NLEP PROGRAMMES STRICTLY FROM THE PARK TEXTBOOK ONLY SPM IT IS UNIVERSITY LAQ EXAM and also about sparsh awareness campaign
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
I now have comprehensive content from Park's textbook. Let me compile the full LAQ answer.
NATIONAL LEPROSY ERADICATION PROGRAMME (NLEP)
From: Park's Textbook of Preventive and Social Medicine
Historical Background
The National Leprosy Control Programme (NLCP) has been in operation since 1955, as a centrally aided programme. It aimed at control of leprosy through early case detection and DDS (dapsone) monotherapy on an ambulatory basis. The programme gained momentum during the Fourth Five Year Plan after being made a centrally-sponsored programme.
In 1980, the Government of India declared its resolve to "eradicate" leprosy by the year 2000 and constituted a Working Group to advise accordingly. The Working Group submitted its report in 1982 and recommended a revised strategy based on multi-drug chemotherapy (MDT) aimed at:
- Reduction in the quantum of infection in the population
- Reduction in sources of infection
- Breaking the chain of transmission
In 1983, the control programme was redesignated National Leprosy "Eradication" Programme (NLEP) with the goal of eradicating the disease by the turn of the century. The aim was to reduce case load to 1 or less than 1 per 10,000 population.
World Bank Support & Integration
- The first World Bank supported project was introduced in 1993 to strengthen leprosy elimination.
- The 2nd phase began in 2001-02 and ended in December 2004.
- Since then, the programme is continued with Government of India funds with technical support from WHO and ILEP.
- The programme was integrated with the general health care system in 2002-03; leprosy diagnosis and treatment services are available at all PHCs and government hospitals.
Components of the Programme
- Decentralized integrated leprosy services through general health care system
- Capacity building of all general health services functionaries
- Intensified IEC (Information, Education, and Communication)
- Prevention of disability and medical rehabilitation
- Intensified monitoring and supervision
Achievements
After introduction of MDT, the recorded case load of leprosy came down from 57.6 cases per 10,000 population in 1981 to less than 1 at the national level in December 2005. The country achieved the goal of leprosy elimination at national level as set by the National Health Policy (2002). 34 states/UTs achieved elimination status. Only 2 states/UTs - Chhattisgarh and Dadra & Nagar Haveli - were yet to achieve elimination.
- A total of 209 high endemic districts were identified for special action during 2012-13.
- 1792 blocks and 150 urban areas were identified for special activities (house-to-house survey + IEC + capacity building).
Major Initiatives
- New case detection rate is now the main indicator for programme monitoring (rather than prevalence).
- Treatment completion rate is taken as an important indicator, calculated by states on a yearly basis.
- DPMR (Disability Prevention and Medical Rehabilitation) services are emphasized:
- Dressing materials, supportive medicines, and ulcer kits are provided.
- Micro-cellular rubber (MCR) footwear is provided for insensitive feet.
- 41 NGOs and 42 Government Medical Colleges (total 83 centres) are strengthened for reconstructive surgery (RCS) services.
- Rs. 5,000/- provided as incentive to each leprosy-affected BPL patient undergoing RCS.
- Rs. 5,000/- per RCS conducted is also provided to government institutions.
- ASHAs are involved in detecting suspected leprosy cases and ensuring treatment completion.
ASHA Incentives
| Activity | Incentive |
|---|---|
| Confirmed diagnosis of case brought by ASHA | Rs. 250/- |
| Treatment completion - PB leprosy case | Rs. 400/- |
| Treatment completion - MB leprosy case | Rs. 600/- |
| Early case (before onset of visible deformity) | Rs. 250/- |
| New case with visible deformity in hands/feet/eye | Rs. 200/- |
ASHA Based Surveillance for Leprosy Suspects (ABSULS) was launched on 1st July 2019.
There are 612 self-settled colonies in the country where more than 50,000 leprosy-affected persons reside - free medical facilities are provided to them.
Three-Pronged Strategy (from 2016-17)
Introduced in NLEP from 2016-17, the three components are:
- Leprosy Case Detection Campaign (LCDC)
- Focused Leprosy Campaign
- Special Plan for Hard to Reach Areas
- LCDC (2016-17): Carried out in 163 districts of 20 states, wherein 34,672 cases were detected and put on treatment. Due to the success (drastic decline of grade 2 disability), LCDC was continued.
- LCDC (2017-18): About 305 districts in 23 states were identified for Phase I.
- Focused Leprosy Campaign: House-to-house survey in villages/urban areas (covering 300 households) where one case of grade 2 disability was detected.
- Special plan for hard to reach areas: Targets populations in difficult terrains, naxalite-affected areas, and other geographically difficult locations.
Programme Strategy (12th Plan Period)
Main strategies followed:
- Integrated leprosy services through general health care system
- Early detection and complete treatment of new leprosy cases
- Household contact survey for early detection
- Involvement of ASHA in detection and completion of treatment
- Strengthening of DPMR services
Case Detection and Management
Since people are hesitant due to stigma, states were advised to draw up innovative plans:
- Improve access to services
- Involve women including leprosy-affected persons in case detection
- Organize skin camps for detecting leprosy patients while providing services for other skin conditions
- Undertake contact survey to identify the source in the neighbourhood of each child or multibacillary case
- Increase awareness through ANM, AWW, ASHA and other health workers
A "District Leprosy Cell" - a team of dedicated workers including medical officer and para-medical workers - is placed at district level to provide technical support to the primary health care system.
Disability Prevention and Medical Rehabilitation (DPMR)
DPMR activities are carried out in a three-tier system:
| Level | Institutions |
|---|---|
| Primary (1st level) | All PHCs, CHCs, Sub-divisional hospitals, Urban leprosy centres |
| Secondary (2nd level) | District HQ Hospitals, District Nucleus Units |
| Tertiary (3rd level) | CLTRI Chingalpettu, RLTRIs (Aska/Gauripur/Raipur), JALMA Agra, NGO RCS centres |
IEC/BCC
The IEC strategy during the 12th Plan focused on communication for behavioural change in the general public against stigma and discrimination. Key messages included:
- Availability of MDT
- Correction of deformity through surgery
- That leprosy-affected persons can live a normal life with the family
An intensive IEC campaign with the theme "Towards Leprosy Free India" was carried out.
Research Institutes
Research is carried out at:
- Central JALMA Institute of Leprosy, Agra
- Central Leprosy Teaching and Training Institute (CLTRI), Chingelput, Chennai
- Regional Training and Referral Institutes at Aska (Odisha), Raipur (Chhattisgarh), Gouripur (West Bengal)
ILEP Agencies
The International Federation of Anti-Leprosy Associations (ILEP) is actively involved as partner in NLEP. In India, ILEP is constituted by 10 agencies, including The Leprosy Mission and Damien Foundation of India Trust.
SPARSH LEPROSY AWARENESS CAMPAIGN
From: Park's Textbook of Preventive and Social Medicine
| Feature | Details |
|---|---|
| Launched | 2017 |
| Platform | Through Gram Sabhas |
| Implementing agencies | Panchayat and Village Health and Sanitation Community |
| Aim | Generate awareness, reduce stigma, improve self-reporting of cases |
| Coverage | Carried out in 60% of total villages across India |
| Continuation | Campaign continued during the year 2018 |
The Sparsh campaign was a community-based initiative specifically designed to tackle the stigma associated with leprosy - a major barrier to early self-reporting and timely treatment.
Survey, Education and Treatment (SET) Scheme (related)
Under the SET scheme, NGOs are presently involved in:
- Disability prevention and ulcer care
- IEC
- Referral of suspected cases
- Referral for Reconstructive Surgery (RCS)
- Research and rehabilitation
NGO support is mainly required for follow-up of under-treatment cases in urban locations and difficult to reach areas.
Incentive to Patient (as of 2017)
An incentive of Rs. 8,000/- will be paid to all patients affected by leprosy undergoing major reconstructive surgery (irrespective of financial status). Payment is made by the District Leprosy Officer. As on January 2017, there were 115 recognized RCS centres (61 Government + 54 NGO) in the country.
NLEP at PHC Level (Essential Activities)
Under NHM, NLEP activities at PHC level include:
- Health education to community regarding leprosy
- Diagnosis and management of leprosy and its complications including reactions
- Training of leprosy patients having ulcers for self-care
- Counselling for leprosy patients for regularity/completion of treatment and prevention of disability
- Park's Textbook of Preventive and Social Medicine, Chapter on National Health Programmes (Leprosy section, pp. 476-482 and p. 1004)
In detail nah...u missed pillars and other points...not randomly but orderly...no confusion but same from the park for University laq exam pov
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Here is the complete, ordered, exam-ready LAQ on NLEP and Sparsh - strictly from Park's textbook, covering every heading and sub-point in sequence:
NATIONAL LEPROSY "ERADICATION" PROGRAMME (NLEP)
Park's Textbook of Preventive and Social Medicine
1. HISTORICAL BACKGROUND
- National Leprosy Control Programme (NLCP) started in 1955 as a centrally aided programme.
- Strategy: Early case detection + DDS (dapsone) monotherapy on an ambulatory basis.
- The programme moved ahead at a slow pace for nearly two decades due to lack of clear-cut policies or operational objectives.
- Gained momentum during the Fourth Five Year Plan when it became a centrally-sponsored programme.
- In 1980, Government of India declared its resolve to "eradicate" leprosy by year 2000; constituted a Working Group.
- The Working Group submitted its report in 1982 and recommended a revised strategy based on multi-drug chemotherapy (MDT) aimed at:
- Reduction in the quantum of infection in the population
- Reduction in sources of infection
- Breaking the chain of transmission
- In 1983, the programme was redesignated National Leprosy "Eradication" Programme (NLEP) with the goal of eradicating the disease by the turn of the century.
- Goal: Reduce case load to 1 or less than 1 per 10,000 population.
2. WORLD BANK SUPPORT & INTEGRATION
- 1st World Bank supported project: Introduced in 1993 to strengthen leprosy elimination.
- 2nd World Bank phase: Started 2001-02, ended December 2004.
- Since then: Programme continued with Government of India funds + technical support from WHO and ILEP.
- Integration with general health care system in 2002-03 - leprosy diagnosis and treatment services now available at all PHCs and government hospitals.
3. COMPONENTS OF THE PROGRAMME (5 PILLARS)
- Decentralized integrated leprosy services through general health care system
- Capacity building of all general health services functionaries
- Intensified Information, Education and Communication (IEC)
- Prevention of disability and medical rehabilitation (DPMR)
- Intensified monitoring and supervision
4. ACHIEVEMENTS
- After MDT introduction: case load fell from 57.6 per 10,000 in 1981 to less than 1 per 10,000 at national level in December 2005.
- Country achieved the goal of leprosy elimination at national level as set by National Health Policy (2002).
- 34 states/UTs achieved the status of leprosy elimination.
- Only 2 states/UTs - Chhattisgarh and Dadra & Nagar Haveli - were yet to achieve elimination.
- Bihar, Goa, Chandigarh and Odisha (who achieved elimination earlier) showed PR > 1 per 1000 population.
- 209 high endemic districts identified for special action during 2012-13.
- 1792 blocks and 150 urban areas identified for special activities (house-to-house survey + IEC + capacity building).
5. MAJOR INITIATIVES
(1) More focus now given to new case detection rate (main indicator for programme monitoring) rather than prevalence.
(2) Treatment completion rate taken as an important indicator - calculated by states yearly.
(3) Emphasis on DPMR services:
- (a) Dressing materials, supportive medicines and ulcer kits provided to leprosy-affected persons with ulcers/wounds; also to those in self-settled colonies.
- (b) Micro-cellular rubber (MCR) footwear provided for protection of insensitive feet.
- 41 NGOs + 42 Government Medical Colleges = 83 centres strengthened for reconstructive surgery (RCS).
- Rs. 5,000/- as incentive to each leprosy-affected BPL person undergoing RCS (to compensate for loss of wages).
- Rs. 5,000/- per RCS also provided to government institutions/PMR centres.
(4) ASHA involvement - bringing suspected leprosy cases for diagnosis and treatment + follow-up for treatment completion.
ASHA Incentives:
| Activity | Amount |
|---|---|
| Confirmed diagnosis of case brought by ASHA | Rs. 250/- |
| Treatment completion - PB leprosy | Rs. 400/- |
| Treatment completion - MB leprosy | Rs. 600/- |
| Early case (before visible deformity) | Rs. 250/- |
| New case with visible deformity (hands/feet/eye) | Rs. 200/- |
Activities performed by ASHA:
- (a) Search for suspected cases before any disability appears - ASHA Based Surveillance for Leprosy Suspects (ABSULS) launched on 1st July 2019.
- (b) Follow-up all cases for treatment completion; look for symptoms of reaction and refer to HW/PHC.
- (c) Advise and motivate self-care practices for disabled cases.
- (d) Spread awareness.
- (e) Free medical facilities (ulcer care, self-care training, counselling, MCR footwear) provided to leprosy persons in 612 self-settled colonies housing more than 50,000 leprosy-affected persons, through PMW/NGOs on weekly/fortnightly basis.
(5) Intensive IEC campaign with theme "Towards Leprosy Free India" - carried out for early reporting, treatment completion, quality services, and reduction of stigma/discrimination.
6. DISABILITY PREVENTION AND MEDICAL REHABILITATION (DPMR)
Main activities under DPMR:
- Implementation of DPMR activities as per guidelines - treatment of leprosy reaction, ulcers, physiotherapy, RCS, MCR footwear.
- Integrating DPMR services - convergence of NLEP into NRHM facilitates integration with other departmental disability services.
- Develop a referral system to provide DPMR services to all leprosy-disabled persons in an integrated set-up.
Three-tier system for DPMR:
| Level | Institutions |
|---|---|
| Primary (1st level) | All PHCs, CHCs, Sub-divisional hospitals, Urban leprosy centres/dispensaries |
| Secondary (2nd level) | District HQ Hospitals, District Nucleus Units |
| Tertiary (3rd level) | CLTRI Chingalpettu, RLTRI at Aska/Gauripur/Raipur, ICMR-JALMA Agra, NGO RCS centres |
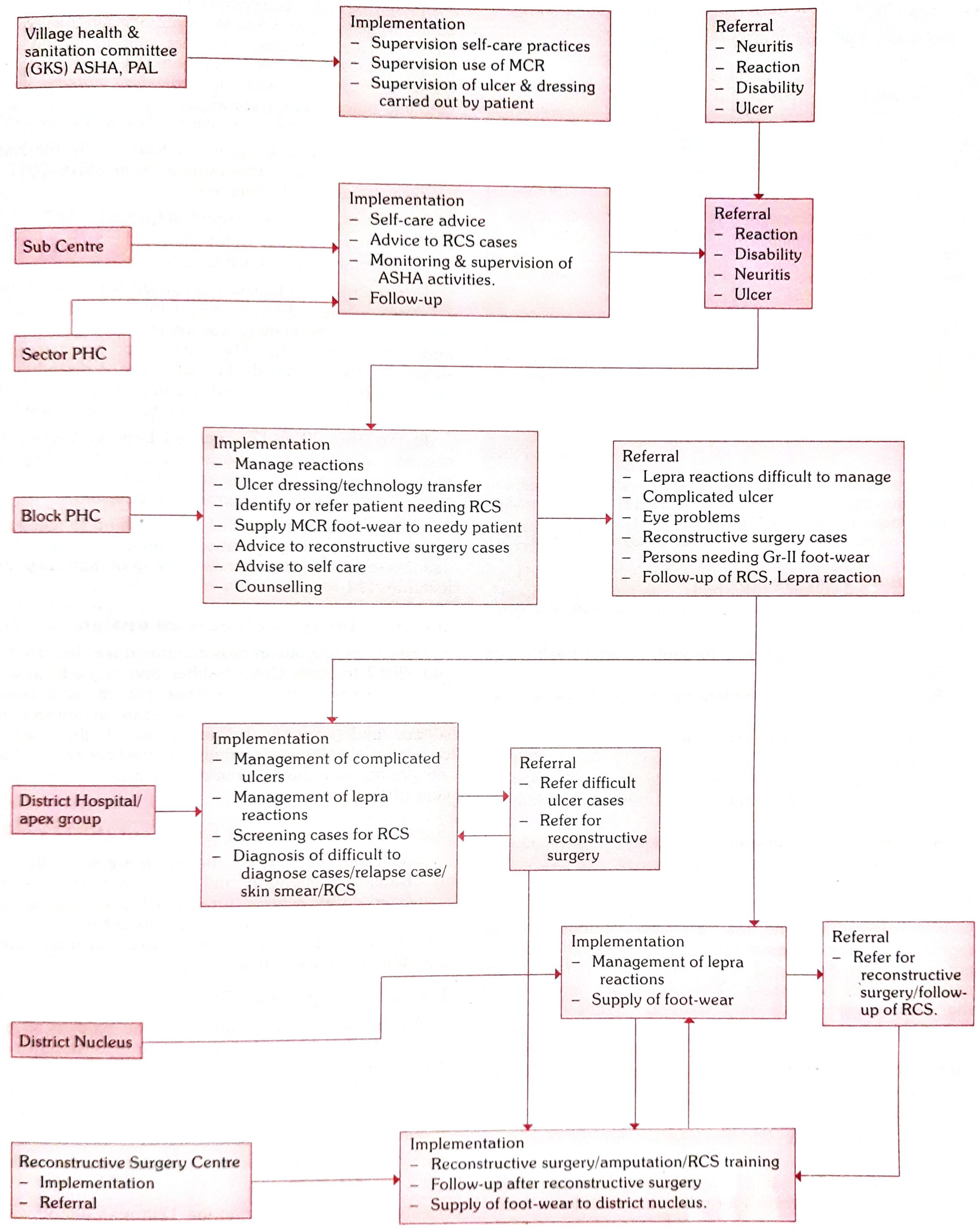
Referral System in NLEP (from the textbook diagram, p.479):
7. SERVICES IN URBAN AREAS
- Urban areas differ from rural due to non-availability of PHC infrastructure and manpower at domiciliary level.
- More cases detected in urban areas (due to migration, good institutions, easy accessibility) BUT treatment completion rate is less compared to rural areas.
- 524 urban localities identified out of 4,388 urban areas (Census 2011) for special action - having population >1,00,000.
- These urban areas are categorized as:
- (a) Town and city (population 1 lac to 5 lacs) - 432 areas
- (b) Medium city (>5 lac to 1 million) - 53 areas
- (c) Mega city (>1 million to 4.5 million) - 34 areas
- (d) Areas with >4.5 million population - 5 areas
8. PROGRAMME IMPLEMENTATION PLAN FOR 12TH PLAN PERIOD (2012-13 to 2016-17)
Objectives (as disease still prevalent with moderate endemicity in ~15% of country):
- a. Elimination of leprosy - prevalence of less than 1 case per 10,000 population in all districts.
- b. Strengthen DPMR of persons affected by leprosy.
- c. Reduction in the level of stigma associated with leprosy.
Targets (Table 3 - Targets for plan period 2012-13 to 2016-17):
| Indicator | Baseline (2011-12) | Target (by March 2017) |
|---|---|---|
| Prevalence Rate (PR) < 1/10,000 | 77% districts | 100% districts |
| New Case Detection Rate (NCDR) | 9.71/1,00,000 | 8/1,00,000 |
| Grade 2 disability among new cases | 3.93% | <2% |
| Child proportion among new cases | 9.78% | <8% |
| Treatment completion rate | PB-67%, MB-59% | PB-90%, MB-85% |
9. PROGRAMME STRATEGY (12TH PLAN)
Main strategies:
- Integrated leprosy services through general health care system
- Early detection and complete treatment of new leprosy cases
- Household contact survey for early detection
- Involvement of ASHA in detection and completion of treatment
- Strengthening of DPMR services
10. CASE DETECTION AND MANAGEMENT
-
People are hesitant to come forward for diagnosis/treatment due to stigma.
-
Early detection at the early stage is the only solution to cut transmission and prevent disabilities.
-
States are advised to draw up innovative plans:
- (i) Improve access to services
- (ii) Involve women including leprosy-affected persons in case detection
- (iii) Organize skin camps for detecting leprosy patients
- (iv) Undertake contact survey to identify the source in the neighbourhood of each child or multibacillary case
- (v) Increase awareness through ANM, AWW, ASHA and other health workers
-
Integrated leprosy services through all PHC facilities will continue in rural areas.
-
For technical support: a team of dedicated workers (MO + para-medical workers) placed at district level - called "District Leprosy Cell".
Three-Pronged Strategy (Introduced from 2016-17):
1. Leprosy Case Detection Campaign (LCDC)
- 2016-17: Carried out in 163 districts of 20 states - 34,672 cases detected and put on treatment.
- Aimed at early case detection and timely treatment.
- Success (drastic decline of grade 2 disability) led to continuation.
- 2017-18: 305 districts in 23 states identified for LCDC Phase I.
2. Focused Leprosy Campaign
- House-to-house survey in villages/urban areas (covering 300 households) wherever one case of Grade 2 disability due to leprosy was detected.
3. Special Plan for Hard to Reach Areas
- Purpose: Find cases in populations in difficult terrains, naxalite-affected areas, and other geographically difficult locations.
11. SPARSH LEPROSY AWARENESS CAMPAIGN
| Feature | Details |
|---|---|
| Launched | 2017 |
| Platform | Through Gram Sabhas |
| Implementing agencies | Panchayat and Village Health and Sanitation Community |
| Aims | Generate awareness, reduce stigma, improve self-reporting of cases |
| Coverage | Carried out in 60% of total villages across India |
| Continuation | Campaign continued in 2018 |
12. SURVEY, EDUCATION AND TREATMENT (SET) SCHEME
Under the SET scheme, NGOs are presently involved in:
- Disability prevention and ulcer care
- IEC
- Referral of suspected cases
- Referral for Reconstructive Surgery (RCS)
- Research and rehabilitation
NGO support is mainly required for follow-up of under-treatment cases in urban locations and difficult to reach areas.
13. INCENTIVE TO PATIENT
- An incentive of Rs. 8,000/- paid to all leprosy patients undergoing major reconstructive surgery (irrespective of financial status).
- Payment made by the District Leprosy Officer.
- As on January 2017: 115 recognized RCS centres (61 Government + 54 NGO) in the country.
14. INFORMATION, EDUCATION AND COMMUNICATION (IEC/BCC)
- IEC strategy during 12th plan: Focus on communication for behavioural change against stigma and discrimination.
- Key messages:
- Availability of MDT
- Correction of deformity through surgery
- Leprosy-affected person can live a normal life with the family
- Research into basic problems of leprosy carried out at:
- Central JALMA Institute of Leprosy, Agra
- Central Leprosy Teaching and Training Institute (CLTRI), Chingelput, Chennai
- Regional Training and Referral Institutes at Aska (Odisha), Raipur (Chhattisgarh), Gouripur (West Bengal)
15. ILEP AGENCIES
-
International Federation of Anti-Leprosy Associations (ILEP) is actively involved as partner in NLEP.
-
In India, ILEP is constituted by 10 agencies:
- The Leprosy Mission
- Damien Foundation of India Trust
- Netherland Leprosy Relief
- German Leprosy Relief Association
- Lepra India
- ALES
- AIFO
- Fontilles-India
- AERF-India
- American Leprosy Mission
-
ILEP provides support in: planning, monitoring & supervision, capacity building, IEC, RCS services, and socio-economic rehabilitation.
-
36 NGOs conducting RCS for disability correction are supported by ILEP.
-
54 NGOs getting grant-in-aid from Government of India under SET scheme.
16. NLEP ACTIVITIES AT PHC LEVEL (Under NHM)
Essential:
- Health education to community regarding leprosy
- Diagnosis and management of leprosy and its complications including reactions
- Training of leprosy patients having ulcers for self-care
- Counselling for leprosy patients for regularity/completion of treatment and prevention of disability
Source: Park's Textbook of Preventive and Social Medicine, Chapter - National Health Programmes (pp. 476-482, 1004)
National strategic plan and roadmapfor leprosy 2023-2027? The 5 pillars? Include them give as whole at one place...
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Searching the Web
National Strategic Plan Roadmap Leprosy 2023-2027 India 5 pillars NLEP
Reading Web Page
https://dghs.mohfw.gov.in/nlep.php
Reading Web Page
https://dhs.kerala.gov.in/wp-content/uploads/2024/01/Website…
Searching the Web
NSP leprosy 2023-2027 pillar 2 accelerate case detection pillar 3 quality services pillar 4 prevention stigma pillar 5 digital surveillance detailed components
I have comprehensive content. Let me now compile the complete ordered answer.
Important note before you read: The National Strategic Plan and Roadmap for Leprosy 2023-2027 was released on 30th January 2023. This content is NOT in Park's textbook (the current edition predates this document). For your University LAQ exam, this is supplementary/updated content from the official Government of India NSP document itself. I am clearly flagging this so you are not confused - Park's textbook covers NLEP up to the 12th Plan period; the NSP 2023-2027 is a newer government document you must read alongside it.
NATIONAL STRATEGIC PLAN AND ROADMAP FOR LEPROSY 2023-2027
Released: 30th January 2023 (World Leprosy Day)
Developed by: Committee of over 80 experts in leprosy, in consultation with national experts, WHO, and key stakeholders
Alignment: WHO Global Leprosy Strategy 2021-2030 + WHO NTD Roadmap 2021-2030 + SDG 3.3
VISION
"Leprosy Free India with Zero infection and disease, Zero disability, Zero stigma and discrimination"
GOAL
Accelerate towards achieving Interruption of Leprosy Transmission in India by 2027 (3 years ahead of the SDG 3.3 target of 2030)
SPECIFIC OBJECTIVES (5)
- Strengthen leadership, commitment, and partnerships
- Acceleration of Case Detection
- Provision of Quality Services
- Enhanced measures for Prevention of Disease, Disabilities, Stigma, Discrimination and Violation of Human Rights
- Digitalization of Surveillance Systems
ROADMAP PHASES (Timeline 2023-2027)
| Phase | Years | Focus |
|---|---|---|
| Phase 1 | 2023-2025 | Acceleration - Accelerated case finding + Quality services to all patients |
| Phase 2 | 2025-2026 | Sustained Momentum with Surveillance - Sustain gains, continue surveillance, sustain expertise, targeted active case detection |
| Phase 3 | 2026-2027 | Continued efforts and Targeted Interventions for interruption of transmission - Move towards zero leprosy |
NSP TARGETS 2023-2027
| Indicators | 2022-23 | 2023-24 | 2024-25 | 2025-26 | 2026-27 |
|---|---|---|---|---|---|
| New Leprosy Cases | 1,15,000 | 1,10,000 | 80,000 | 65,000 | 50,000 |
| Child Cases | 6,000 | 5,000 | 4,000 | 2,000 | 1,000 |
| Child Percentage | 5.21% | 4.5% | 5% | 3.07% | 2% |
| Grade 2 Disability per million | 1.7 | 1.8 | 1.2 | 1 | 0.5 |
THE FIVE STRATEGIC PILLARS
PILLAR 1: STRENGTHEN LEADERSHIP, COMMITMENT, AND PARTNERSHIPS
Key components:
- Enduring political commitment at national, state, and district levels
- Creation of customized state and UT-specific roadmaps
- Ensure availability of dedicated programme managers at national, state, and high-burden district level
- Resource mapping, pooling, and redistribution at national, state, and district levels
- Increase investment at central and state levels for acceleration and coverage
- Training of healthcare service providers at least once in 3 years; fill up vacant positions under the programme
- Involvement of AYUSH for NLEP
- Launch of Guidelines for AMR (Anti-Microbial Resistance) Surveillance for Leprosy
- Introduction of molecular testing for early diagnosis - specifically for confirming leprosy in early atypical cases
- Emphasis on disease and AMR surveillance; implementation of both international and domestic research
- Socio-economic rehabilitation of persons affected by leprosy
- Engagement with development partners (WHO, ILEP, NGOs)
PILLAR 2: ACCELERATE CASE DETECTION
Key components:
- Raise community awareness and actively search for new leprosy cases
- Methods of detection:
- Focused Leprosy Campaigns (FLC)
- ASHA-Based Surveillance for Leprosy Suspects (ABSULS) - launched 1st July 2019, strengthens case finding at grassroots level
- Leprosy Case Detection Campaigns (LCDC)
- Coordination with other national health programmes for case detection
- Retrospective contact tracing and reverse contact tracing
- Follow-up with tracked contacts - carried out twice a year for 5 years to check for any signs of leprosy
- Leprosy screening integrated with:
- Rashtriya Bal Swasthya Karyakram (RBSK) - for screening children 0-18 years
- Rashtriya Kishore Swasthya Karyakram (RKSK)
- Skin camps and house-to-house surveys in endemic areas
- Carry out household contact surveys involving ASHA for early detection
- Special plans for hard-to-reach areas (naxalite zones, difficult terrains)
- Post-Exposure Prophylaxis (PEP) administered to eligible contacts of index cases to interrupt chain of transmission
- Grade 2 Deformity Case Investigation (G2D): All new G2D cases investigated within 15 days of reporting
PILLAR 3: PROVIDE QUALITY AND COMPREHENSIVE SERVICES
Key components:
- Complete and timely MDT (Multi-Drug Therapy) for all detected cases - free of cost
- Treatment of leprosy reactions - prevent disability
- DPMR (Disability Prevention and Medical Rehabilitation):
- Reconstructive surgery for deformities
- Provision of Micro-Cellular Rubber (MCR) chappals/footwear
- Aids and appliances (wheelchairs, crutches, goggles, etc.) - all provided free of cost
- Ulcer care and self-care kits
- Patient-centric, rights-based approach to leprosy care
- Quality services at all levels - sub-centre, PHC, CHC, district hospital
- Nikusth 2.0 - web-based online reporting system with patient tracking mechanism launched in 2023:
- Patient records management
- Drug stock management
- Digital reporting
- Training of Medical Officers, Health Workers, Para-Medical Workers, ASHA workers
- Sensitization of Anganwadi workers, tribal promoters, educated youth in high-risk communities
- Incentive to patient: Rs. 8,000/- for major reconstructive surgery (irrespective of financial status)
- 115 recognized RCS centres (61 Government + 54 NGO) for reconstructive surgeries
PILLAR 4: PREVENTION OF DISEASE, DISABILITIES, STIGMA, DISCRIMINATION, AND VIOLATION OF HUMAN RIGHTS
Key components:
A. Prevention of Disease:
- Post-Exposure Prophylaxis (PEP) - administered to eligible contacts to limit disease transmission
- Early case detection before Grade 2 disability sets in
B. Prevention of Disability:
- Early intervention and expanded surveillance
- Grade 2 Deformity Case Investigation within 15 days of reporting
- Physiotherapy, ulcer care, reconstructive surgery, MCR footwear
C. Reduction of Stigma and Discrimination:
- Sparsh Leprosy Awareness Campaign (2017) - through Gram Sabhas, Panchayat, and Village Health and Sanitation Community; 60% of total villages covered
- SLAC (Sub-national Leprosy Awareness Campaign) - Theme for 2025-26: "Together, let us raise awareness, dispel misconceptions and ensure that no one affected by leprosy is left behind"
- Sapna - a concept/mascot: a common school-going girl in the community who helps spread awareness through key IEC messages; can be any local girl willing to be 'Sapna'
- IEC/BCC (Behaviour Change Communication) activities:
- Promote self-reporting
- Target early case detection
- Community pledge not to discriminate against persons affected by leprosy
- IEC posters at high visibility places
- Awareness through gram sabhas, school health education, community meetings
- Intensive IEC campaign with theme "Towards Leprosy Free India"
D. Human Rights:
- Rights-based approach - persons affected by leprosy receive care, protection, and dignity
- Anti-discrimination advocacy at community and policy levels
PILLAR 5: DEVELOP DIGITAL SURVEILLANCE SYSTEMS FOR NLEP (DIGITALIZATION)
Key components:
- Aligned with Ayushman Bharat Digital Health Mission (ABDM)
- NLEP committed to making patient-related reporting, recording, and logistics management fully digital, real-time, and web-based
- Nikusth 2.0 - digital case-based data management system:
- Launched in 2023
- Patient tracking mechanism
- Drug stock management
- Online reporting system
- Roll-out of digitalized case-based data management
- Mapping of cases shall be introduced
- Integration of reporting on IHIP (Integrated Health Information Platform)
- "Whole-of-government" and "whole-of-society" approach along with digital surveillance tools and strong institutional memory
APPROACH OF THE NSP
The NSP promotes a patient-centric, rights-based approach. It focuses on:
- (a) Promotion of self-reporting
- (b) Targeted early case detection
- (c) Collaboration with partners
- (d) Introduction of Anti-Microbial Resistance (AMR) surveillance to achieve zero leprosy by 2030
KEY INITIATIVES UNDER NSP 2023-2027
- NSP and Roadmap 2023-27 + National Guidelines for AMR for Leprosy - released together on 30th January 2023
- Contact tracing + PEP - for eligible contacts of index cases to interrupt transmission chain
- Leprosy Case Detection Campaign (LCDC) - active case detection in rural and urban areas through ASHAs and frontline workers
- ABSULS - ASHA-Based Surveillance for Leprosy Suspects
- Nikusth 2.0 - digital reporting system for patient records and drug stock management (2023)
- G2D Investigation - all Grade 2 Deformity cases investigated within 15 days
- RBSK and RKSK integration - leprosy screening of children 0-18 years
- Integration of leprosy services into Health and Wellness Centres (HWCs)
SDG TARGETS FOR LEPROSY BY 2030
Under SDG 3.3: End epidemics of neglected tropical diseases by 2030. India's specific SDG leprosy targets:
- Reduce Prevalence Rate (PR) to less than 0.1/10,000 population at district, block, and Panchayat level
- Reduce child cases of leprosy from 1.17/million to < 0.6/million
- Rate of child case with zero disability to be sustained
- Grade 2 deformity from 1.2/million to < 1/million
Sources: National Strategic Plan and Roadmap for Leprosy 2023-2027 (GOI, MoHFW, NLEP); DGHS official NLEP page; NLR India Foundation - NSP document; Clinical Dermatology Review - Zero Leprosy Strategic Plans.
This is a shared conversation. Sign in to Orris to start your own chat.