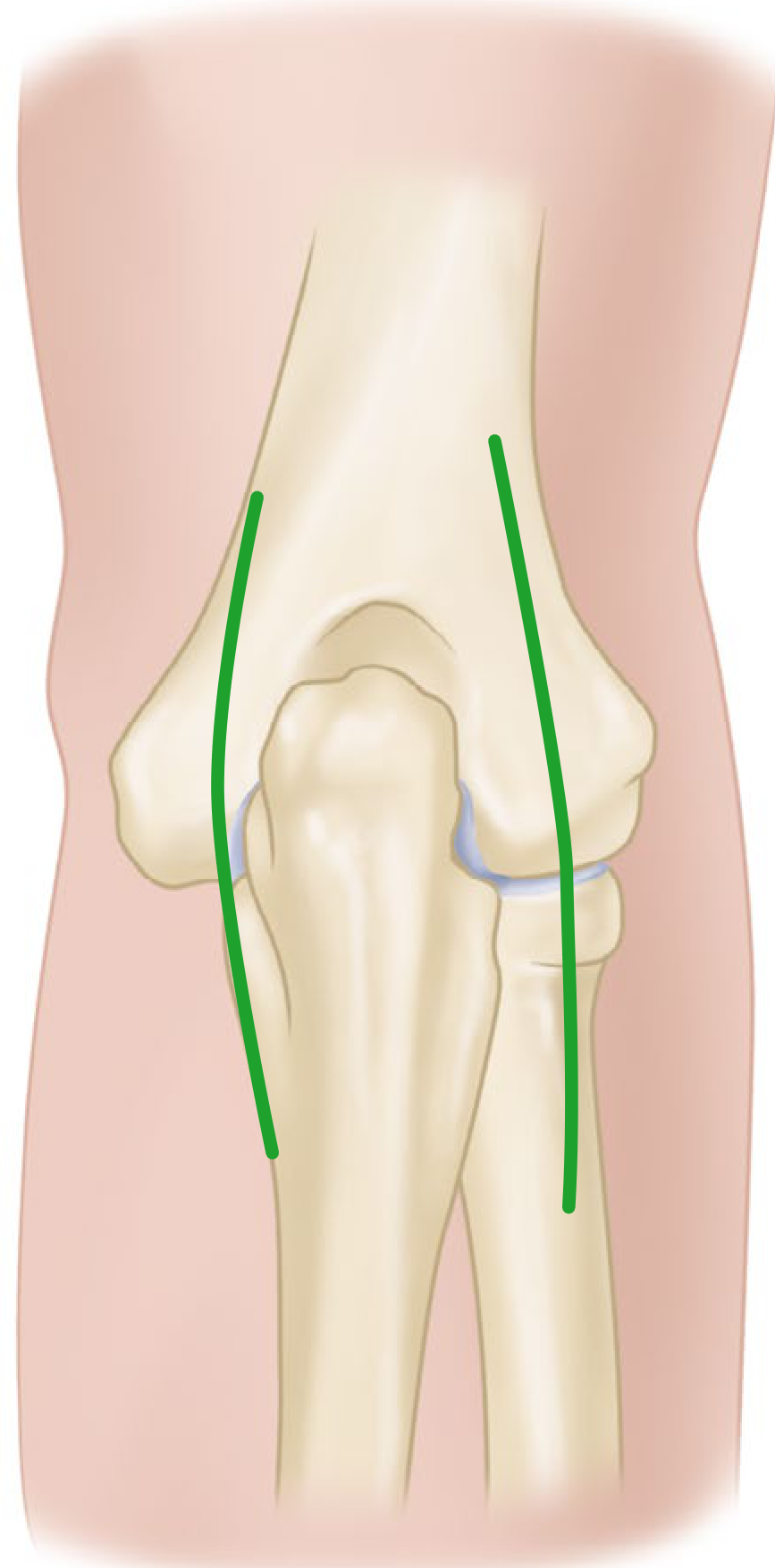 FIGURE 24.15 - Parallel longitudinal incisions on each side of the olecranon for posterior drainage. SEE TECHNIQUE 24.21.
FIGURE 24.15 - Parallel longitudinal incisions on each side of the olecranon for posterior drainage. SEE TECHNIQUE 24.21.
- Parallel longitudinal incisions on each side of the olecranon, extending 7.5 cm proximally
- Deepen through medial and lateral borders of the triceps aponeurosis into the posterior joint compartment
- Avoid the ulnar nerve crossing the posteromedial epicondyle
Postoperative care: Splint at 90 degrees with forearm in neutral rotation until wound heals. Then start active range-of-motion exercises early to prevent ankylosis - this is especially important at the elbow, which is highly prone to stiffness.
Step 3: Disposition and Monitoring
- Admit all patients for IV antibiotics and orthopaedic consultation
- Monitor ESR and CRP to track treatment response
- Orthopedic surgery consultation is mandatory
- Serial synovial fluid analysis guides duration of treatment
- Early active mobilization once infection is controlled
Complications
| Complication | Notes |
|---|---|
| Elbow ankylosis / stiffness | Most feared long-term complication; more common at elbow than other joints |
| Cartilage destruction | Irreversible; occurs within days if untreated |
| Adjacent osteomyelitis | Distal humerus, proximal radius or ulna |
| Ulnar neuropathy | Can result from inflammation or surgical intervention |
| Radial nerve injury | Risk during lateral surgical drainage |
| Septicemia / death | Rare but possible in untreated or immunocompromised patients |
| Prosthetic joint infection | If total elbow arthroplasty is present - requires specialist management including likely implant removal |
Special Consideration: Septic Elbow in IV Drug Users
Intravenous drug users have a particular predilection for sternoclavicular and sacroiliac joints, but the elbow is also affected more often in this population due to direct inoculation during injection. Pseudomonas aeruginosa must be empirically covered alongside S. aureus in this group.
Sources: Campbell's Operative Orthopaedics, 15th Ed 2026 | Goldman-Cecil Medicine, 27th Ed | Rosen's Emergency Medicine, 9th Ed | Rheumatology 2-Volume Set (Elsevier, 2022) | Medical Microbiology 9e
Clindamycin for septic arthritis
Finding Sources
Searching PubMed
"septic arthritis" AND clindamycin
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
I now have all the information needed for a thorough, well-sourced answer.
Clindamycin for Septic Arthritis
Summary of Role
Clindamycin occupies a specific and conditional role in septic arthritis. It is not a first-line empirical agent in most adults, but it is a well-established:
- Alternative to vancomycin for MRSA - when local MRSA clindamycin resistance is <10%
- Oral step-down agent after initial IV therapy for both MSSA and MRSA
- Option in beta-lactam allergy
- Pediatric first-line agent in community-acquired MRSA-prevalent settings
Mechanism and Pharmacology
Clindamycin is a lincosamide antibiotic that inhibits bacterial protein synthesis by binding to the 50S ribosomal subunit. It is bacteriostatic against most organisms at standard doses.
Synovial Penetration - Key Concept
A common misconception is that antibiotics penetrate joints poorly. The textbooks are clear on this:
"The synovial penetration of all intravenous antibiotics and most oral antimicrobials is sufficient and significantly better than for bone infections. Therefore the analogy by equating the septic joint with the poor penetration into infected bone is clinically incorrect."
- Rheumatology, 2-Volume Set (Elsevier, 2022), p. 1014
"Quinolones, cotrimoxazole, and basically all non-beta-lactam antibiotics are known for their good bioavailability in synovial tissues and/or adjacent bone."
- Rheumatology, 2-Volume Set (Elsevier, 2022)
This means clindamycin achieves adequate synovial fluid drug levels when given systemically - both IV and oral formulations - making the oral step-down strategy pharmacologically sound.
Key Pharmacokinetic Properties Relevant to Septic Arthritis
| Property | Detail |
|---|---|
| Synovial penetration | Excellent - sufficient for joint infections |
| Oral bioavailability | ~90% - makes oral step-down reliable |
| Spectrum | Gram-positive cocci (including MRSA if susceptible), anaerobes |
| Gram-negative coverage | None - do not use for gram-negative septic arthritis |
| Intra-articular administration | Contraindicated / no benefit - systemic levels are sufficient; intra-articular antibiotics add no value and may damage cartilage |
When Clindamycin is Used in Septic Arthritis
1. MRSA Septic Arthritis - Alternative to Vancomycin (IV)
Per IDSA guidelines (referenced in Red Book 2021 and Rosen's Emergency Medicine):
"Clindamycin 40 mg/kg/day q6-8h can be substituted for vancomycin if local S. aureus resistance to clindamycin is <10%."
- Rosen's Emergency Medicine, 9th Ed (citing IDSA MRSA guidelines)
Condition for use: The local/institutional MRSA clindamycin susceptibility rate must be >90% (i.e., resistance <10%). This threshold must be checked against your local antibiogram before prescribing.
| Scenario | Primary Choice | Clindamycin Role |
|---|---|---|
| MRSA - serious infection (adults) | Vancomycin IV | Alternative if susceptible and local resistance <10% |
| MRSA - less severe (skin, SSTIs, joint if stable) | Vancomycin or clindamycin | Co-equal option if susceptible |
| Community-acquired MRSA in children | Vancomycin or clindamycin | Well-established alternative |
- Red Book 2021, p. 1063; Rosen's Emergency Medicine, p. 3312
2. Oral Step-Down Therapy After IV Antibiotics (Both MSSA and MRSA)
This is arguably the most important and common role of clindamycin in septic arthritis. After 2-4 days of IV therapy (once the patient is clinically improving and tolerating oral medications), oral step-down is standard practice.
From Rheumatology 2-Volume Set (Table 111.2) - Targeted Antibiotic Therapy:
| Pathogen | IV Therapy (0-2 weeks) | Oral Step-Down Options (complete 3 weeks) |
|---|---|---|
| MSSA | Cefazolin 2g TID or Flucloxacillin 2g QID | Clindamycin 600 mg TID, or Co-trimoxazole 2-3x forte/day, or Doxycycline 100 mg BID |
| MRSA | Vancomycin (trough 15-20 mg/L) or Daptomycin 8-10 mg/kg OD | Clindamycin 600 mg TID (if susceptible), or Co-trimoxazole, or Doxycycline, or Fusidic acid + rifampin, or Linezolid |
| Streptococcus spp. | Penicillin 4 MU QID or Ceftriaxone 2g OD | Amoxicillin 1000 mg TID, or Clindamycin 600 mg TID, or Doxycycline |
Clindamycin oral dose for step-down: 600 mg three times daily (adults)
Note: Recent evidence supports short total antibiotic duration - a randomized trial found no difference in clinical remission, adverse events, or sequelae with 2 weeks vs. 4 weeks of antibiotics after surgical drainage of native joint septic arthritis.
- Rheumatology, 2-Volume Set, p. 1014
- Rheumatology, 2-Volume Set (Elsevier, 2022), p. 1014-1015
3. Pediatric Septic Arthritis - Established First-Line Alternative
In children, clindamycin plays a more prominent role in both IV and oral phases when MRSA is a concern.
Harriet Lane Handbook (Johns Hopkins, 23rd Ed) - Septic Arthritis:
- Children <5 years: Cefazolin or oxacillin + clindamycin (if concern for MRSA)
- Children >5 years: Cefazolin, or clindamycin if concern for MRSA
- For unstable/ill-appearing children: IV vancomycin preferred over clindamycin
Red Book 2021 - Systems-Based Treatment Table (Bone/Joint):
- For septic arthritis due to S. aureus: Cefazolin OR Oxacillin OR Nafcillin OR Clindamycin as listed treatment options
- Important caveat: Kingella kingae is not affected by clindamycin and is not reliably susceptible to oxacillin/nafcillin - relevant in children <5 years where Kingella is a common cause
Pediatric IV dose: Clindamycin 40 mg/kg/day divided q6-8h
- Harriet Lane Handbook, 23rd Ed, p. 601; Red Book 2021, p. 1405
4. Beta-Lactam Allergy
Clindamycin is an appropriate alternative for gram-positive septic arthritis (including MSSA and MRSA if susceptible) in patients with:
- Penicillin allergy
- Cephalosporin hypersensitivity
- Carbapenem allergy
It does not have cross-reactivity with beta-lactam antibiotics.
5. Mycoplasma / Ureaplasma Arthritis (Rare)
Clindamycin is listed as an alternative treatment (alongside fluoroquinolones) for Mycoplasma septic arthritis, with doxycycline as the first choice.
- Goldman-Cecil Medicine, 27th Ed
When Clindamycin Should NOT Be Used
| Situation | Reason |
|---|---|
| Gram-negative septic arthritis (Enterobacteriaceae, Pseudomonas) | No gram-negative coverage |
| N. gonorrhoeae arthritis | Ceftriaxone is drug of choice |
| Kingella kingae arthritis (children <5 yr) | Not effective against Kingella |
| MRSA with local clindamycin resistance >10% | Risk of treatment failure |
| Inducible clindamycin resistance (D-zone test positive) | Despite in vitro susceptibility, clinical failure may occur - check D-zone (double-disk diffusion) test |
| Intra-articular injection | No added benefit; potential cartilage toxicity |
The Inducible Resistance Problem (D-Zone Test)
This is a critical clinical consideration. Some MRSA (and MSSA) strains show:
- Erythromycin-resistant, clindamycin-susceptible phenotype on routine testing
- But carry the erm gene causing inducible clindamycin resistance (iMLSB)
- The D-zone test (double-disk diffusion) detects this - a "D-shaped" zone of inhibition around the clindamycin disk indicates inducible resistance
If the D-zone test is positive, clindamycin should NOT be used even if the isolate appears susceptible, because resistance will emerge during therapy.
Always request D-zone testing when considering clindamycin for MRSA or erythromycin-resistant MSSA.
Practical Summary
| Phase | Role | Dose (Adults) | Dose (Children) |
|---|---|---|---|
| Empirical IV | Alternative to vancomycin if MRSA risk and local resistance <10%; beta-lactam allergy | 600-900 mg IV q8h | 40 mg/kg/day IV q6-8h |
| Oral step-down | After clinical improvement, for both MSSA and MRSA (if susceptible) | 600 mg PO TID | 30-40 mg/kg/day PO q6-8h |
| Empirical in children | When MRSA is likely (community-acquired) in stable patients | - | 40 mg/kg/day IV/PO q6-8h |
Before using clindamycin:
- Check local MRSA clindamycin resistance rate (<10% threshold)
- Request D-zone test on the isolated organism
- Confirm organism is gram-positive (no gram-negative coverage)
- Confirm Kingella is not the pathogen (children <5 yr)
Sources: Rosen's Emergency Medicine, 9th Ed | Rheumatology 2-Volume Set (Elsevier, 2022) | Red Book 2021 (AAP) | Harriet Lane Handbook, 23rd Ed (Johns Hopkins) | Goldman-Cecil Medicine, 27th Ed
This is a shared conversation. Sign in to Orris to start your own chat.