A 50y old male complains of dragging sensation in abdomen. Physical examination revealed pallor and massive spleenomegaly. There is no lymphadenopathy. Total leucocyte count is 1,60,000 cell/mm³ and platelet count is 2 Lakhs/mm³. M a) What is the probable diagnosis? b) Describe cytogenetic change in this case? c) Enumerate peripheral blood smear findings?
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
I now have all the information needed for a thorough, well-sourced answer. Here it is:
Clinical Case Analysis
50-year-old male | Dragging abdominal sensation | Pallor | Massive splenomegaly | No lymphadenopathy | TLC 1,60,000/mm³ | Platelets 2 Lakhs/mm³
a) Probable Diagnosis: Chronic Myeloid Leukemia (CML) - Chronic Phase
The clinical triad strongly points to CML:
| Feature | This Case | Significance |
|---|---|---|
| Age/sex | 50-year-old male | Peak incidence 5th-6th decade |
| Dragging sensation in abdomen | Present | Caused by massive splenomegaly |
| Massive splenomegaly | Present | Extramedullary hematopoiesis |
| Pallor | Present | Mild-to-moderate anemia |
| No lymphadenopathy | Absent | Distinguishes from lymphoma/CLL |
| TLC 1,60,000/mm³ (1,60,000 cells/mm³) | Markedly elevated | Leukocytosis often exceeds 1,00,000/µL in CML |
| Platelets 2 Lakhs | Normal-slightly elevated | Typical of CML chronic phase |
As Robbins & Kumar Pathologic Basis of Disease explicitly states: "Sometimes the first symptom is a dragging sensation in the abdomen caused by splenomegaly." CML is primarily a disease of adults with peak incidence in the fifth to sixth decades of life.
The absence of lymphadenopathy is a key feature distinguishing CML from lymphoma/CLL, as CML splenomegaly results from extramedullary hematopoiesis - not lymphoid infiltration.
b) Cytogenetic Change: The Philadelphia Chromosome - t(9;22)(q34;q11)
The Philadelphia (Ph) Chromosome
The hallmark cytogenetic change in CML is the reciprocal translocation between chromosomes 9 and 22: t(9;22)(q34;q11)
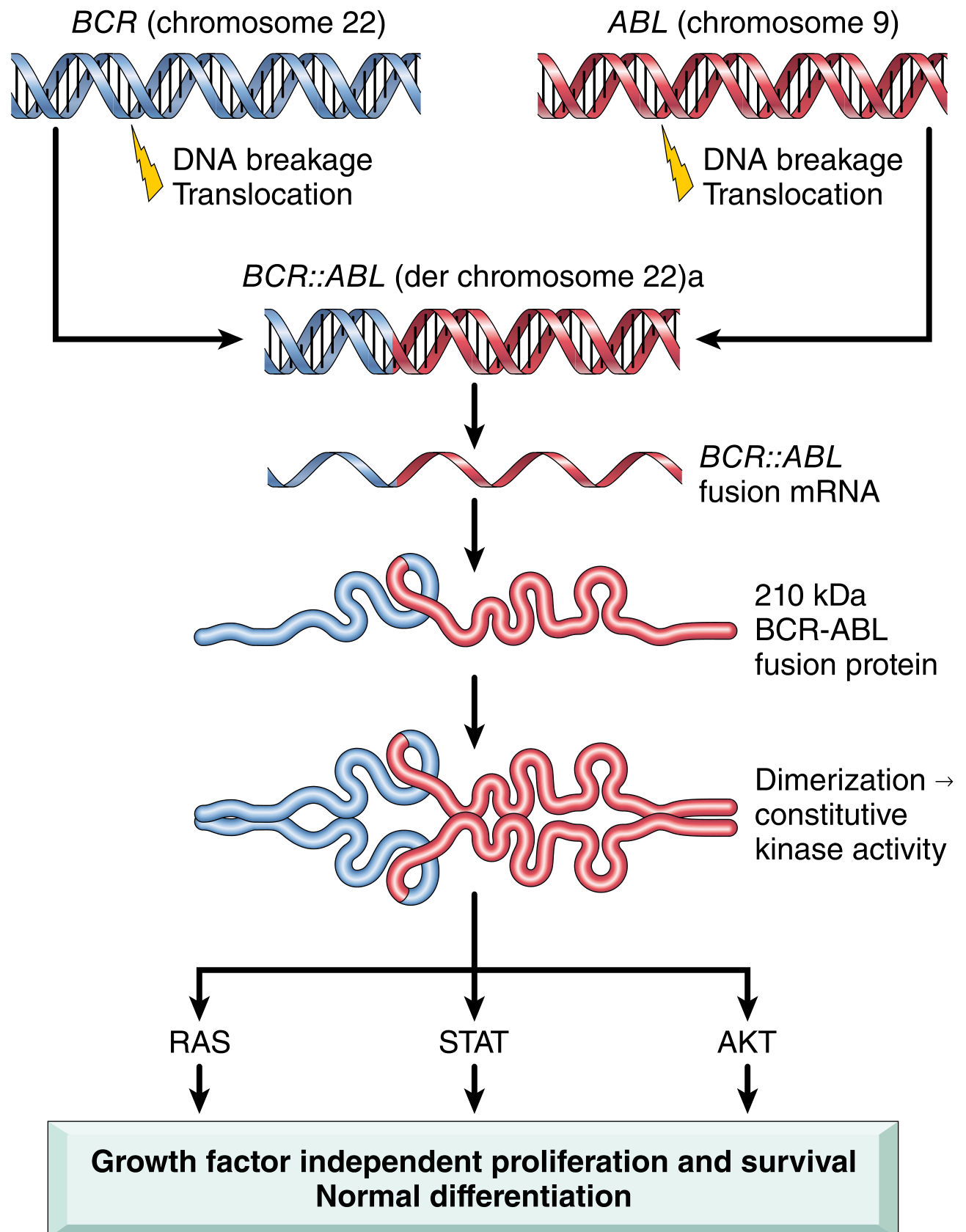
Fig: Pathogenesis of CML - BCR::ABL fusion gene creation and downstream signaling (Robbins & Kumar Pathologic Basis of Disease)
Mechanistic cascade:
- DNA breakage occurs at chromosome 22q11 (BCR gene) and chromosome 9q34 (ABL gene)
- Reciprocal translocation fuses BCR sequences from chromosome 22 with ABL sequences from chromosome 9
- This creates the chimeric BCR::ABL fusion gene on the derivative (shortened) chromosome 22 - the Philadelphia chromosome
- The fusion gene is transcribed into BCR::ABL fusion mRNA
- Translated into a 210 kDa BCR-ABL fusion protein (p210)
- The BCR moiety contains a dimerization domain that causes self-association, leading to constitutive (always "on") ABL tyrosine kinase activity
- The activated kinase phosphorylates downstream proteins activating RAS, JAK/STAT, and AKT pathways - driving growth-factor-independent proliferation and survival
- Net result: increased mature granulocytes and platelets in peripheral blood (differentiation remains intact, unlike acute leukemia)
Key cytogenetic facts:
- Present in >90% of CML cases by karyotype
- The remaining cases have cryptic (karyotypically invisible) BCR-ABL rearrangements detectable only by FISH or PCR
- There is NO BCR-ABL-negative CML - if BCR-ABL is absent by all methods, it is a different disease entity (e.g., atypical CML, chronic neutrophilic leukemia)
- The Ph chromosome results in an elongated chromosome 9 and a shortened chromosome 22
- The cell of origin is a pluripotent hematopoietic stem cell (explaining why blast crisis can be myeloid or lymphoid)
c) Peripheral Blood Smear Findings in CML
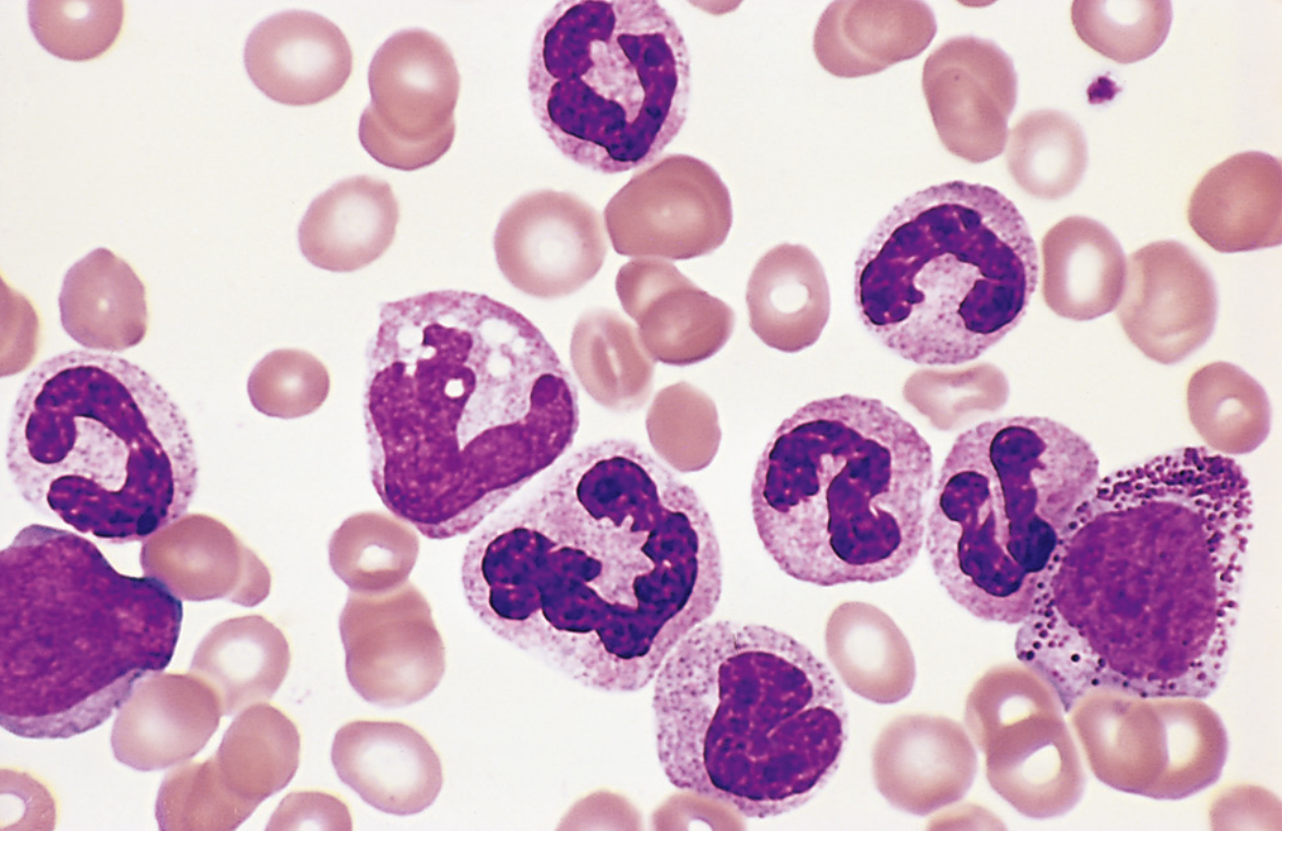
Fig: CML peripheral blood smear showing mature neutrophils, metamyelocytes, and a myelocyte (Robbins & Kumar Pathologic Basis of Disease)
The peripheral blood smear in CML shows a characteristic "left shift" - increased granulocytes at all stages of maturation:
| Finding | Details |
|---|---|
| Leukocytosis | Often >1,00,000 cells/µL; predominantly granulocytic |
| Neutrophilia | Mature neutrophils predominate |
| Band forms | Increased band neutrophils |
| Metamyelocytes | Present in increased numbers |
| Myelocytes | Present - classically myelocytes > metamyelocytes (opposite of leukemoid reaction) |
| Promyelocytes | May be present |
| Blasts | Usually <10% in chronic phase |
| Basophilia | Characteristically increased - a distinguishing feature |
| Eosinophilia | Present |
| Thrombocytosis | Platelets often increased, sometimes markedly |
| Anemia | Mild to moderate normocytic normochromic anemia |
Distinguishing CML from Leukemoid Reaction on smear:
| Feature | CML | Leukemoid Reaction |
|---|---|---|
| Myelocyte:metamyelocyte ratio | Myelocytes > metamyelocytes | Metamyelocytes > myelocytes |
| Basophilia | Present | Absent |
| Eosinophilia | Present | Absent |
| Anemia | Present | Absent |
| Thrombocytosis | Present | Absent |
| LAP (Leukocyte Alkaline Phosphatase) score | Low/absent | High |
| Philadelphia chromosome | Present | Absent |
Sources:
- Robbins, Cotran & Kumar - Pathologic Basis of Disease, Ch. 13 (Chronic Myeloid Leukemia)
- Robbins & Kumar - Basic Pathology
- Goldman-Cecil Medicine - Chronic Myelogenous Leukemia chapter
This is a shared conversation. Sign in to Orris to start your own chat.