I am a 1st year mbbs student
- Anatomy - bones, muscles, nerves, vessels, organ systems
- Physiology - how body systems function (cardiac, respiratory, renal, neuro, etc.)
- Biochemistry - metabolism, enzymes, molecular biology, genetics
- Histology - tissue types and microscopic anatomy
- Embryology - developmental biology
- Clinical correlations - connecting basic science to real diseases
I have a sentup test from Saturday
I will give you questions of different subject you give answers of about 5 marks
- Clear headings/points
- Key facts and definitions
- Diagrams described where relevant
- Concise but complete coverage
Firstly biochem
Acid base balance disorder
Acid-Base Balance Disorders
Normal Acid-Base Status
- Normal arterial pH = 7.35 - 7.45
- Regulated by the Henderson-Hasselbalch equation:
- pH = 6.1 + log([HCO3-] / 0.03 × PaCO2)
- Normal values: HCO3- = 24 mEq/L, PaCO2 = 40 mmHg
Classification of Acid-Base Disorders
| Disorder | Primary Change | pH | Compensation |
|---|---|---|---|
| Metabolic Acidosis | ↓ HCO3- | <7.35 | ↓ PaCO2 (hyperventilation) |
| Metabolic Alkalosis | ↑ HCO3- | >7.45 | ↑ PaCO2 (hypoventilation) |
| Respiratory Acidosis | ↑ PaCO2 | <7.35 | ↑ HCO3- (renal retention) |
| Respiratory Alkalosis | ↓ PaCO2 | >7.45 | ↓ HCO3- (renal excretion) |
1. Metabolic Acidosis
- Cause: Excessive acid production (e.g., diabetic ketoacidosis, lactic acidosis), loss of bicarbonate (diarrhea), or renal failure
- Features: Low pH, low HCO3-, compensatory hyperventilation (Kussmaul breathing)
2. Metabolic Alkalosis
- Cause: Vomiting (loss of HCl), excess alkali intake, diuretic use
- Features: High pH, high HCO3-, compensatory hypoventilation
3. Respiratory Acidosis
- Cause: Hypoventilation - COPD, respiratory failure, sedative overdose
- Features: Low pH, high PaCO2; kidneys retain HCO3- to compensate
4. Respiratory Alkalosis
- Cause: Hyperventilation - anxiety, fever, pulmonary embolism, high altitude
- Features: High pH, low PaCO2; kidneys excrete HCO3- to compensate
Key Points for Compensation
- Metabolic disorders → compensated by the lungs (change in CO2)
- Respiratory disorders → compensated by the kidneys (change in HCO3-)
- Compensation never fully corrects the pH - it only minimizes the change
- If compensation is excessive or insufficient, a mixed disorder is present
Mixed Disorders
Sources: Medical Physiology (Boron & Boulpaep); ROSEN's Emergency Medicine; Quick Compendium of Clinical Pathology
Any diagram?
Diagram 1 - Simple Acid-Base Disorder (Decision Tree)
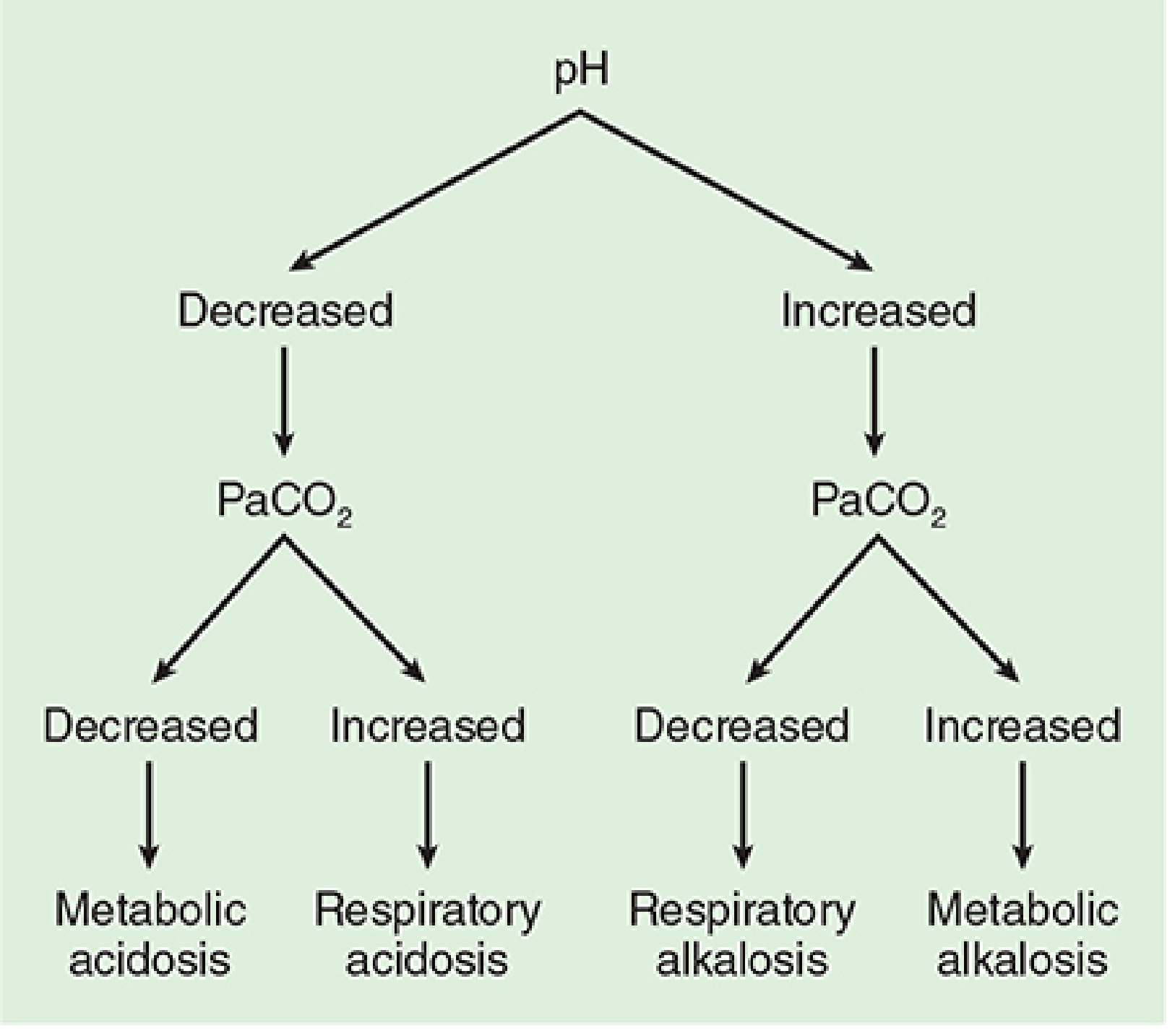
- pH ↓ + PaCO2 ↓ = Metabolic acidosis
- pH ↓ + PaCO2 ↑ = Respiratory acidosis
- pH ↑ + PaCO2 ↓ = Respiratory alkalosis
- pH ↑ + PaCO2 ↑ = Metabolic alkalosis
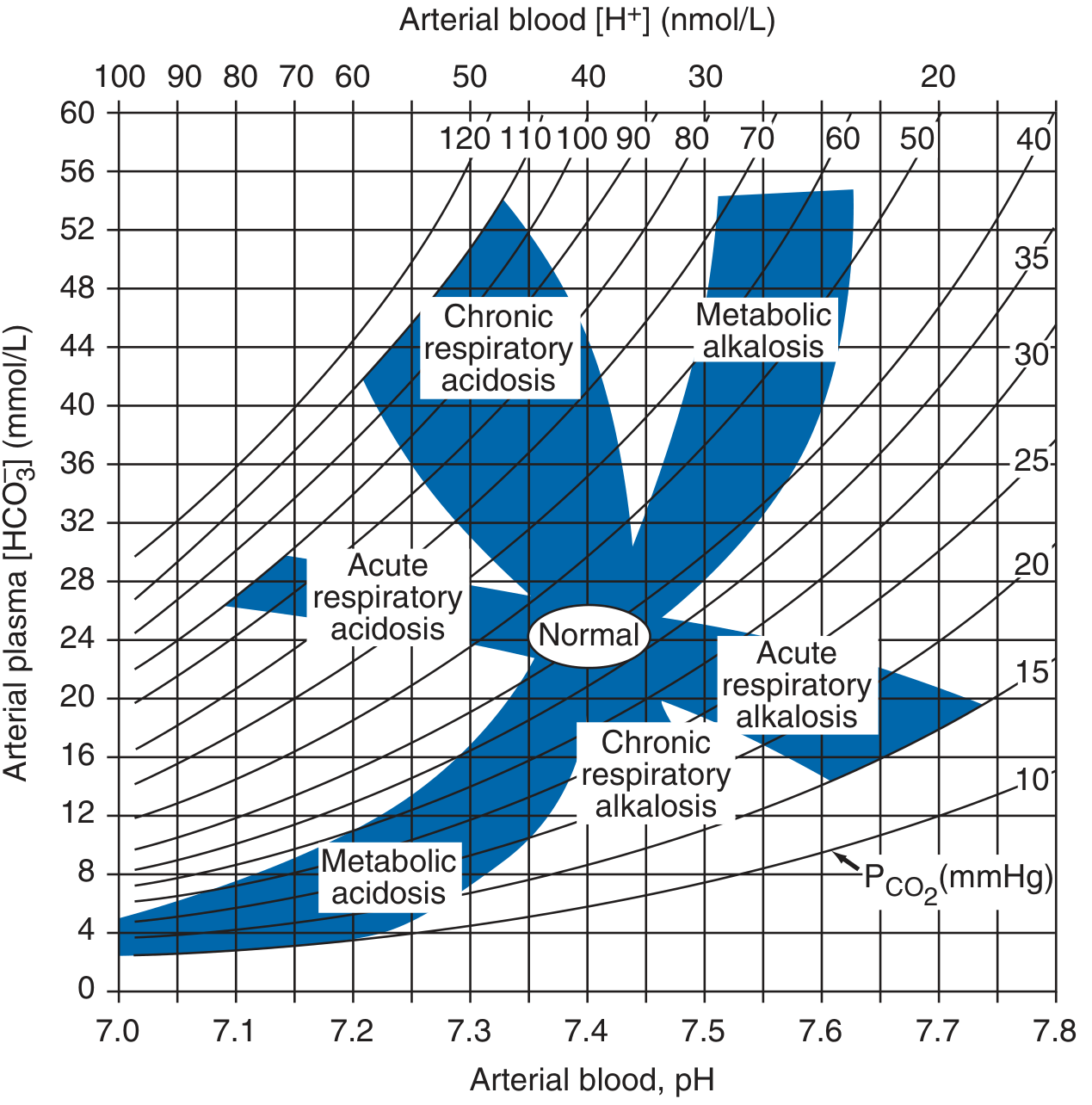
Diagram 2 - Acid-Base Nomogram (90% Confidence Bands)
Now anatomy give detail answer with diagram and clinical
Shoulder joint
Shoulder Joint (Glenohumeral Joint)
1. Type and Articulation
- Type: Ball-and-socket synovial joint - the most mobile joint in the body
- Articulation: Between the head of humerus (ball) and the glenoid cavity of scapula (socket)
- The glenoid cavity is shallow and small (covers only 1/3 of humeral head) - this allows wide movement but sacrifices stability
- The glenoid labrum (fibrocartilaginous rim) deepens the socket and improves congruity
2. Articular Capsule
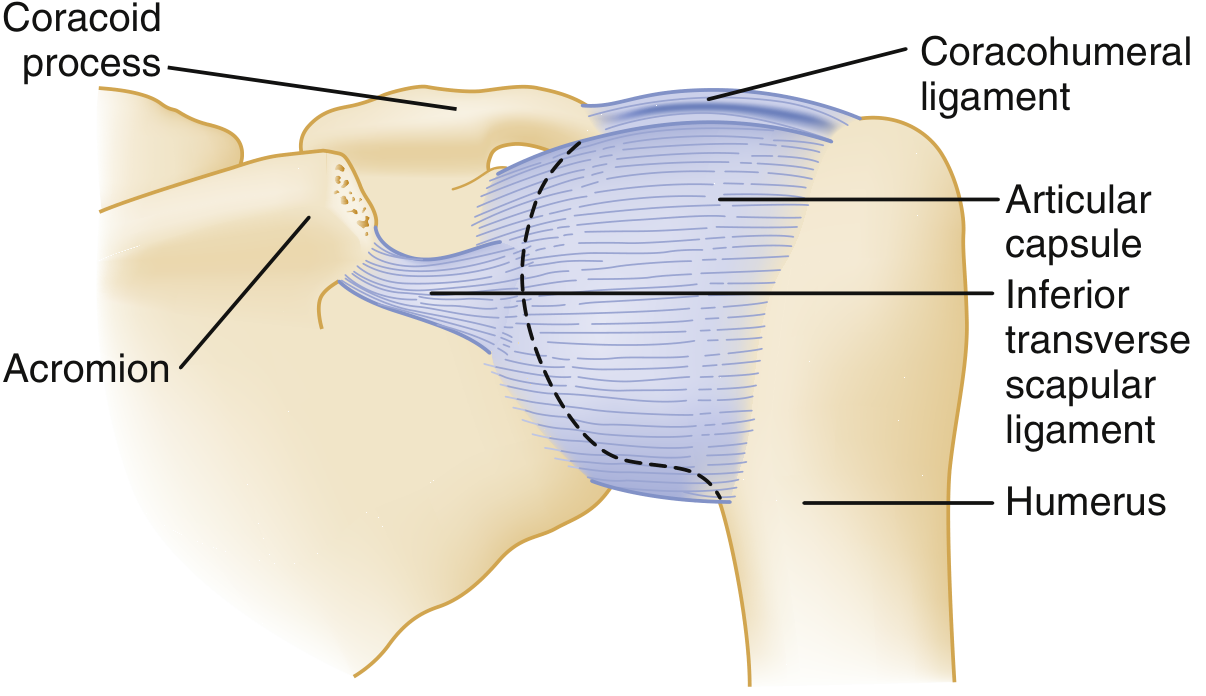
- The fibrous capsule is loose and redundant - especially inferiorly, allowing wide movement
- Attaches to the glenoid labrum medially and anatomical neck of humerus laterally
- Weak point: The inferior wall is the thinnest - site of most dislocations
- Two openings in the capsule:
- For the tendon of long head of biceps (superiorly)
- Communication with subscapular bursa (anteriorly)
3. Ligaments
| Ligament | Attachment | Function |
|---|---|---|
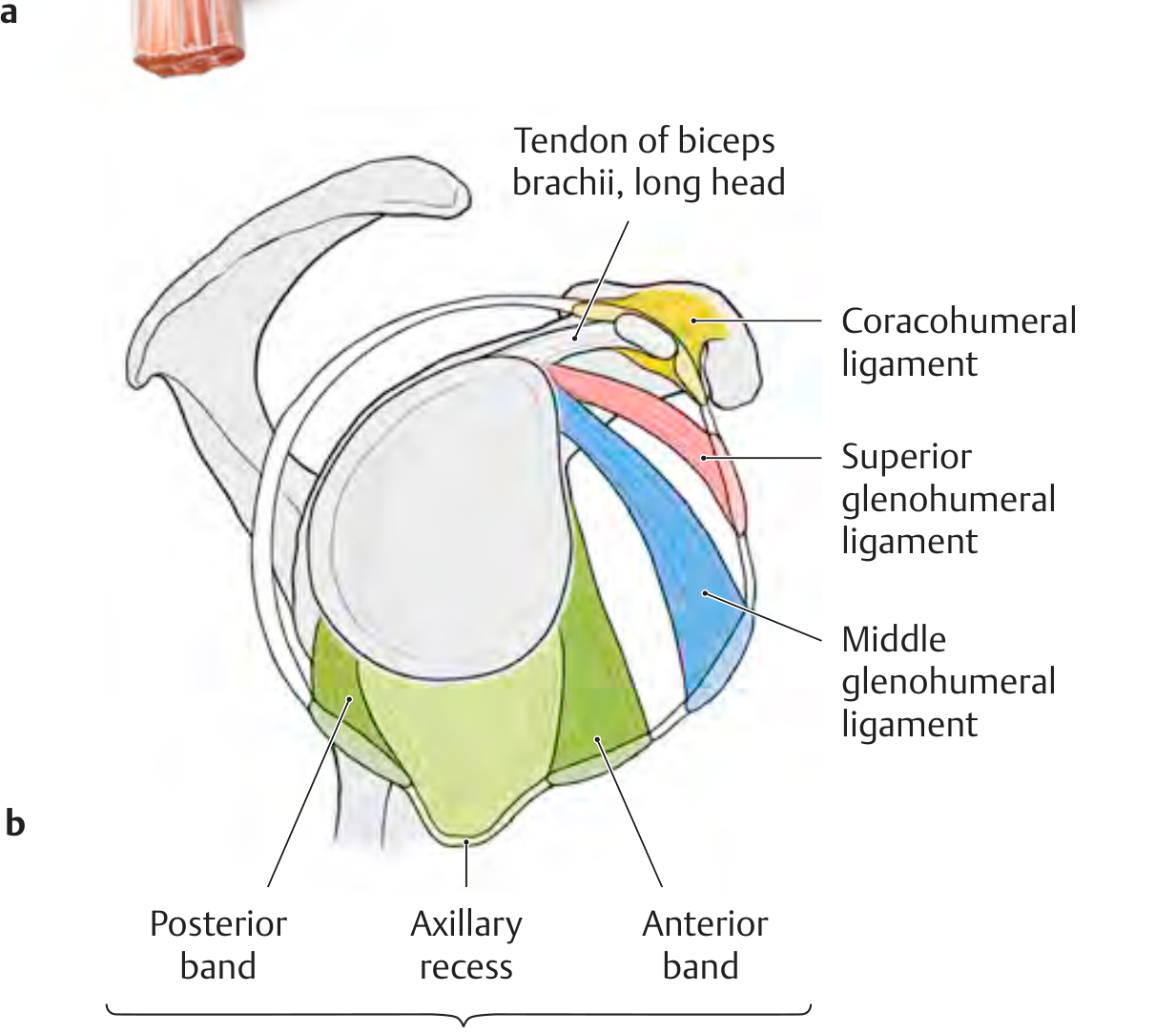
| Superior GH ligament | Upper glenoid → lesser tubercle | Limits inferior translation |
| Middle GH ligament | Upper glenoid → anatomic neck | Anterior stability in mid-abduction |
| Inferior GH ligament | Inferior glenoid → surgical neck | Most important - prevents anterior dislocation |
| Coracohumeral ligament | Coracoid → greater/lesser tubercle | Resists inferior subluxation; stabilizes biceps tendon |
The inferior glenohumeral ligament (with its anterior band, posterior band, and axillary recess) forms a hammock during abduction and is the primary restraint to anterior dislocation.
4. Rotator Cuff Muscles (Dynamic Stabilizers)
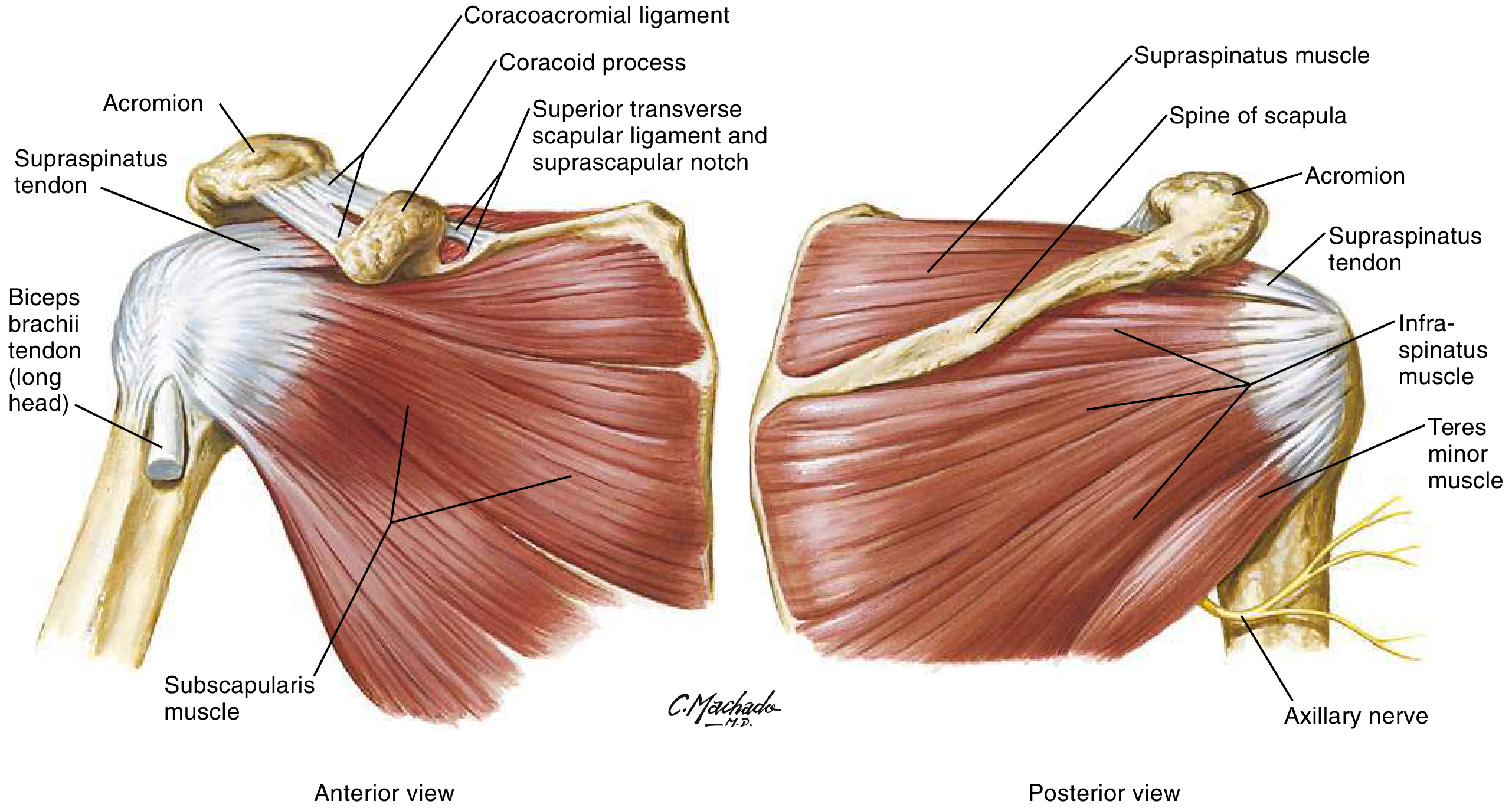
| Muscle | Nerve | Action |
|---|---|---|
| Supraspinatus | Suprascapular (C5) | Initiates abduction (0-15°) |
| Infraspinatus | Suprascapular (C5, C6) | Lateral rotation |
| Teres minor | Axillary (C5) | Lateral rotation |
| Subscapularis | Upper/lower subscapular (C5, C6) | Medial rotation |
5. Movements and Muscles
| Movement | Range | Primary Muscles |
|---|---|---|
| Flexion | 0-180° | Deltoid (anterior), pec major, biceps |
| Extension | 0-60° | Deltoid (posterior), teres major, latissimus dorsi |
| Abduction | 0-180° | Supraspinatus (0-15°), Deltoid (15-90°), trapezius + serratus anterior (90-180°) |
| Adduction | Deltoid, pec major, latissimus dorsi | |
| Medial rotation | Subscapularis, pec major, teres major | |
| Lateral rotation | Infraspinatus, teres minor |
6. Nerve Supply and Blood Supply
- Nerve: Axillary nerve (C5, C6) and suprascapular nerve
- Blood supply: Anterior and posterior circumflex humeral arteries (branches of axillary artery)
7. Clinical Correlations
- Anterior dislocation (95-97%) - most common
- Mechanism: abduction + external rotation (e.g., falling on outstretched arm)
- Humeral head moves anteroinferiorly
- Bankart lesion: avulsion of anteroinferior glenoid labrum - causes recurrent dislocation
- Hill-Sachs lesion: compression fracture of posterosuperior humeral head
- Axillary nerve injury: loss of sensation over "regimental badge" area (lateral arm) + deltoid paralysis
- Most commonly affects supraspinatus tendon
- Presents with painful arc (60-120° of abduction)
- Common in overhead athletes and the elderly
- Fibrosis and contraction of the joint capsule
- Painful restriction of all movements, especially external rotation
- Common in diabetics and middle-aged women
- Can occur with shoulder dislocation or fracture of surgical neck of humerus
- Results in: deltoid paralysis (loss of abduction), loss of sensation over lateral arm
Sources: THIEME Atlas of Anatomy; ROSEN's Emergency Medicine; Gray's Anatomy for Students; Miller's Review of Orthopaedics
Give diagram which i can draw in test easy and drawable
A simple, clean, hand-drawable anatomical diagram of the shoulder joint (glenohumeral joint) suitable for a medical student exam. Black lines on white background, simple schematic style (not realistic). Show: glenoid cavity of scapula on the left (shallow cup shape), humeral head on the right (round ball), glenoid labrum (small rim around glenoid), joint capsule (dashed outline around the joint), coracohumeral ligament (labeled at top), superior glenohumeral ligament, middle glenohumeral ligament, inferior glenohumeral ligament (labeled with arrows), acromion process above, coracoid process, subacromial space, tendon of long head of biceps passing through, rotator cuff muscles labeled as SITS (supraspinatus on top, subscapularis anterior, infraspinatus and teres minor posterior). All labels in clear simple text with leader lines. Simple enough for a student to copy in an exam in 3 minutes.
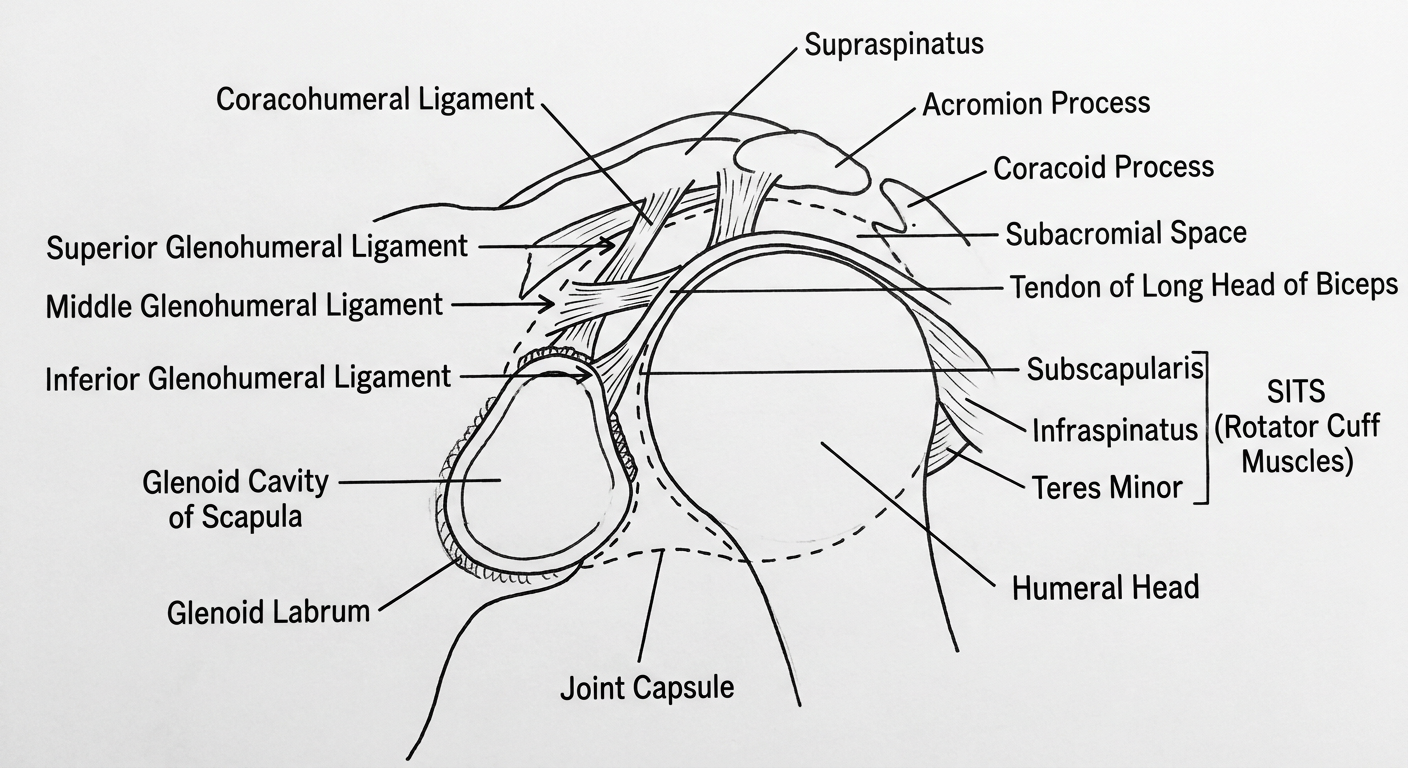
- Draw a shallow cup on the left = glenoid cavity, with a small rim = labrum
- Draw a large circle fitting into the cup = humeral head
- Draw a dashed oval around the joint = capsule
- Add the acromion as a shelf above (flat hook shape)
- Add the coracoid process as a beak below-front
- Label the 3 GH ligaments (superior, middle, inferior) on the anterior capsule
- Draw 4 small arrows around the humeral head for SITS rotator cuff
- Add the biceps tendon coming out of the top of the joint
- Glenoid labrum
- Articular capsule
- Inferior GH ligament (most important!)
- SITS muscles (especially supraspinatus on top)
- Axillary nerve below the joint
- Acromion + coracohumeral ligament
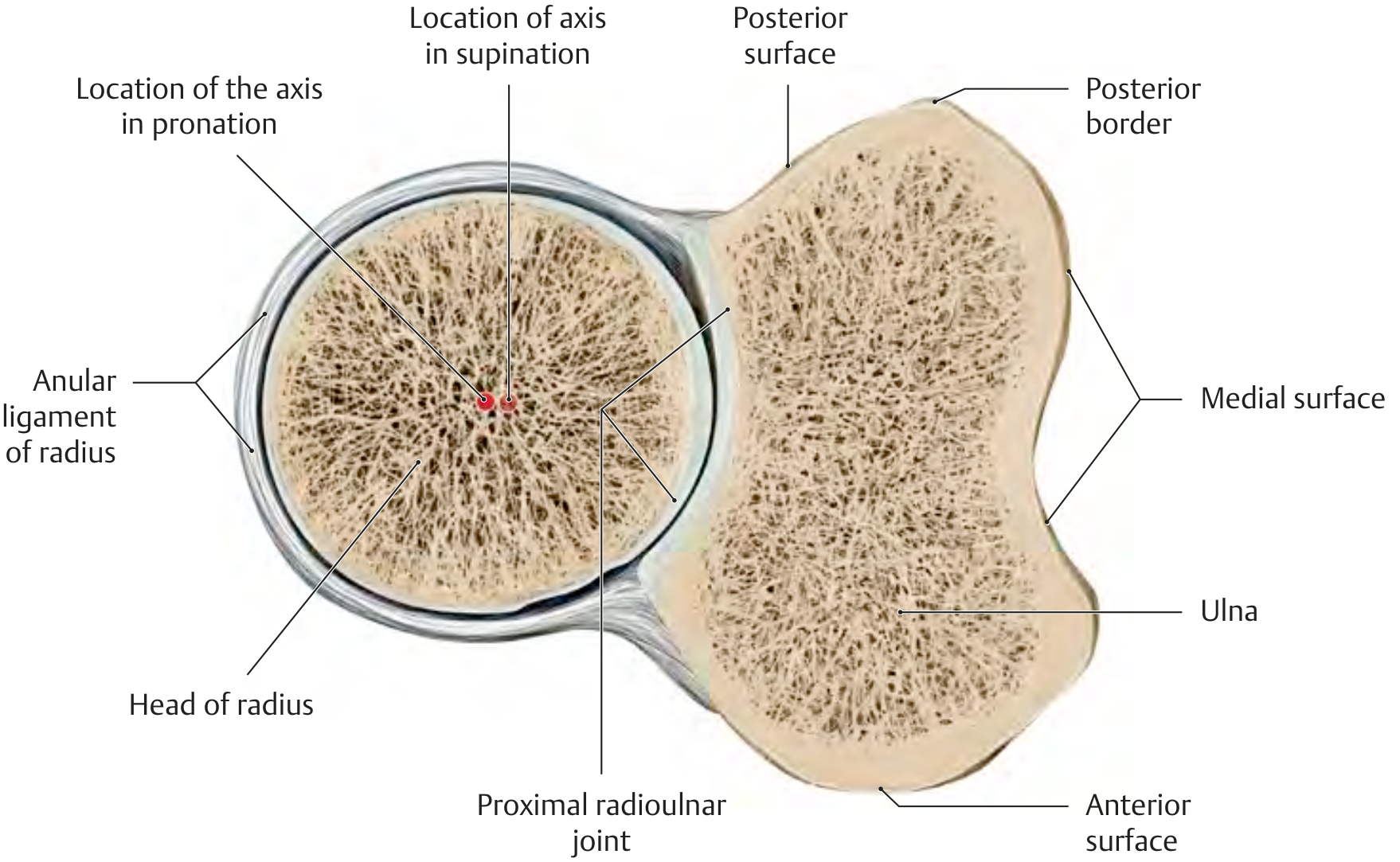
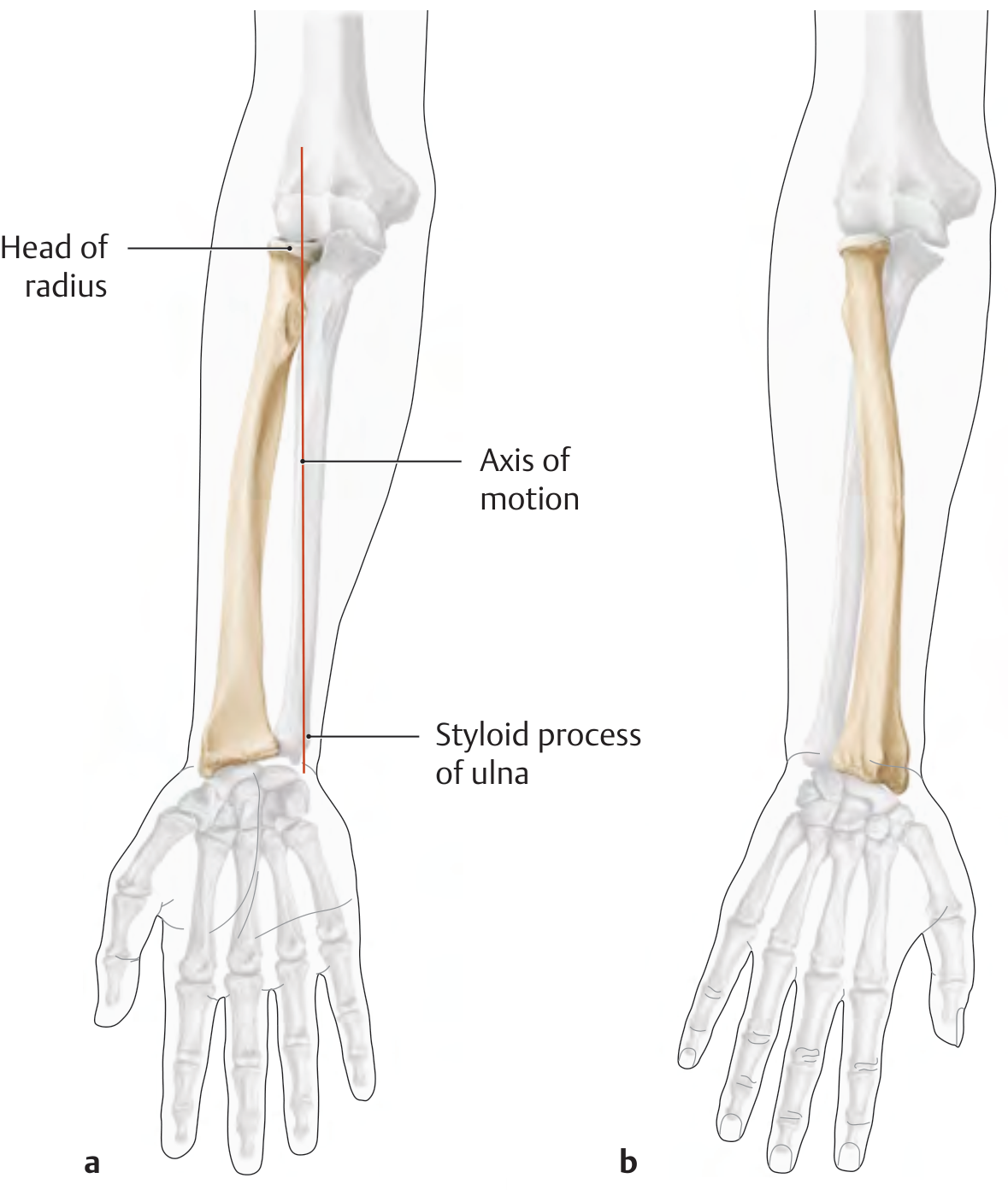
Movement at Radioulnar Joint.
Simple clean black-and-white schematic diagram for a medical student to draw in an exam, showing movements at the radioulnar joints. Two side-by-side panels: Left panel labeled "SUPINATION" showing radius and ulna parallel, with radius lateral to ulna, palm facing up, axis of rotation shown as dotted vertical line from radial head to ulnar styloid. Right panel labeled "PRONATION" showing radius crossed over ulna, palm facing down. Between both panels show the interosseous membrane connecting radius and ulna. Label clearly: proximal radioulnar joint (top, pivot joint), distal radioulnar joint (bottom), annular ligament at proximal joint, interosseous membrane in middle, articular disc at distal joint. Add arrows showing direction of rotation. Below each panel list muscles: Supination = Biceps brachii + Supinator. Pronation = Pronator teres + Pronator quadratus. Simple line-art style, easy to copy.
Movements at the Radioulnar Joint
1. Introduction
- Proximal radioulnar joint (PRUJ) - at the elbow
- Distal radioulnar joint (DRUJ) - at the wrist
2. The Two Joints
| Feature | Proximal RUJ | Distal RUJ |
|---|---|---|
| Type | Pivot joint | Pivot joint |
| Articulation | Head of radius in radial notch of ulna | Head of ulna in ulnar notch of radius |
| Key stabiliser | Annular ligament (holds radial head) | Articular disc (triangular fibrocartilage) |
| Location | Just below elbow | Just above wrist |
3. Movements: Pronation and Supination
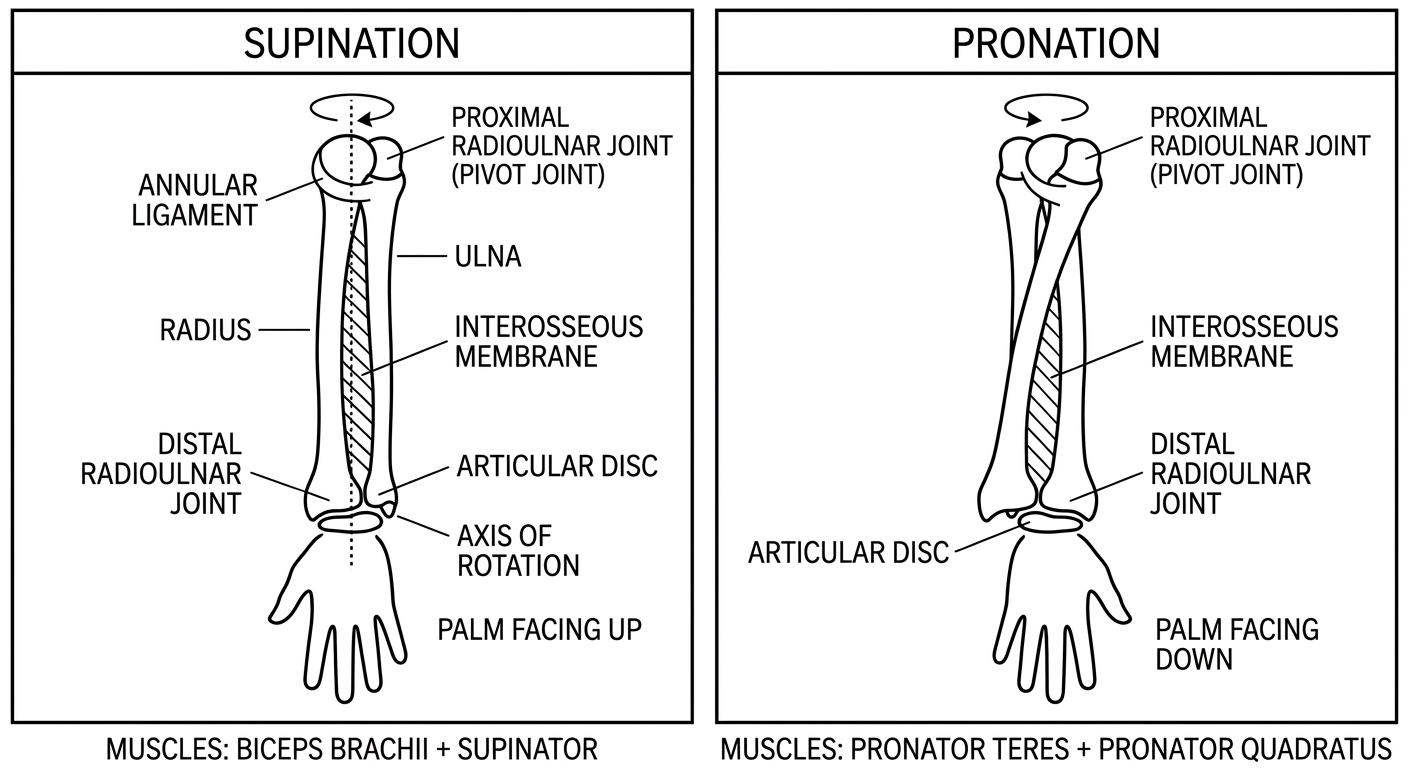
- In supination: radius and ulna lie parallel to each other, palm faces anteriorly (up)
- In pronation: radius crosses over the ulna, palm faces posteriorly (down)
- The ulna remains fixed - only the radius rotates around it
4. Range of Motion
- Supination: 0° → 90° (from neutral/anatomical position)
- Pronation: 0° → 85°
- Combined functional range used in daily activities: ~170°
5. Muscles Producing Movement
| Movement | Muscles | Nerve |
|---|---|---|
| Supination | Biceps brachii (most powerful) | Musculocutaneous (C5, C6) |
| Supinator | Posterior interosseous (C6, C7) | |
| Pronation | Pronator teres | Median nerve (C6, C7) |
| Pronator quadratus (prime mover) | Anterior interosseous (C7, C8) |
Memory tip: Supination is the stronger movement (turning a screwdriver, tightening a bolt). Biceps brachii is the most powerful supinator - hence elbow must be flexed for maximum supination power.
6. Role of Interosseous Membrane
- A strong fibrous sheet connecting radius and ulna between the two joints
- Transmits forces from radius to ulna (e.g., a fall on outstretched hand)
- Functionally links PRUJ and DRUJ - movement at one joint requires movement at the other
7. Clinical Correlations
- Common in children under 6 years
- Sudden pull on the child's hand causes radial head to slip under the annular ligament
- Child holds forearm in pronation and refuses to move it
- Treatment: Supination + flexion manoeuvre to reduce
- Fracture of distal radius - disrupts the DRUJ
- Affects pronation and supination
- Injury at the radial neck/arcade of Frohse
- Supinator muscle denervated → weakness of supination
- No sensory loss (pure motor nerve)
Sources: Gray's Anatomy for Students; THIEME Atlas of Anatomy; Rockwood & Green's Fractures in Adults
Movement at radioulnar joint
Movement at the Radioulnar Joint - Quick Summary
Two Joints, One Movement
- Proximal RUJ (pivot joint) - radial head in radial notch of ulna, held by annular ligament
- Distal RUJ (pivot joint) - head of ulna in ulnar notch of radius, stabilized by articular disc
- Linked by the interosseous membrane
Only Two Movements
| Movement | Description | Range |
|---|---|---|
| Supination | Radius + ulna parallel, palm faces up | 0-90° |
| Pronation | Radius crosses over ulna, palm faces down | 0-85° |
Muscles
| Movement | Muscles | Nerve |
|---|---|---|
| Supination | Biceps brachii + Supinator | Musculocutaneous + Posterior interosseous |
| Pronation | Pronator teres + Pronator quadratus | Median nerve |
Clinical Points
- Pulled elbow (children) - radial head slips under annular ligament; treat by supination + flexion
- Colles' fracture - disrupts DRUJ
- Posterior interosseous nerve palsy - weak supination
Drawable Diagram
Give detail answer with easy drawable diagram and clinical 10 marks
Simple clean black-and-white line art diagram for a medical student exam showing Radioulnar Joints. Draw two forearm diagrams side by side. Left diagram labeled "SUPINATION - palm up" shows radius (thin bone) and ulna (thick bone) parallel, radius on lateral side, ulna on medial side. Right diagram labeled "PRONATION - palm down" shows radius crossing over ulna forming an X shape. On both diagrams label: at the top - "Proximal Radioulnar Joint (Pivot)" with annular ligament drawn as a ring around radial head. At the bottom - "Distal Radioulnar Joint (Pivot)" with articular disc labeled. In the middle - "Interosseous Membrane" shown as diagonal lines connecting radius and ulna. Add a dotted line showing Axis of Rotation from radial head to ulnar styloid. Below the diagrams, add a simple table: SUPINATION muscles = Biceps brachii (stronger), Supinator. PRONATION muscles = Pronator teres, Pronator quadratus. Clean, minimal, easy to draw in 3 minutes.
Movements at the Radioulnar Joint (10 Marks)
1. Introduction
- Proximal Radioulnar Joint (PRUJ) - just below the elbow
- Distal Radioulnar Joint (DRUJ) - just above the wrist
2. Proximal Radioulnar Joint (PRUJ)
| Feature | Detail |
|---|---|
| Type | Pivot (trochoid) synovial joint |
| Articulation | Cylindrical head of radius rotates within radial notch of ulna |
| Capsule | Shared with elbow joint |
| Key ligament | Annular ligament - a strong fibrous ring that wraps around radial head, holding it in radial notch; attached to anterior and posterior margins of radial notch of ulna |
| Nerve supply | Musculocutaneous, radial, median nerves |
3. Distal Radioulnar Joint (DRUJ)
| Feature | Detail |
|---|---|
| Type | Pivot synovial joint |
| Articulation | Head of ulna fits into ulnar notch (sigmoid notch) of radius |
| Key stabiliser | Articular disc (triangular fibrocartilage complex - TFCC) |
| Capsule | Thin, weak; reinforced by dorsal and palmar radioulnar ligaments |
4. Interosseous Membrane
- A strong fibrous sheet running diagonally between the radius and ulna
- Fibres run obliquely downward and medially from radius to ulna
- Functions:
- Mechanically links PRUJ and DRUJ - so both joints always move together
- Transmits force from radius to ulna (e.g., fall on outstretched hand transfers force proximally)
- Gives attachment to deep muscles of forearm
5. The Two Movements: Pronation and Supination
Axis of Rotation
Easy Drawable Diagram:
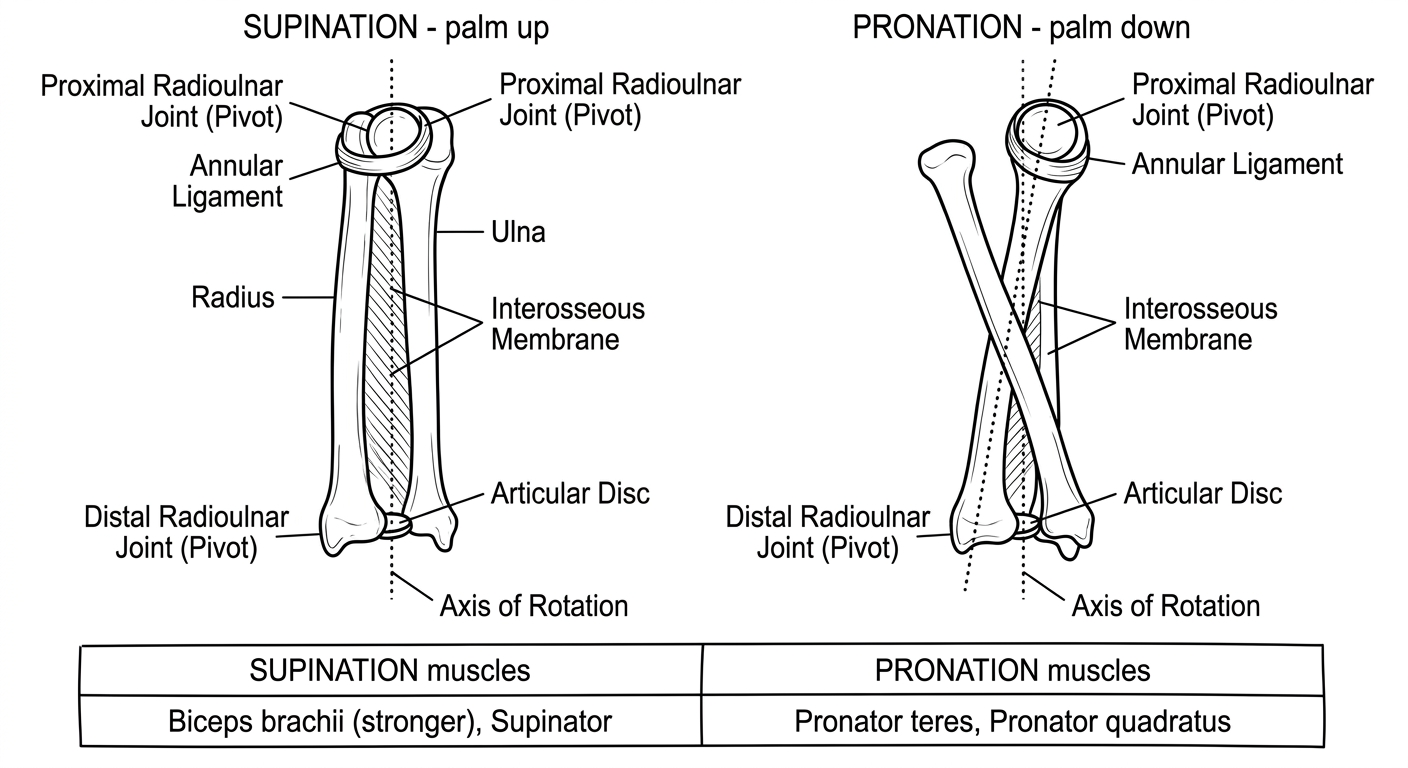
How to Draw This in Exam (2 minutes):
- Draw two vertical forearms side by side
- Left = two parallel bones (radius lateral, ulna medial) - label SUPINATION, palm UP
- Right = radius crossing over ulna forming an X - label PRONATION, palm DOWN
- At top of each: small circle = Proximal RUJ + ring around radial head = Annular ligament
- At bottom: label Distal RUJ + Articular disc
- Middle: diagonal lines between bones = Interosseous membrane
- Dotted line through both = Axis of rotation
6. Range of Motion
| Movement | Range | Position |
|---|---|---|
| Supination | 0° to 90° | Radius and ulna parallel; palm faces anteriorly (up) |
| Neutral | 0° (semipronation) | Thumb points upward |
| Pronation | 0° to 85° | Radius crosses over ulna; palm faces posteriorly (down) |
7. Muscles Producing Movements
Supination Muscles
| Muscle | Origin | Insertion | Nerve |
|---|---|---|---|
| Biceps brachii (most powerful) | Supraglenoid tubercle + coracoid | Radial tuberosity | Musculocutaneous C5, C6 |
| Supinator | Lateral epicondyle + supinator crest of ulna | Upper 1/3 of radius (lateral surface) | Posterior interosseous C6, C7 |
Key point: Biceps brachii is the most powerful supinator - it works best when the elbow is flexed at 90°. When elbow is extended, supinator acts alone.
Pronation Muscles
| Muscle | Origin | Insertion | Nerve |
|---|---|---|---|
| Pronator teres | Medial epicondyle + coronoid process of ulna | Middle 1/3 of radius (lateral surface) | Median nerve C6, C7 |
| Pronator quadratus (prime mover) | Anterior surface of distal ulna | Anterior surface of distal radius | Anterior interosseous C7, C8 |
Key point: Pronator quadratus is the primary pronator at all positions of elbow flexion. Pronator teres assists and acts as accessory.
8. Nerve Supply Summary
| Nerve | Structures supplied |
|---|---|
| Musculocutaneous (C5, C6) | Biceps brachii (supination) |
| Posterior interosseous (C6, C7) | Supinator |
| Median nerve (C6, C7) | Pronator teres |
| Anterior interosseous (C7, C8) | Pronator quadratus |
9. Applied Anatomy / Clinical Correlations
A. Pulled Elbow (Nursemaid's Elbow / Chassaignac's Paralysis)
- Age: Most common in children 1-4 years (annular ligament is lax and weak at this age; becomes stronger with age)
- Mechanism: Sudden axial traction on the child's outstretched, pronated forearm (e.g., swinging a child by the hands, pulling child upstairs)
- Pathology: The annular ligament slips forward and becomes entrapped between the radial head and capitellum of humerus
- Clinical features:
- Sudden pain at elbow
- Child holds arm in slight flexion and pronation (pseudoparalysis - "arm looks paralyzed")
- No swelling or bony tenderness
- Refuses to move the arm
- Treatment: Supination + flexion manoeuvre OR hyperpronation technique
- A click is felt/heard on successful reduction
- Child is symptom-free within minutes after reduction
- X-ray: Usually normal (clinical diagnosis); done to rule out fractures
B. Galeazzi Fracture
- Fracture of middle/distal third of radius + dislocation of DRUJ
- DRUJ is disrupted and unstable
- Treatment: ORIF of radius fracture to restore DRUJ stability
C. Monteggia Fracture
- Fracture of proximal third of ulna + dislocation of radial head at PRUJ
- Anterior dislocation most common (Bado type I)
- Anterior interosseous nerve or radial nerve may be injured
- Treatment: ORIF of ulna + reduction of radial head
D. Posterior Interosseous Nerve (PIN) Palsy
- Compression of PIN in the arcade of Frohse (fibrous edge of supinator)
- Denervates supinator and extensors
- Weakness of supination (biceps partially compensates)
- No sensory loss (pure motor nerve)
E. TFCC (Triangular Fibrocartilage Complex) Tear
- Common in fall on outstretched hand or forceful rotation
- Presents with ulnar-sided wrist pain worsened by forearm rotation
- Diagnosed by MRI arthrography
- Treatment: Arthroscopic debridement or repair
10. Summary Table
| Feature | PRUJ | DRUJ |
|---|---|---|
| Type | Pivot | Pivot |
| Articulating bones | Radial head in radial notch of ulna | Ulnar head in ulnar notch of radius |
| Key stabiliser | Annular ligament | Articular disc (TFCC) |
| Capsule | Shared with elbow | Separate |
| Common injury | Pulled elbow (children) | Galeazzi fracture, TFCC tear |
Sources: THIEME Atlas of Anatomy; Gray's Anatomy for Students; Tintinalli's Emergency Medicine; Campbell's Operative Orthopaedics